
Abstract
Objective
This study aimed to evaluate the effectiveness of robot-assisted gait training (RAGT) in treating lower extremity function in patients with cerebral palsy (CP) and compare the efficacy differences between different robotic systems.
Methods
PubMed, Web of Science, Cochrane Library, Embase, CNKI, VIP, CBM, and Wanfang databases were searched to collect randomized controlled trials of RAGT for lower extremity dysfunction in patients with CP from the time the databases were created until December 26, 2022. The D and E of Gross Motor Function Measure-88 (GMFM-88) assessed lower limb motor function. Berg Balance Scale (BBS) was used to assess balance function. Walking endurance and speed were assessed using the 6-minute walk test (6MWT) and walking speed. The modified Ashworth Scale (MAS) was used to assess the degree of muscle spasticity in the lower extremities. The Cochrane Risk Assessment Scale and the Physiotherapy Evidence Database (PEDro) scale were used for qualitative assessment in the studies included. RevMan 5.4 was used for data merging and statistical analysis. R 4.2.0 and ADDIS 1.16.8 were used to map the network relationships and to perform the network meta-analysis.
Results
A total of 14 studies were included in the review. The meta-analysis showed that RAGT significantly improved GMFM-88 D and E, BBS, and 6MWT scores in CP patients compared with conventional rehabilitation. However, for walking speed and MAS, the intervention effect of RAGT was insignificant. The network meta-analysis showed that the best probability ranking for the effect of the 3 different robots on the GMFM-88 D score was LokoHelp (P = 0.66) > Lokomat (P = 0.28) > 3DCaLT (P = 0.06) and the best probability ranking for the GMFM-88 E score was LokoHelp (P = 0.63) > 3DCaLT (P = 0.21) > Lokomat (P = 0.16).
Conclusion
RAGT positively affects walking and balance function in patients with CP, while efficacy in improving gait speed and muscle spasticity is unknown. The best treatment among the different robots is LokoHelp. Future high-quality, long-term follow-up studies are needed to explore the clinical efficacy of RAGT in depth.
Similar content being viewed by others

Introduction
Cerebral palsy (CP) is a neurodevelopmental disorder caused by damage to the brain during early development and is characterized clinically by postural and motor dysfunction [1]. Motor dysfunction due to CP is often accompanied by sensory, perceptual, cognitive, communication, and behavioral deficits, as well as epilepsy and secondary musculoskeletal problems [2]. The different clinical features of CP can be divided into spastic, irregular, ataxic, and mixed CP [3]. The prevalence of CP is between 0.20 and 0.35% of surviving infants, and the number of people with CP is currently 17 million worldwide [4]. About 40% of these patients cannot walk independently, which seriously affects their activities of daily living [5]. Clinical rehabilitation interventions for CP patients mainly include neurodevelopmental therapy, physiotherapy, and hydrotherapy, which have achieved some success but are less effective in treating walking and balance functions [6].
Robot-assisted gait training (RAGT) is a new rehabilitation intervention that facilitates repetitive and efficient walking training with external mechanical assistance [7,8,9]. Lerner found that a robotic exoskeleton improved knee range of motion in patients with spastic CP [10]. Borggraefe trained 20 children with CP on a robot-assisted treadmill for 3 weeks, and they showed significant improvements in standing and walking function [11]. Digiacomo showed that RAGT combined with conventional treatment improved motor performance and endurance in children with CP [12].
However, the number of studies is small, outcome indicators and treatment effects vary, clinical effectiveness remains controversial, and there needs to be more high-quality evidence of evidence-based medicine to support this [13, 14]. Network meta-analysis is a statistical method that quantifies several interventions and prioritizes interventions’ effects based on different outcome indicators. In this study, we used the network meta-analysis method to search randomized controlled trials (RCTs) of RAGT for CP patients, extract relevant outcome indicators to evaluate their efficacy, and compare the differences in the efficacy of different robotic devices to provide evidence-based references for the clinical application of RAGT training.
Methods
This study was registered on the international system evaluation registration platform PROSPERO (CRD42022366471).
Search strategy
PubMed, Web of Science, Cochrane Library, Embase, CNKI, VIP, CBM, and Wanfang databases were searched by two researchers using medical mesh words and free words from the establishment of the database to December 26, 2022. The search formula is as follows: #1 “robot-assisted gait training” [MeSH] OR robot OR robotics OR RAGT, #2 “cerebral pals*” [MeSH] OR spastic quadriplegia OR spastic diplegia OR spastic hemiplegia OR CP, #3, #1, and #2. The condition was limited to a randomized controlled trial. Cross-check the results after the search, and discuss the decision with the third researcher in case of disagreement.
Inclusion criteria
The following are the inclusion criteria:
Study design—Chinese and English RCTs.
Participants—children aged <18 years with a precise diagnosis of CP, regardless of gender and race; the child is conscious, has a reasonable level of intelligence, and can cooperate with treatment and follow-up.
Intervention and control measures—the intervention group received RAGT combined with conventional rehabilitation, while the control group received conventional rehabilitation.
Outcome indicators—the primary outcome measures were Gross Motor Function Measure-88 (GMFM-88) D (standing and standing) and E (walking and running and jumping). The secondary outcome measures were the Berg Balance Scale (BBS), 6-minute walk test (6MWT), walking speed, and Modified Ashworth Scale (MAS).
Data—the experimental data are complete and provide sample sizes, means, and standard deviations within groups.
Exclusion criteria
Exclusion criteria are as follows: literature from non-randomized controlled trials; animal studies; conference abstracts, duplicate studies; incomplete outcome data; selective reporting studies; unavailable full text; literature not in Chinese or English.
Study selection and data extraction
Two researchers carried out the search, screening, and collation of the literature and the extraction of data and information independently, and the results were cross-checked after completion. In case of disagreement, a third researcher was assigned to decide. Data extraction included the first author, year of publication, basic information about the study population (sample size, age), basic information about the interventions (interventions, duration of treatment, follow-up, type of robot), and outcome indicators.
Quality assessment
Two researchers assessed the risk of bias in the included literature according to the Cochrane Risk Assessment Scale and the Physiotherapy Evidence Database (PEDro) scale. The third researcher discussed the decision in any disagreement between the two researchers.
Statistical analysis
RevMan 5.4 was used for meta-analysis. The data types of the outcome indicators for this meta-analysis were all measures. The standard mean difference (SMD) and its 95% confidence interval (CI) were used for statistical analysis of effect values. A fixed effect model was used to analyze if I2 ≤ 50% and P ≥ 0.1, indicating a small heterogeneity among the included studies. A random effect model was used for analysis if I2 > 50%, P < 0.1, indicating more significant heterogeneity between studies. Subgroup analysis or sensitivity analysis was used to identify sources of heterogeneity. The significance level α=0.05.
R 4.2.0 was used to make the network relationship map of the efficacy comparison of different robotic devices. ADDIS 1.16.8 was used for network meta-analysis. Since there is no closed loop in this study’s evidence relationship network graph, a consistency model was fitted to perform a probabilistic analysis of the outcome indicators. Four Markov chains were set, the initial value of the model was 2.5, the iteration step was fine-tuned by 10, and the number of iterations was 50,000, of which the first 20,000 were annealed to eliminate the effect of the initial value. The last 30,000 were used for sampling. The potential scale reduction factor (PSRF) was used to evaluate the convergence efficiency. The PSRF tends to be 1, indicating good convergence efficiency and high reliability of the network meta-analysis results. The rank-ranking probability diagram presented the probability of each intervention becoming the best intervention, and rank 1 was the best probability. The ranking of interventions’ superiority was based on the magnitude of the rank 1 value. The funnel plot was drawn using RevMan 5.4, and if the funnel plot was symmetrical, it suggested that the possibility of publication bias was low.
Results
Study selection and characteristics
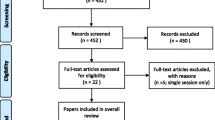
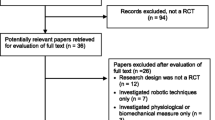
According to the literature search strategy, 428 studies were obtained from the initial search. After excluding 192 duplicate publications, the remaining 236; after reading the titles and abstracts, 204 were excluded, and the remaining 32. After carefully reading the complete text, 14 studies were finally included, including 8 in Chinese [15,16,17,18,19,20,21,22] and 6 in English [23,24,25,26,27,28], with a total of 654 patients. The process of literature screening is shown in Fig. 1. The essential characteristics of the included studies are shown in Table 1.

Screening process of literature selection
Quality and risk of bias assessment
All studies mentioned “random” or “randomized grouping,” but two studies [21, 23] did not specify the specific randomized scheme. Two studies [25, 27] used opaque envelopes to complete allocation hiding, while the remaining studies did not mention allocation sequence hiding. One study [24] blinded the treatment, and four studies [23,24,25, 28] were blinded to outcome assessors. The data results included in the literature were complete and not reported selectively. One study [26] had another bias. Nine included studies [16, 18, 19, 23,24,25,26,27,28] were of high quality, and five [15, 17, 20,21,22] were of moderate quality, with a mean score of 7.14. The results of the quality assessment of the included studies are shown in Fig. 2 and Table 2.

Risk assessment of bias
Meta-analysis
GMFM-88 D score
Nine studies [16, 18,19,20,21,22, 24, 26, 27] reported GMFM-88 D scores. Heterogeneity tests suggested significant heterogeneity among studies (I2 = 57%, P = 0.02), and a random effect model was used to combine effect sizes. Overall, the GMFM-88 D score was higher in the experimental group than in the control group (SMD = 0.84, 95% CI 0.54 to 1.15, P < 0.05) (Fig. 3). Subgroup analysis showed that GMFM-88 D scores were significantly higher in both the LokoHelp and Lokomat groups than in the control group (SMD = 1.14, 95% CI 0.89 to 1.40, P < 0.05 and SMD = 0.71, 95% CI 0.20 to 1.23, P < 0.05). However, the difference between the 3DCaLT and control groups was insignificant (SMD = −0.11, 95% CI −0.97 to 0.75, P > 0.05).

Effects of RAGT on GMFM-88 D scores of patients with CP
GMFM-88 E score
Nine studies [16, 18,19,20,21,22, 24, 26, 27] reported GMFM-88 E scores. Heterogeneity tests suggested significant heterogeneity among studies (I2 = 68%, P = 0.002), and a random effect model was used to combine effect sizes. Overall, GMFM-88 E scores were significantly higher in the experimental group than in the control group (SMD = 0.78, 95% CI 0.43 to 1.14, P < 0.05) (Fig. 4). Subgroup analysis showed that GMFM-88 E scores were higher in both the LokoHelp and Lokomat groups than in the control group (SMD = 0.88, 95% CI 0.31 to 1.46, P < 0.05 and SMD = 0.80, 95% CI 0.28 to 1.32, P < 0.05). However, there was no significant difference between the 3DCaLT and control groups (SMD = 0.13, 95% CI −0.73 to 0.99, P > 0.05).

Effects of RAGT on GMFM-88 E scores of patients with CP
BBS
Five studies [15,16,17,18, 22] reported BBS scores. Heterogeneity tests suggested significant heterogeneity among studies (I2 = 71%, P = 0.009), and a random effect model was used to combine effect sizes. Overall, BBS scores were higher in the experimental group than in the control group (SMD = 0.91, 95% CI 0.50 to 1.32, P < 0.05) (Fig. 5). Subgroup analysis showed that BBS scores were higher in both the LokoHelp and Lokomat groups than in the control group (SMD = 1.00, 95% CI 0.51 to 1.50, P < 0.05 and SMD = 0.57, 95% CI 0.09 to 1.04, P < 0.05).

Effects of RAGT on BBS scores of patients with CP
6MWT
Three studies [21, 25, 27] reported the results of the 6MWT evaluation. Heterogeneity tests suggested no significant heterogeneity among studies (I2 = 0%, P = 0.75), and a fixed effect model was used to combine effect sizes. Overall, the results of the 6MWT evaluation were higher in the experimental group than in the control group (SMD = 0.67, 95% CI 0.18 to 1.15, P < 0.05) (Fig. 6). Subgroup analysis showed that 6MWT evaluation results were higher in the 3DCaLT group than in the control group (SMD = 0.91, 95% CI 0.00 to 1.82, P = 0.05). 6MWT evaluation results in both the Lokomat and Gait Trainer 1 group were not statistically significant compared to the control group (SMD = 0.66, 95% CI −0.07 to 1.40, P > 0.05 and SMD = 0.41, 95% CI −0.53 to 1.35, P > 0.05).

Effects of RAGT on 6MWT of patients with CP
Walking speed
Four studies [17, 23, 26, 27] reported walking speed (m/s) in patients with CP after treatment. Heterogeneity tests suggested no significant heterogeneity among studies (I2 = 0%, P = 0.49), and a fixed effect model was used to combine effect sizes. Overall, the walking speed of patients in the experimental group was higher than that of the control group. The difference between the experimental and control groups was not statistically significant (SMD = 0.31, 95% CI −0.08 to 0.71, P > 0.05) (Fig. 7).

Effects of RAGT on the walking speed of patients with CP
MAS
Five studies [15, 17, 18, 27, 28] reported MAS scores. Heterogeneity tests suggested significant heterogeneity among studies (I2 = 93%, P < 0.00001), and a random effect model was used to combine effect sizes. Overall, the MAS scores were lower in the experimental group than in the control group. The difference between the experimental and control groups was not statistically significant (SMD = −0.67, 95% CI −1.75 to 0.41, P > 0.05) (Fig. 8).

Effects of RAGT on MAS scores of patients with CP
Network meta-analysis
Evidence network
The GMFM-88 E score, more closely related to lower limb motor function, was used to compare the efficacy of different robotic. Of the studies reporting GMFM-88 E scores, four studies [16, 18,19,20] used the LokoHelp rehabilitation robot (RECK Company), four studies [21, 22, 24, 26] used the Lokomat children's version rehabilitation robot (HOCOMA Company), and one study [27] used 3DCaLT robot device. The network relationship is shown in Fig. 9 (a, LokoHelp; b, Lokomat; c, 3DCaLT; d, control).

The network relationship of efficacy Comparison of different robot
Consistency test
There was no closure of the loop between interventions in this study. Therefore, consistency testing was not required.
Convergence diagnosis
A convergence diagnosis of the included studies revealed bandwidth values close to 0, suggesting good convergence (Fig. 10).

Track density map of the GMFM-88 E score
Probability ranking
The network meta-analysis revealed that the best ranking of probabilities for the effect of 3 different robots on GMFM-88 D scores was LokoHelp (P = 0.66) > Lokomat (P = 0.28) > 3DCaLT (P = 0.06) and the best ranking of probabilities for the GMFM-88 E score was LokoHelp (P = 0.63) > 3DCaLT (P = 0.21) > Lokomat (P = 0.16) (Fig. 11, Fig. 12, Table 3).

Rank of GMFM-88 D scores

Rank of GMFM-88 E scores
Adverse reaction
One study [17] reported that RAGT training caused a small number of patients to experience mild discomfort from rubbing the skin on the inner root of the thigh from wearing the robot device, which was relieved by rest and did not interfere with the next day’s treatment. No adverse effects were reported in other studies.
Subgroup analysis of primary outcomes
GMFM-88 D and E scores were analyzed in subgroups according to the intervention time and patient age. The analysis results generally follow the above analysis (Table 4).
Sensitivity analysis
The meta-analysis results were analyzed for sensitivity using a one-by-one exclusion method, removing one study at a time. The results showed no significant change from the above results, indicating that the meta-analysis results were relatively stable.
Publication bias
No significant asymmetry was seen in the funnel plot of the study with GMFM-88 D and E scores as outcome indicators. It is suggested that the results of data analysis are less influenced by publication bias (Fig. 13).

Funnel plot
Discussion
Lower limb motor dysfunction is one of the most common symptoms in patients with CP [29, 30], leading to an inability to walk or abnormal gait patterns, such as horseshoe foot or crouching gait [31]. It can cause secondary injuries and have a severe impact on the quality of life of patients. Therefore, the balance of lower limbs and walking functions are essential in rehabilitating patients with CP [32, 33]. RAGT, as an emerging rehabilitation therapy, brings new hope for the functional rehabilitation of CP patients [34]. This study analyzed the literature on RAGT for lower limb motor function in patients with CP using a network meta-analysis. We compared the clinical efficacy of different robotic devices.
The meta-analysis showed that RAGT training improved GMFM-88 D and E area scores, BBS scores, and 6MWT significantly better than conventional rehabilitation in CP patients. However, the effect of improved gait speed and lower limb muscle spasticity is unclear. The network meta-analysis results showed that RAGT improved lower limb motor function in CP patients, with LokoHelp most likely to improve lower limb motor function to a greater extent in CP patients.
Central nervous system plasticity theory and motor learning theory, closely related to the reconstruction of brain cell function, suggest that repetitive movements can induce plastic changes in the brain. Neural plasticity changes are primarily realized by rebuilding neural networks [35,36,37,38]. The therapeutic mechanism of RAGT on lower limb motor function in patients with CP may be related to the improvement of nervous system plasticity [39]. Shin showed that repetitive RAGT training promotes functional network reorganization in the brain’s motor cortex and stimulates neuroplasticity [40]. Youssofzadeh found that RAGT training significantly improved functional network connectivity around the sensory-motor areas of the brain and enhanced functional connectivity between the prefrontal and parietal lobes after EEG analysis in healthy subjects [41].
The following limitations exist in this study: the total number of subjects included in the literature was small; some of the literature was not allocation sequence concealed and blinded, which may lead to a potential risk of bias; there were age differences in the study population and varying severity of the condition, which may have had an impact on the rehabilitation outcome; the frequency and periodicity of interventions varied in the literature, which may have biased the findings; some of the literature had short treatment periods.
Conclusion
In conclusion, RAGT training improved the motor function of the lower limbs of CP patients, with LokoHelp probably having the best treatment effect. This positively impacted the patient’s quality of life, balance function, and motor control. However, the evidence for the efficacy of RAGT in improving gait speed and muscle spasticity is insufficient and needs further exploration. In addition, the small sample size of the literature included in this study and the variable quality of the articles may have impacted the analysis results. Therefore, adequate sample size and high-quality and long-term follow-up studies are still needed to explore the clinical efficacy of RAGT in depth.
Data availability
The data used to support the findings of this study are available from the corresponding author upon request.
References
Graham HK, Rosenbaum P, Paneth N, Dan B, Lin JP, Damiano DL, Becher JG, Gaebler-Spira D, Colver A, Reddihough DS et al (2016) Cerebral palsy. Nat Rev Dis Primers 2:15082. https://doi.org/10.1038/nrdp.2015.82
Sadowska M, Sarecka-Hujar B, Kopyta I (2020) Cerebral palsy: current opinions on definition, epidemiology, risk factors, classification and treatment options. Neuropsychiatr Dis Treat 16:1505–1518. https://doi.org/10.2147/ndt.S235165
Schwabe AL (2020) Comprehensive care in cerebral palsy. Phys Med Rehabil Clin N Am 31:1–13. https://doi.org/10.1016/j.pmr.2019.09.012
Subspecialty Group of Rehabilitation, the Society of Pediatrics, Chinese Medical Association (2020) Rehabilitation strategy and recommendation for motor dysfunction in children with cerebral palsy. Chin J Pediatr 58:91–95. https://doi.org/10.3760/cma.j.issn.0578-1310.2020.02.005
Korzeniewski SJ, Slaughter J, Lenski M, Haak P, Paneth N (2018) The complex aetiology of cerebral palsy. Nat Rev Neurol 14:528–543. https://doi.org/10.1038/s41582-018-0043-6
Xiong HC, Chen JH, Wang J, Zhu DN, Xiao N, Zhou YP, Zhou ZH, Tang GH, Yang YH (2021) Effects of robot-assisted gait training on the gross motor and balance function of children with spastic cerebral palsy. J Zhengzhou Univ Med Sci 56:370–375. https://doi.org/10.13705/j.issn.1671-6825.2020.12.112
Peri E, Turconi AC, Biffi E, Maghini C, Panzeri D, Morganti R, Pedrocchi A, Gagliardi C (2017) Effects of dose and duration of robot-assisted gait training on walking ability of children affected by cerebral palsy. Technol Health Care 25:671–681. https://doi.org/10.3233/thc-160668
Ammann-Reiffer C, Bastiaenen CHG, Meyer-Heim AD, van Hedel HJA (2020) Lessons learned from conducting a pragmatic, randomized, crossover trial on robot-assisted gait training in children with cerebral palsy (PeLoGAIT). J Pediatr Rehabil Med 13:137–148. https://doi.org/10.3233/prm-190614
Jin LH, Yang SS, Choi JY, Sohn MK (2020) The effect of robot-assisted gait training on locomotor function and functional capability for daily activities in children with cerebral palsy: a single-blinded, randomized cross-over trial. Brain Sci 10:801. https://doi.org/10.3390/brainsci10110801
Lerner ZF, Damiano DL, Park HS, Gravunder AJ, Bulea TC (2017) A robotic exoskeleton for treatment of crouch gait in children with cerebral palsy: design and initial application. IEEE Trans Neural Syst Rehabil Eng 25:650–659. https://doi.org/10.1109/tnsre.2016.2595501
Borggraefe I, Schaefer JS, Klaiber M, Dabrowski E, Ammann-Reiffer C, Knecht B, Berweck S, Heinen F, Meyer-Heim A (2010) Robotic-assisted treadmill therapy improves walking and standing performance in children and adolescents with cerebral palsy. Eur J Paediatr Neurol 14:496–502. https://doi.org/10.1016/j.ejpn.2010.01.002
Digiacomo F, Tamburin S, Tebaldi S, Pezzani M, Tagliafierro M, Casale R, Bartolo M (2019) Improvement of motor performance in children with cerebral palsy treated with exoskeleton robotic training: a retrospective explorative analysis. Restor Neurol Neurosci 37:239–244. https://doi.org/10.3233/rnn-180897
Lobato Garcia L, González González Y, Da Cuña Carrera I, Alonso Calvete A (2020) Benefits of robotics in gait rehabilitation in cerebral palsy: a systematic review. Rehabilitacion (Madr) 54:128–136. https://doi.org/10.1016/j.rh.2020.01.004
Guo HB, Zhou X, Du Q (2021) Research progress of lower limb rehabilitation robot in improving the walking ability of children with cerebral palsy. Chin J Rehabil 36:376–379. https://doi.org/10.3870/zgkf.2021.06.013
Ye N, Fan QH, Chen ZH, Wu TT, Shen LF (2020) Influence study of lower limb robot-assisted gait training on rehabilitation effects and quality of life of children patients with cerebral palsy. Chin Med Equip 17:94–97. https://doi.org/10.3969/J.ISSN.1672-8270.2020.11.023
Lv N, Shang Q, Ma CY, Li JJ, Zhang QM (2017) Rehabilitation effect of rehabilitation robot on children with spastic cerebral palsy. Chin J Pract Nerv Dis 20:45–47. https://doi.org/10.3969/j.issn.1673-5110.2017.07.018
Yin ZL, Meng ZX, Xue YJ, Ren SW, Jin X (2017) Effects of rehabilitation robot-assisted walking training on walking ability in adult patients with cerebral palsy. Chin J Rehabil Med 32:97–99. https://doi.org/10.3969/j.issn.1001-1242.2017.01.022
Zhang RJ (2018) Rehabilitation robot-assisted walking training on lower limb muscle tone in children with cerebral palsy. Chin J Pract Med 45:99–101. https://doi.org/10.3760/cma.j.issn.1674-4756.2018.13.032
Zhu MJ (2016) Observation of curative effect by rehabilitation robot in rehabilitation therapy for cerebral palsy children. Chin Pract Med 11:283–284. https://doi.org/10.14163/j.cnki.11-5547/r.2016.29.191
Jin X, Meng ZX, Yin ZL, Zhang XB, Wang JB, Fan ZL, Chen B, Ke MH (2012) The effects of robot-aided walking training on the walking ability in children with cerebral palsy. Chin J Rehabil Med 27:822–824. https://doi.org/10.3969/j.issn.1001-1242.2012.09.008
Ma TT, Zhang H (2021) Effect of robotic-assisted gait training on motor and walking for children with spastic cerebral palsy. Chin J Rehabil Theory Pract 27:1260–1265. https://doi.org/10.3969/j.issn.1006-9771.2021.11.004
Zheng HC, Wang Q, Yang L (2021) Effect of lower limb robot combined with exercise thera. Clin Res Pract 6:166–168. https://doi.org/10.19347/j.cnki.2096-1413.202133053
Drużbicki M, Rusek W, Snela S, Dudek J, Szczepanik M, Zak E, Durmala J, Czernuszenko A, Bonikowski M, Sobota G (2013) Functional effects of robotic-assisted locomotor treadmill thearapy in children with cerebral palsy. J Rehabil Med 45:358–363. https://doi.org/10.2340/16501977-1114
Klobucká S, Klobucký R, Kollár B (2020) Effect of robot-assisted gait training on motor functions in adolescent and young adult patients with bilateral spastic cerebral palsy: a randomized controlled trial. Neurorehabil 47:495–508. https://doi.org/10.3233/nre-203102
Smania N, Bonetti P, Gandolfi M, Cosentino A, Waldner A, Hesse S, Werner C, Bisoffi G, Geroin C, Munari D (2011) Improved gait after repetitive locomotor training in children with cerebral palsy. Am J Phys Med Rehabil 90:137–149. https://doi.org/10.1097/PHM.0b013e318201741e
Wallard L, Dietrich G, Kerlirzin Y, Bredin J (2018) Effect of robotic-assisted gait rehabilitation on dynamic equilibrium control in the gait of children with cerebral palsy. Gait Posture 60:55–60. https://doi.org/10.1016/j.gaitpost.2017.11.007
Wu M, Kim J, Arora P, Gaebler-Spira DJ, Zhang Y (2017) Effects of the integration of dynamic weight shifting training into treadmill training on walking function of children with cerebral palsy: a randomized controlled study. Am J Phys Med Rehabil 96:765–772. https://doi.org/10.1097/phm.0000000000000776
Yaşar B, Atıcı E, Razaei DA, Saldıran TÇ (2021) Effectiveness of robot-assisted gait training on functional skills in children with cerebral palsy. J Pediatr Neurol 20:164–170. https://doi.org/10.1055/s-0041-1725128
Bartels EM, Korbo L, Harrison AP (2020) Novel insights into cerebral palsy. J Muscle Res Cell Motil 41:265–267. https://doi.org/10.1007/s10974-020-09577-4
Wu M, Kim J, Gaebler-Spira DJ, Schmit BD, Arora P (2017) Robotic resistance treadmill training improves locomotor function in children with cerebral palsy: a randomized controlled pilot study. Arch Phys Med Rehabil 98:2126–2133. https://doi.org/10.1016/j.apmr.2017.04.022
Goldstein M, Harper DC (2001) Management of cerebral palsy: equinus gait. Dev Med Child Neurol 43:563–569. https://doi.org/10.1111/j.1469-8749.2001.tb00762.x
Roostaei M, Akbarfahimi N, Dalvand H, Abedi S (2021) The relationship between functional motor status and self-evaluation in individuals with cerebral palsy: a systematic review. Iran J Child Neurol 15:9–27. https://doi.org/10.22037/ijcn.v15i4.26438
Wilson JL, Kim YM, O'Malley JA, Gelineau-Morel R, Gilbert L, Bain JM, Aravamuthan BR (2022) Cerebral palsy in child neurology and neurodevelopmental disabilities training: an unmet need. J Child Neurol 37:194–201. https://doi.org/10.1177/08830738211072711
van Hedel HJA, Severini G, Scarton A, O'Brien A, Reed T, Gaebler-Spira D, Egan T, Meyer-Heim A, Graser J, Chua K et al (2018) Advanced Robotic Therapy Integrated Centers (ARTIC): an international collaboration facilitating the application of rehabilitation technologies. J Neuroeng Rehabil 15:30. https://doi.org/10.1186/s12984-018-0366-y
Wiart L, Rosychuk RJ, Wright FV (2016) Evaluation of the effectiveness of robotic gait training and gait-focused physical therapy programs for children and youth with cerebral palsy: a mixed methods RCT. BMC Neurol 16:86. https://doi.org/10.1186/s12883-016-0582-7
Dayan E, Cohen LG (2011) Neuroplasticity subserving motor skill learning. Neuron 72:443–454. https://doi.org/10.1016/j.neuron.2011.10.008
Xie ZC, Tang JK (2006) Analysis of training techniques for the functional rehabilitation of cerebral palsy. Chin J Clin Rehabil 10:128–130. https://doi.org/10.3321/j.issn:1673-8225.2006.24.056
Li L, Huang H, Jia Y, Yu Y, Liu Z, Shi X, Wang F (2021) Systematic review and network meta-analysis of noninvasive brain stimulation on dysphagia after stroke. Neural Plast 2021:3831472. https://doi.org/10.1155/2021/3831472
de Oliveira RMW (2020) Neuroplasticity. J Chem Neuroanat 108:101822. https://doi.org/10.1016/j.jchemneu.2020.101822
Shin J, Yang S, Park C, Lee Y, You SJH (2022) Comparative effects of passive and active mode robot-assisted gait training on brain and muscular activities in sub-acute and chronic stroke. Neurorehabil 51:51–63. https://doi.org/10.3233/nre-210304
Youssofzadeh V, Zanotto D, Wong-Lin K, Agrawal SK, Prasad G (2016) Directed functional connectivity in fronto-centroparietal circuit correlates with motor adaptation in gait training. IEEE Trans Neural Syst Rehabil Eng 24:1265–1275. https://doi.org/10.1109/tnsre.2016.2551642
Author information
Authors and Affiliations
Contributions
YW conceived the theme of the study. YW, PZ, and CL performed the systematic search, reviewed the literature, and extracted the data. YW analyzed data and wrote the first draft of the paper. PZ checked and modified the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wang, ., Zhang, P. & Li, C. Systematic review and network meta-analysis of robot-assisted gait training on lower limb function in patients with cerebral palsy. Neurol Sci 44, 3863–3875 (2023). https://doi.org/10.1007/s10072-023-06964-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-023-06964-w