
Abstract
Background
Alport syndrome is one of the most common inherited kidney diseases worldwide. A genetic test or kidney biopsy is necessary for a definite diagnosis of this disease, and an accurate diagnosis system for this disease is highly desired in each country. However, the current situation in Asian countries is not clear. Therefore, the tubular and inherited disease working group of the Asian Pediatric Nephrology Association (AsPNA) aimed to assess the current situation of diagnosis and treatment for Alport syndrome in Asia.
Methods
The group conducted an online survey among the members of AsPNA in 2021–2022. Collected data included the number of patients for each inheritance mode, availability of gene tests or kidney biopsy, and treatment strategies for Alport syndrome.
Results
A total of 165 pediatric nephrologists from 22 countries in Asia participated. Gene test was available in 129 institutes (78%), but the cost was still expensive in most countries. Kidney biopsy was available in 87 institutes (53%); however, only 70 can access electron microscopy, and 42 can conduct type IV collagen α5 chain staining. Regarding treatment, 140 centers use renin-angiotensin system (RAS) inhibitors (85%) for Alport syndrome patients.
Conclusions
This study result might suggest that the system is underdeveloped enough to diagnose all Alport syndrome patients in most Asian countries. However, once diagnosed with Alport syndrome, most of them were treated with RAS inhibitors. These survey results can be used to address knowledge, diagnostic system, and treatment strategy gaps and improve the Alport patients’ outcomes in Asian countries.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
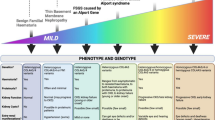
Recently, the natural history of Alport syndrome has been reported, including registry-based and cross-sectional studies [1,2,3,4,5]. Most of them are from European countries, America, and part of Asian countries, including Japan, China, and Korea. In those countries, a comprehensive gene testing system for this disease has already been established, so accurate diagnosis of this disease is relatively easy. For the diagnosis of Alport syndrome, either a gene test or kidney biopsy is necessary [6]. In addition, for the pathological diagnosis, we need to find either abnormal glomerular basement membrane (GBM) changes, such as diffuse basket-weave changes by electron microscopy or abnormal expression of type IV collagen α5 chain (α5(IV)) by immunohistochemistry.
Recently, it has been clarified from both prospective and retrospective studies that renin-angiotensin system (RAS) inhibitors treatment can reduce the urinary protein level and delay the development of end-stage kidney disease (ESKD) remarkably [5, 7,8,9]. Therefore, an accurate and early diagnosis system for this disease is highly desired in each country to improve the prognosis of patients with Alport syndrome. However, the current situation in Asian countries is not clear. Therefore, the tubular and inherited disease working group of the Asian Pediatric Nephrology Association (AsPNA) aimed to assess the current status of diagnosis and treatment for Alport syndrome in Asian countries.
We have previously conducted a survey of the current status of pediatric tubular and inherited disorders in Asia as a first step [10]. The results highlight the diversity of disease prevalence, diagnostic practices, capability, and access to genetic tests across Asia. This time, we conducted the survey only for Alport syndrome to reveal the availability of a genetic test and kidney biopsy, including access to electron microscopy and α5(IV) staining. In addition, we asked the doctors about the treatment strategies. The data gathered from this survey can be used to address knowledge gaps and improve management and outcomes in Asian countries.
Methods
Survey development and conduct
We developed a web-based survey that included the following information (Supplementary data 1): (1) total patient numbers of Alport syndrome in each inheritance mode following at each institute. (2) Accessibility of gene test. If yes, we also asked about the cost of the gene test. (3) Availability of kidney biopsy. If yes, we also asked about the accessibility to electron microscopy and α5(IV) staining availability. (4) Treatment strategies, especially RAS inhibitor treatment. Using the Google platform or its equivalent for China, the final survey was administered by sending the link using the valid e-mail addresses of members of the AsPNA from October 2021 to April 2022. In centers with more than one nephrologist, we asked them to reply to only one representative doctor. Completion of the survey implied consent to participation. The survey closed on the last day of April 2022. Respondents did not receive remuneration for participating in this survey.
Ethics
This study did not require human subjects or sensitive data covered by the data privacy act; we sought for waiver of consent.
Results and discussion
As for the first survey covering many kinds of inherited kidney diseases, the results highlight the diversity of disease prevalence, diagnostic practices, capability, and access to genetic tests across Asia [10]. This second survey which focused on Alport syndrome again revealed the diversity of diagnostic strategies for this disease.
We received responses from 165 pediatric nephrologists and 165 institutes (academic; 110, public; 31, and private; 24) from 22 Asian countries (Table 1). Japan (n = 55), China (n = 40), and India (n = 14) have the most significant number of survey participants. In total, 1240 Alport syndrome patients were followed up in these institutes; 532 were male X-linked Alport syndrome (XLAS), 322 were female XLAS, 105 were autosomal recessive Alport syndrome (ARAS), and 84 were autosomal dominant Alport syndrome (ADAS).
Although most of the institutes (78%) had access to gene tests in Asian countries, most of them sent genomic DNA samples to foreign countries except for China, India, Iran, Japan, Korea, and Thailand. In that case, gene tests are costly (100–2000 USD). The ‘genetic first approach’ was defined as a diagnostic approach of directly conducting gene tests before kidney biopsy when physicians see patients with hematuria and a family history of chronic kidney diseases (CKD). This is a common approach among responders in Malaysia, China and Japan.
As for kidney biopsy, it is available in about half of the institutes (54%) in Asian countries; however, most of the institutes, except for some countries, do not have access to type IV collagen α5 staining (26%) or electron microscopy (43%). These two items are indispensable for the pathological diagnosis of Alport syndrome without which a definite pathological diagnosis of this disease is impossible [6].
Regarding treatment, almost all pediatric nephrologists use renin-angiotensin system (RAS) inhibitors. Some of them still use cyclosporine, which is currently considered more harmful than beneficial in this disease [11, 12]. Doctors in Asian countries tend to hesitate to start RAS inhibitor treatment for suspected but not definitely diagnosed Alport syndrome patients. To the consensus of our working group, patients with hematuria and proteinuria who are not yet diagnosed should be started RAS inhibitor treatment because it benefits the patients more than harms them.
Of course, this study has many limitations that must be addressed. 1. The survey only included members of the AsPNA, and thus it may have yet to capture the actual burden of the diseases in Asia. However, it was very difficult to obtain detailed data such as what percentage of pediatric nephrologists in each country have answered the survey. 2. We asked separately for the patient number and availabilities for gene tests and kidney biopsy. So we still need to get the information on how many patients were diagnosed by these tools. It means the proportion of the inheritance mode needs to be more reliable. 3. Although most of the institutes have access to gene tests, it is expensive, and only some suspected patients can have gene tests, but we have yet to ask what proportion of the patients have conducted gene tests. Therefore, in the future survey, we should have revealed how many patients are correctly diagnosed based on genetic tests. 4. We have not yet investigated the precise method of RAS inhibitor treatment for Alport syndrome patients. In a further study, we need to know the age of start taking RAS inhibitors and their efficacy.
Clinical practice guidelines published in Western countries are not always applicable to Asians. The most significant difference with Western countries is the complete lack of diagnostic systems in most Asian countries. Fortunately, RAS inhibitors are not expensive medicines, and may be recommended to start these drugs even for suspected Alport syndrome patients but not a definitive diagnosis because the benefits of treatment with these agents outweigh the drawbacks to these patients. Therefore, Asia-specific clinical practice guidelines should be developed for rapid, correct diagnosis and treatment to improve disease outcomes suitable to this particular group. The aim of this study was to solve the knowledge gap and improve the management and outcomes of Alport syndrome in Asia. To bridge the gaps in the knowledge of the disease, diagnostic practices, and access to genetic tests, a network for broader collaborations is needed in undertaking prospective research studies. Free webinars for these countries should be planned by AsPNA.
In conclusion, the results highlight that the availability of gene tests or kidney biopsies for diagnosing Alport syndrome is needed in Asian countries. This result might suggest that the system is underdeveloped enough to save all Alport syndrome patients. However, once diagnosed with Alport syndrome, most of them were treated with RAS inhibitors. These survey results can be used to address knowledge, diagnosis system, and treatment strategy gaps and improve the Alport patients’ outcomes in Asian countries.
References
Jais JP, Knebelmann B, Giatras I, De Marchi M, Rizzoni G, Renieri A, Weber M, Gross O, Netzer KO, Flinter F, Pirson Y, Dahan K, Wieslander J, Persson U, Tryggvason K, Martin P, Hertz JM, Schroder C, Sanak M, Carvalho MF, Saus J, Antignac C, Smeets H, Gubler MC. X-linked Alport syndrome: natural history and genotype-phenotype correlations in girls and women belonging to 195 families: a “European Community Alport syndrome concerted action” study. J Am Soc Nephrol. 2003;14:2603–10.
Jais JP, Knebelmann B, Giatras I, Marchi M, Rizzoni G, Renieri A, Weber M, Gross O, Netzer KO, Flinter F, Pirson Y, Verellen C, Wieslander J, Persson U, Tryggvason K, Martin P, Hertz JM, Schroder C, Sanak M, Krejcova S, Carvalho MF, Saus J, Antignac C, Smeets H, Gubler MC. X-linked Alport syndrome: natural history in 195 families and genotype- phenotype correlations in males. J Am Soc Nephrol. 2000;11:649–57.
Mallett A, Tang W, Clayton PA, Stevenson S, McDonald SP, Hawley CM, Badve SV, Boudville N, Brown FG, Campbell SB, Johnson DW. End-stage kidney disease due to Alport syndrome: outcomes in 296 consecutive Australia and New Zealand dialysis and transplant registry cases. Nephrol Dial Transplant. 2014;29:2277–86.
Yamamura T, Nozu K, Fu XJ, Nozu Y, Ye MJ, Shono A, Yamanouchi S, Minamikawa S, Morisada N, Nakanishi K, Shima Y, Yoshikawa N, Ninchoji T, Morioka I, Kaito H, Iijima K. Natural history and genotype-phenotype correlation in female X-linked Alport syndrome. Kidney Int Rep. 2017;2:850–5.
Zhang Y, Bockhaus J, Wang F, Wang S, Rubel D, Gross O, Ding J. Genotype-phenotype correlations and nephroprotective effects of RAAS inhibition in patients with autosomal recessive Alport syndrome. Pediatr Nephrol. 2021;36:2719–30.
Nozu K, Nakanishi K, Abe Y, Udagawa T, Okada S, Okamoto T, Kaito H, Kanemoto K, Kobayashi A, Tanaka E, Tanaka K, Hama T, Fujimaru R, Miwa S, Yamamura T, Yamamura N, Horinouchi T, Minamikawa S, Nagata M, Iijima K. A review of clinical characteristics and genetic backgrounds in Alport syndrome. Clin Exp Nephrol. 2019;23:158–68.
Gross O, Licht C, Anders HJ, Hoppe B, Beck B, Tonshoff B, Hocker B, Wygoda S, Ehrich JH, Pape L, Konrad M, Rascher W, Dotsch J, Muller-Wiefel DE, Hoyer P, Study Group Members of the Gesellschaft fur Padiatrische N, Knebelmann B, Pirson Y, Grunfeld JP, Niaudet P, Cochat P, Heidet L, Lebbah S, Torra R, Friede T, Lange K, Muller GA, Weber M. Early angiotensin-converting enzyme inhibition in Alport syndrome delays renal failure and improves life expectancy. Kidney Int. 2012;81:494–501.
Gross O, Tonshoff B, Weber LT, Pape L, Latta K, Fehrenbach H, Lange-Sperandio B, Zappel H, Hoyer P, Staude H, Konig S, John U, Gellermann J, Hoppe B, Galiano M, Hoecker B, Ehren R, Lerch C, Kashtan CE, Harden M, Boeckhaus J, Friede T, German Pediatric Nephrology Study G, Investigators EP-TA. A multicenter, randomized, placebo-controlled, double-blind phase 3 trial with open-arm comparison indicates safety and efficacy of nephroprotective therapy with ramipril in children with Alport’s syndrome. Kidney Int. 2020;97:1275–86.
Yamamura T, Horinouchi T, Nagano C, Omori T, Sakakibara N, Aoto Y, Ishiko S, Nakanishi K, Shima Y, Nagase H, Takeda H, Rossanti R, Ye MJ, Nozu Y, Ishimori S, Ninchoji T, Kaito H, Morisada N, Iijima K, Nozu K. Genotype-phenotype correlations influence the response to angiotensin-targeting drugs in Japanese patients with male X-linked Alport syndrome. Kidney Int. 2020;98:1605–14.
Real Resontoc L, Kandai N, Hooman N, Vasudevan A, Ding J, Kang H. Pediatric tubular and inherited disorders in asia: results of preliminary survey of the asian pediatric nephrology association (aspna) tubular and inherited working group. Asian J Pediatric Nephrol. 2022;5:14–20.
Sugimoto K, Fujita S, Miyazawa T, Nishi H, Enya T, Izu A, Wada N, Sakata N, Okada M, Takemura T. Cyclosporin A may cause injury to undifferentiated glomeruli persisting in patients with Alport syndrome. Clin Exp Nephrol. 2014;18:492–8.
Massella L, Muda AO, Legato A, Di Zazzo G, Giannakakis K, Emma F. Cyclosporine A treatment in patients with Alport syndrome: a single-center experience. Pediatr Nephrol. 2010;25:1269–75.
Funding
Open access funding provided by Kobe University.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Nozu, K., Resontoc, L.P.R., Hooman, N. et al. Investigation of the current situation regarding diagnosis and treatment of Alport syndrome in Asian countries: results of survey of the Asian Paediatric Nephrology association (AsPNA) tubular and inherited working group. Clin Exp Nephrol 27, 776–780 (2023). https://doi.org/10.1007/s10157-023-02358-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-023-02358-6