
Abstract
Objectives: To assess the potential of immersive virtual reality (IVR) in achieving moderate exercise intensity, and 2) to examine the acute effects of two IVR exergame sessions (BOXVR and Beat Saber), comparing them with the impact of traditional exercise on heart rate variability (HRV), perceived effort, delayed onset muscle soreness, motivation, and sleep. Materials and methods: A crossover design was used. The participants (n = 22) randomly performed two sessions of IVR and one session of moderate intensity physical activity, each session lasting 30 min. Heart Rate (HR) and HRV, Perceived Exertion Scale, Intrinsic Motivation Inventory, sleep quality, and perceived pain, were evaluated. Results: The cardiac response to the activities was significantly higher when participants performed traditional physical activity as compared to the BOXVR and Beat Saber games. Traditional training provided a different HRV response as compared to Beat Saber (LnRMSSD, p = 0.025; SDNN, p = 0.031). Although the sessions were planned for moderate intensity, BOXVR generated a moderate intensity (49.3% HRreserve), Beat Saber (29.6% HRreserve) a light one, and the Circuit session, a vigorous one (62.9% HRreserve). In addition, traditional training reported higher perceived exertion and pain with less enjoyment. Differences were observed between the exergames. BOXVR resulted in a lower cardiac response (HRmax and HRmean), and a higher perception of exertion and pain at 72 h. The sleep variables analyzed were not altered by any of the sessions. Conclusions: BOXVR and traditional training can lead to moderate intensity physical activity. However, traditional training could result in lower adherence to physical exercise programs, as it was perceived as more intense and less enjoyable.
Similar content being viewed by others

1 Introduction
In the last few years, sedentarism has become a risk factor associated to diseases such as hypertension, Type-2 diabetes, and even different types of cancer (Arocha Rodulfo 2019). Previous studies have indicated that the increase in sedentary behaviors in the general population is due, in part, to the technological development in the last 20 years, mainly because of the arrival of products such as tablets, smartphones, or gaming consoles. This phenomenon has been named “digital sedentarism” (Panadero-Pérez et al. 2019). The use of these products has resulted in a substantial decrease in the levels of physical activity performed by the general population (Lozano-Sánchez et al. 2019).
Despite the many studies that underline the health benefits derived from performing physical exercise (Lavie et al. 2019), the World Health Organization (WHO) estimates that 80% of adolescents and 25% of adults worldwide are physically inactive (Bull et al. 2020). A recent study conducted by Qian et al. (2020) (Qian, McDonough, and Gao 2020) indicated that one of the main reasons for the lack of sufficient physical levels of the population is that they conceived it as a boring and a difficult task to perform. Also, to obtain the benefits derived from physical exercise, the activity must reach minimum levels of intensity. According to the American College of Sports Medicine (ACSM)(Garber et al. 2011), adults must perform at least 5 days of moderate intensity (64–76% of the maximum heart rate [%HRmax] or 40–59% of the heart rate reserve [%HRR]), 30 min per day, for a total of 150 min per week. In this context, to reach the minimum requirements of physical activity considered healthy, new exercise modalities are needed that are more attractive to the population. Thus, adherence to physical activity has become vitally important, with motivation being a key aspect that influences the start, maintenance, and even abandonment of physical exercise (Rivera-Torres et al. 2019). Along this line, Thin et al. (2013) (Thin, Brown, and Meenan 2013) showed that modalities that are considered pleasurable increase participation in the long term.
Within the technological development cited above, the world of videogames has grown tremendously in the past few years, becoming an attractive type of entertainment (Thin, Brown, and Meenan 2013), and it is consumed by 53% of the European population, or 58% of the population in the United States (Polechoński, Dȩbska, and Dȩbski 2019). Despite most games not having physical demands by the player, more active games are becoming more popular, such as the exergames (Garcia et al. 2016; Peng, Lin, and Crouse 2011), videogames in which the objective of the game is to perform physical activity, and which require body movements of the player.
In the last few years, due to the appearance of virtual reality, and the objective of health improvement, a fusion of videogames with virtual reality has been produced, in which the player is immersed in a highly realistic world, in a visual and auditory environment that makes the player part of the game, increasing the emotions experienced. This fusion is named immersive virtual reality (IVR). Recent studies have shown that physical exercise through virtual reality can decrease the level of effort perceived, through enjoyment, which would increase one’s willingness towards doing more exercise (Düking et al. 2018), improving the psychological aspects and increasing exercise adherence in the long term (Qian, McDonough, and Gao 2020). In addition, fully IVR systems can contribute to muscle-strengthening activities for healthy users (Feodoroff et al. 2019).
Although some studies have suggested that IVR is a valid modality for achieving the minimum guidelines of physical activity proposed by some associations, such as the ACSM (Miyachi et al. 2010a; O’Donovan and Hussey 2012a), as far as we know, no studies have been conducted that analyzed the effects of this type of training on psycho-physical variables such as heart rate, perceived effort, delayed onset muscle soreness, motivation, or sleep, and which also compared it with traditional methods of exercise. Also, whether or not the recommended intensities of physical exercise during physical activity proposed by the WHO can be achieved through the use of IVR, is under question.
Given the above, the objectives of the study were: (1) to assess the potential of immersive virtual reality in achieving moderate exercise intensity recommended by the WHO, and (2) to examine the acute effects of two immersive virtual reality exergame sessions, comparing them with the impact of traditional exercise on heart rate variability, perceived effort, delayed onset muscle soreness, motivation, and sleep. The main hypothesis of the study is that physical exercise with virtual reality is valid when reaching the minimum intensity defined by the World Health Organization. The secondary hypothesis is that motivation, interest, and effort will be greater in the physical exercise sessions performed with virtual reality as compared to the traditional training session, while the effort perceived will be less in the virtual reality sessions as compared with the traditional session. As for the quality of sleep and delayed onset muscle soreness, it is expected that the traditional session will decrease their levels, as compared with the virtual reality session. Lastly, it is expected that the variability of heart rate will show acute differences between sessions, due to the greater demand of the sympathetic system in the IVR sessions.
2 Materials and methods
2.1 Design
A randomized and comparative crossover study was conducted to test the effects of three physical activity sessions performed with immersive virtual reality (IVR, games: BOXVR [BOX] and Beat Saber [BS]) and traditional physical activity (moderate-intensity circuit training [C]) on heart rate (HR), heart rate variability (HRV), sleep quality, and perceived enjoyment, effort, exertion, and pain. Participants performed the physical sessions in the morning, at the same time of the day (± 1 h) to minimize differing responses due to circadian rhythm changes. The study was approved by the University of XXX Ethics Committee and was in accordance with the Declaration of Helsinki.
2.2 Participants
A non-probability convenience sampling method was used for sample selection. For the sample size, an a priori sample size estimation was performed using G*Power statistical power software v.3.1.9.7. For this purpose, we established an α value of 0.05, a power of 80%, an effect size of 0.8 (Cohen’s d = large) and a Nonsphericity correction of 1. In addition, following Hopkins’ recommendations, sample size estimates for prospective studies and controlled trials should be inflated by 10–30% to account for dropouts (Hopkins 2006). The final estimated sample was 23 participants. Recruitment was conducted through the instant messaging application for smartphones WhatsApp (Meta Platforms, Inc, Menlo Park, California, USA). The messages were sent to those who a priori met the eligibility criteria, a total of 113 people, and 37 participants declared their interest to voluntarily enroll in the study. Participants had to be between 18 and 40 years old, available to complete the 3 sessions of physical activity, willing, and cognitively able to provide a written informed consent. The exclusion criteria were as follows: (a) participants were unable to perform moderate/intensive physical activity, (b) injuries to the musculoskeletal system and/or history of pulmonary, cardiovascular, metabolic diseases. Participants were instructed to maintain a regular diet and hydration and not to ingest caffeine or alcohol for at least 24 h prior to each physical activity session to ensure that the data obtained were due to the physical activity sessions alone. A demanding training session during the 48 h prior to each test was not allowed.
2.3 Procedures
In visit 1, participants were familiarized with all test procedures and the different intervention conditions (virtual reality games and traditional physical exercise). In addition, the sequence of the physical activity sessions was randomized (BOX, BS, and C). Before the physical activity sessions, the participants read and signed an informed consent document, completed a physical activity questionnaire (International Physical Activity Questionnaire, IPAQ) and height (m) and body mass (kg) were assessed according to the ISAK guidelines. The IPAQ (Roman-Viñas et al. 2010) is a validated and widely used tool for assessing physical activity levels in adults across various populations and contexts. IPAQ encompasses diverse dimensions of physical activity, including intensity, duration, and frequency of activities undertaken, thereby providing a comprehensive measure of physical behavior. Additionally, IPAQ facilitates the estimation of the volume of physical activity, quantified in metabolic equivalent of task minutes per week (METs/week). Participants returned a week later to begin the physical activity sessions. During the following 3 weeks, the participants completed a total of 3 physical activity sessions, two of them with immersive virtual reality (BOX and BS games), and one with moderate intensity circuit training (C). The order of the conditions for each session was randomized.
2.4 Physical activity sessions
The participants performed a standardized warm-up prior to each physical activity session (BOX, C or BS). The duration of each session was 5 min of warm-up followed by 30 min of physical activity.
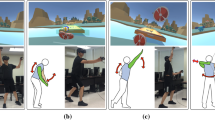
The virtual reality sessions (BOXVR and BS games) were conducted with the HMD Oculus Quest 2 and two controllers (Oculus VR, Menlo Park, CA, USA): (a) BOXVR game (FitXR, Perpetual Europe); the player’s avatar is two boxing gloves of different colors, and the player is placed in a scenario that simulates a gymnasium. The game requires the player to hit light spheres of the same color as the gloves, using different boxing punches such as the jab, the hook, and the uppercut, and to dodge blocks by bending and squatting to the rhythm of the music. The score changes according to the speed and trajectory with which the punch is performed. The game only admits an individual mode and the score obtained is recorded in an individual and world ranking. To match the duration of the virtual reality games, the session included 2 consecutive sets of 14 and 16 min respectively, and (b) Beat Saber game (indie Beat Games, Prague, Czech Republic); the participant is immersed in a tunnel, where cubes appear that must be cut in half, and in which obstacles must be avoided to the rhythm of the music and different visual effects. The cubes are colored with two different colors and carry an arrow that indicates the direction in which they must be cut with two lightsabers of the same color as the cubes (the player’s avatar). The game allows single or multiplayer mode, for playing against other users, with the score recorded for ranking oneself both at a personal and global level. For the development of this session, 8 songs were chosen, ordered from less to more difficult depending on the number of blocks per second to cut, and the “no lives” option was selected to finish each song and fail without any penalty (Table 1). Figure 1 shows the interface of the two immersive virtual reality games and virtual reality device used in the studio.

Interface of the two immersive virtual reality games and virtual reality device used in the studio. (a) BOXVR game, (b) Beat Saber games, (c) virtual reality device used in the studio
Regarding the physical activity circuit session, the participants completed a circuit (5 laps of 2 min, with 4 min active rest walking at a moderate speed per lap, total activity time: 30 min). The circuit consisted of a 6 m zigzag run (separation between cones of 1.2 m x 1.2 m), followed by a 1.6 m multi-jump with feet together (separation between rods of 0.4 m with a height of 0.18 m with respect to the ground), followed by going around a cone to change direction (180º), and a 7 m sprint to reach another cone to go around (90º) to reach the last part of the circuit, a 2.4 m stretch of strides (separation between hoops of the same lower limb of 1.2 m), to finish with 10 push-ups with knees resting on a mat placed 1.2 m from the last hoop to be overcome.
2.5 Testing procedures
The participants performed the testing measurements during and after physical session. The order of testing was the same for all three conditions, and each assessment was performed by the same researcher. The heart rate was monitored during each of the sessions. The participant’s Heart rate (HR) and Heart rate variability (HRV) were measured using a Polar H10 heart rate sensor chest strap (Polar Electro Oy, Kempele, Finland) and recorded at resting, one minute before the start of the different activities, during the session, and one minute after the end of the activity. Thus, a 32-minute measurement window was recorded for each session. The maximum (HRmax) and mean (HRmean) heart rate of each participant was obtained from the recorded data using the app Polar Beat for smartphone, HR reserve (%HRR) was calculated and categorized as follows: <30% indicating very light intensity, 30–39% indicating light intensity, 40–59% indicating moderate intensity, 60–89% indicating vigorous intensity, and ≥ 90% indicating near-maximal to maximal intensity, in accordance with the recommendations of the ACSM (Garber et al. 2011).
In addition, HRV was also analyzed using a smartphone application (Elite HRV™, Ashville, North Carolina, USA) (Moya-Ramon et al. 2022). The following HRV variables were evaluated: (I) ratio of low frequency (LF) to high frequency (HF) band; (II) total power (TP); (III) percentage of differences between adjacent normal R-R intervals > 50 ms (pNN50); (IV) square root of the mean of the sum of the squared differences between adjacent normal R-R intervals (RMSSD); (V) standard deviation of all NN intervals (SDNN); (VI) mean heart rate; and (VII) R-R mean intervals. The recording using the app was collected after each session of physical activity.
At the end of each session, the participants were asked to complete the modified Borg Rating of Perceived Exertion (RPE) Scale (Scale 0–10), and the interest-enjoyment and effort-importance scale (Intrinsic Motivation Inventory, IMI) (McAuley et al. 2013). The interest/enjoyment subscale is composed of 7 items (e.g., I really enjoyed doing this activity or I thought it was a boring activity) and the effort/importance subscale is composed of 5 items (e.g., I put a lot of effort into this game or it was important for me to do well at this game). All items are scored on a Likert scale ranging from strongly disagree (1) to strongly agree (7).
Additionally, the sleep quality (Karolinska Sleep Questionnaire) was measured after each training day, with a previous period of instruction to the participants. The participants were instructed to assess the subjective sleep quality in the morning after waking up, using the Karolinska Sleep Diary (KSD) (Akerstedt et al. 2016), which addresses the following aspects: (I) sleep quality; (II) sleep comfort; (III) ease of falling asleep; (IV) awakening; (V) ease of waking up; (VI) feeling of rest; (VII) Did you have enough sleep?.
Lastly, 72 h after the session, perceived pain was recorded using the Visual Analogue Scale (VAS) (Strøyer et al. 2007). It was used to register post-exercise soreness pain after 72 h, because the onset of clinical symptoms is usually delayed 48–72 h after the activity (Hotfiel et al. 2018). This scale ranges from 0 indicating no pain, to 10 indicating unbearable pain.
2.6 Statistical analyses
The statistical analyses were performed using the software Jamovi v. 2.3.2 (The jamovi project, Sidney, Australia). Descriptive analyses (mean and standard deviation) were calculated. For inferential analysis, the Shapiro–Wilk W-test was performed to establish the normality of the sampling distribution, and Mauchly’s W-test analyzed the sphericity between measurements. For those conditions where the sphericity assumption was not met, the Greenhouse-Geisser sphericity criterion was applied. Moreover, a repeated-measures analysis of variance (ANOVA; general linear model) was performed to analyze differences between physical activity sessions (BOX, C, BS) on outcomes. Post-hoc tests (Bonferroni) were performed when significant interaction effects were observed. Partial eta squared (η2p) for variance analysis was used to calculate the effect size, and Cohen’s d (ES) to evaluate the standardized difference between two means. A η2p of 0.1–0.24 indicated a small effect, 0.25–0.36 a medium effect, and ≥ 0.37 a large effect. In the pairwise comparison, Cohen’s d was calculated for related samples. The Cohen scale was used to delimit effect sizes, where 0.2 represents a small effect, 0.5 a moderate effect, and ≥ 0.8 a large effect (Cohen 1992). For all procedures, a level of p ≤ 0.05 was set to indicate statistical significance.
3 Results
Fifteen of the 37 participants who provided their signed consent did not start the study due to injury, incompatibility of schedules, illness, or personal reasons. Finally, twenty-two participants (male: 54.5%, age: 29.1 ± 7.8 years old, height: 1.74 ± 0.08 m, body mass: 70.4 ± 12.5 kg, body mass index: 23.3 ± 3.23 kg m− 2; METs/week: 2657.0 ± 2495.4) were involved in the study.
The results of the impact of different types of physical activity on HR are shown in Table 2. The ANOVA analysis showed significant main effects on HRmax (F = 76.1, η2p = 0.78, p < 0.001), HRmean (F = 73.0, η2p = 0.78, p < 0.001) and %HRR (F = 74.2, η2p = 0.78, p < 0.001).
In addition, higher HRmax, HRmean and %HRR (Fig. 2) were observed when participants performed physical activity in a circuit as compared to physical activity performed in IVR with the BOX (HRmax: ES = 1.6; HRmean: ES = 2.7 and %HRR: ES = 1.1) and BS (HRmax: ES = 2.7; HRmean: ES = 1.1 and %HRR: ES = 2.7) games. Likewise, the BOX physical activity resulted in a higher HRmax, HRmean and %HRR, as compared to BS (HRmax: ES = 1.1; HRmean: ES = 1.4 and %HRR: ES = 0.7).

Differences between different types of physical activity on Heart Rate (HR). The figure shows the observed scores as grey circles, the mean is represented by an unfilled circle and the error bars are expressed as the 95% confidence interval of the men. HRmax: Maximum heart rate; HRmean: Mean heart rate; %HRR: Percentage of reserve heart rate; BOX: BOXRV game; BPM: beat per minute; C: circuit-moderate training; BS: Beat Saber game; ***: p < 0.001
With respect to the heart rate variability (Table 3) a significant effect was observed on the SDNN (F = 4.1, η2p = 0.16, p = 0.023) and Mean R-R (F = 53.4, η2p = 0.72, p < 0.001). In this regard, the Bonferroni post hoc showed a higher SDNN when the physical activity was performed in a circuit as compared to BS (p = 0.010, ES = 0.6). In addition, the BS game led to a higher Mean R-R compared to C (p < 0.001, ES = 1.9) and BOX (p < 0.001, ES = 1.3). Nevertheless, the BOX game also led to a higher mean R-R as compared to C (p < 0.001, ES = 1.1).
Regarding the perception of the physical activity, significant main effects on enjoyment (F = 25.7, η2p = 0.55, p < 0.001), Borg scale (F = 127.0, η2p = 0.86, p = < 0.001) and the VAS scale (F = 26.5, η2p = 0.56, p < 0.001) were observed (Table 4). However, no statistically significant differences in effort/interest were observed between sessions.
The circuit training session showed less enjoyment as compared to the sessions conducted with IVR games (BOX: p < 0.001, ES = 1.8, BS: p = 0.003, ES = 0.8). No differences were observed between IVR games. In addition, the perception of exertion (Borg scale) and pain (VAS scale) was higher when performing the circuit session as compared to BOX (Borg: p < 0.001, ES = 2.0, VAS: p < 0.001, ES = 3.3) and BS (Borg: p = 0.001, ES = 0.9, VAS: p = 0.003, ES = 1.4) (Fig. 3). Nevertheless, the BOX game led a higher perception of exertion and pain as compared to the BS game (Borg: p < 0.001, ES = 1.3, VAS: p = 0.004, ES = 0.8).

Differences between different types of physical activity on enjoyment, exertion (Borg Scale) and pain (VAS scale) perception. The figure shows the observed scores as grey circles, the mean is represented by an unfilled circle and the error bars are expressed as the 95% confidence interval of the men. BOX: BOXRV game; C: circuit-moderate training; BS: Beat Saber game; **: p < 0.01; ***: p < 0.001
Regarding the quality of sleep analyzed with the Karolinska Sleep Questionnaire, a main effect was not observed in sleep quality (Table 5).
4 Discussion
The first aim of the present study was to assess the potential of immersive virtual reality in achieving moderate exercise intensity recommended by the WHO. In addition, the second aim of the present research was to examine the acute effects of two immersive virtual reality exergame sessions (BOXVR and Beat Saber), comparing them with the impact of traditional exercise on heart rate variability, perceived effort, delayed onset muscle soreness, motivation, and sleep. The main findings of the present study were: (i) the BOX session promoted moderate intensity exercise, but the BS session only demanded very light intensity; (ii) traditional exercise (C) provoked higher decreases in HRV than the IVR sessions; (iii) the IVR sessions were perceived as being more enjoyable that traditional circuit-based exercise; and (iv) similar sleep quality responses were reported after the three exercise sessions.
Regarding the cardiorespiratory recommendations, the ACSM guidelines recommend that adults should perform at least five days of moderate-intensity (40–59% HRreserve) aerobic exercise for ≥ 30 min per day for a total of ≥ 150 min per week, or at least three days per week of vigorous-intensity (60–89% HRreserve) cardiorespiratory exercise lasting ≥ 20 min, for a total of ≥ 75 min per week (Garber et al. 2011). According to the results obtained in the present study, the exercise intensity of each session was: BOX: moderate intensity (49.30 ± 12.11 HRreserve); C: vigorous intensity (62.90 ± 6.93 HRreserve); and BS (29.60 ± 11.41 HRreserve): very light intensity. Therefore, only C, as the traditional exercise session, and BOX, as the IVR session, fulfilled the exercise intensity suggested by ACSM recommendations. These findings were corroborated by the RPE scale results, as the self-reported intensity (BOX = ~ 4 or somewhat hard; C = ~ 7) or very hard; and BS = 2.6 or from easy to moderate) suggested the same intensity as the heart rate from each session. Furthermore, the higher delayed onset muscle soreness was clearly linked with the physiological intensity of the session, with higher values of soreness observed in the C session than in the two IVR ones, and in the BOX session as compared to in the BS one. The main explanation for these findings is related with the link between cardiovascular responses and the active muscle mass (Lewis et al. 1985), where a greater amount of exercised muscle mass produces a higher increase of cardiovascular responses (i.e. increase in heart rate, blood pressure) (Matos-Santos et al. 2017). In this way, the demonstrated linear relationship between heart rate and oxygen consumption during exercise, and consequently, energy expenditure(Achten and Jeukendrup 2003) suggest that the higher cardiovascular responses obtained in the C and BOX sessions promoted a higher expenditure of energy in these exercise sessions. Specifically, our findings are in agreement with previous studies with virtual games, which showed that some games (Wii Sports Boxing, Tennis and Baseball) were light-intensity activities, in terms of HR, but others (Wii Fit Free Jogging) can increase the intensity of the activity to moderate-intensity (O’Donovan and Hussey 2012b). In addition, Miyachi et al. (2010) (Miyachi et al. 2010b) confirmed that the lower energy and cardiovascular response in some virtual games was due to the lower horizontal locomotion involved in these types of the active video games. This justifies the findings obtained in the present study, where the BS game involved lower global movements (i.e. squat or dodge) than BOX (Table 1). Therefore, if the aim is to perform physical activity to fulfil ACSM guidelines, it is recommended that the IVR games used include global movements to obtain a moderate intensity. Studies such as the one developed by Xu et al. (2020) showed that seated exergames can be a good complement to standing exergames in increasing participant effort. Remarkably, some video games and IVR are recommended as physical activity tools (although they are not specifically designed for performing exercise) (Miyachi et al. 2010a; O’Donovan and Hussey 2012a), but not all of them have demonstrated their ability to meet the physical activity guidelines.
Immersive virtual reality can distract the athlete from negative symptoms during exercise (Rutkowski et al. 2021a) and produces a higher parasympathetic response in terms of HRV in an exercise performed at the same equivalent work without IVR (Rutkowski et al. 2021b). In this regard, the findings of the current study revealed reduced vagal activity during the traditional session compared to the BS session. This disparity is primarily attributed to the higher intensity of the traditional exercise, eliciting a heightened autonomic response to increased stress stimuli. Additionally, research indicates that a greater extent of exercised muscle mass contributes to an altered autonomic balance, resulting in diminished vagal activity (Matos-Santos et al. 2017). However, although, HRV analyses the stress produced by the stimulus on the autonomic nervous system, this tool does not analyze if the stress comes from physiological, cognitive, or emotional stress. Therefore, the IVR can modify the perceptual and cognitive stresses but, according to the results of the present study, the key factor that promotes a greater autonomic response is the exercise intensity. Thus, the IVR should include activities that increase exercise intensity to provoke a autonomic response similar to traditional exercise.
Adequate adherence is the key for achieving optimal benefits from physical activity intervention. To improve adherence, enjoyment has been considered as an important factor for increasing intrinsic motivation, and consequently, for performing more regular physical activity throughout one’s lifespan (Polechoński, Dȩbska, and Dȩbski 2019; Radhakrishnan et al. 2022). The results of the present study showed that the two IVR sessions were perceived as being more enjoyable that traditional circuit-based exercises (BOX: 6.3 ± 0.8; BS: 5.5 ± 1.3; C = 3.6 ± 1.5 of 7 points). Our results are in accordance with previous studies with virtual reality games that reported higher values of enjoyment in a cycling exercise in combination of IVR in comparison with the traditional cycle ergometer exercise (Farrow et al. 2018; Liu et al. 2019). The gamification of physical activity has been previously associated with higher values of enjoyment, and it can explain the findings of the present study (Dębska et al. 2019; Khundam and Nöel 2021; Mouatt et al. 2020; Tuveri et al. 2016). Therefore, IVR exercise, due to the higher enjoyment, may be used as an interesting tool in order to improve adherence to physical activity programs. However, the introduction of virtual reality in the realm of exercise brings a novel element that may foster increased short-term motivation. However, it’s crucial to acknowledge the uncertainty surrounding the long-term effects of this novelty, which necessitates examination through future studies and specific interventions. The sustainability of motivation over time could play a pivotal role, potentially leading to greater adherence to the exercise program, a critical aspect in long-term health promotion.
Sleep helps in the recovery process of the nervous system and metabolic cost imposed by the waking state (Nédélec et al. 2015). However, sleep problems and insomnia are increasingly reported in modern societies, affecting quality of life, decreasing mental and physical health (Halson 2016), and increasing the prevalence of some pathologies (i.e. sarcopenia) (Rubio-Arias et al. 2019). In addition, a positive relationship between sleep quality and academic performance in youth has been previously reported (Redondo-Flórez et al. 2022). In this way, previous studies reported that moderate physical activity enhanced sleep quality (Driver and Taylor 2000; Youngstedt and Kline 2006), but vigorous acute exercise affect sleep behavior, decreasing sleep quality and producing insomnia (Ramos-Campo et al. 2019). The results reported in the present study showed the lack of an effect of the exercise session (BOX, C or BS) on sleep quality. One possible reason that could explain why all the exercise sessions produced similar responses on these outcomes is related to the exercise characteristics, as the exercise volume of the three sessions was matched, and they only lasted 30 min. Moreover, the physiological and self-reported exercise intensity in all of them was lower than the previously reported, which produce adverse effects (insomnia and lower sleep quality) (Ramos-Campo et al. 2019). Finally, the three exercise sessions were performed in the morning, while negative effects were reported when the exercise sessions took place about 3 h before bedtime (Ramos-Campo et al. 2019). Therefore, the three types of exercise sessions proposed in the present study produced a similar sleep quality response in the participants.
Several strengths and limitations of this study warrant discussion. One of the strengths is the practical application of the results to the real world. Moreover, we acknowledge some limitations that must be taken into consideration in data interpretation. The assessment of the muscle soreness outcomes was only tested 72 h after the exercise was performed, and it should be measured also at the 24 and 48 h time points. Additionality, the inclusion of other biochemical markers (CK, LDH,…), and the assessment of other metabolic outcomes (VO2max, energy expenditure,…) could be interesting in future research to provide a more comprehensive picture of the use of IVR to fulfil physical activity recommendations. From a practical application point of view, if users or physical education educators want to utilize an IVR activity to achieve the ACSM recommendations, the IVR game should include global exercises (squats, punches, dodges…) and last at least 30 min. Future research should be conducted on specific IVR games that focus on physical activity sessions, to analyze the response to the game and the achievement of physical activity recommendations.
5 Conclusions
The data of the present study found that healthy adults that performed one immersive virtual reality boxing-based exercise session can fulfil the moderate intensity exercise recommended by the WHO’s physical activity guidelines. However, another immersive virtual reality experience based on the Beat Saber game only provided a very light intensity. Moreover, both immersive virtual reality exercises were performed at a lower intensity than a traditional circuit-based exercise designed to fulfil physical activity guidelines.
Additionally, traditional circuit-based exercise produced a greater decrease in HRV than the IVR sessions. Interestingly, the IVR sessions were perceived as more enjoyable that traditional exercise. Finally, similar sleep quality responses were reported after the three types of exercise sessions.
Data availability
The data that support the findings of this study are available from the corresponding author, LAC, upon reasonable request.
References
Achten J, Jeukendrup A (2003) Heart Rate Monitoring: Applications and limitations. Sports Med 33(7):517–538. https://doi.org/10.2165/00007256-200333070-00004
Akerstedt T, Hume K, Minors D et al (2016) The subjective meaning of good sleep, an Intraindividual Approach using the Karolinska Sleep Diary. Percept Mot Skills 79(1):287–926. https://doi.org/10.2466/PMS.1994.79.1.287
Arocha Rodulfo J (2019) Sedentarism, a Disease from Xxi Century. Clín Invest Arter 31(5):233–240. https://doi.org/10.1016/j.artere.2019.04.001
Bull FC, Al-Ansari SS, Biddle S, et al (2020). World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports M 54(24):1451–1462
Cohen J (1992) A power primer. Psychol Bull 112(1):155–159. https://doi.org/10.1037/0033-2909.112.1.155
Dębska M, Polechoński J, Mynarski A et al (2019) Enjoyment and intensity of physical activity in immersive virtual reality performed on innovative training devices in Compliance with recommendations for Health. Int J Envir Res Pub Heal 16(19):3673. https://doi.org/10.3390/IJERPH16193673
Driver HS, Taylor S (2000) Exercise and Sleep. Sleep Med Rev 4(4):387–402. https://doi.org/10.1053/SMRV.2000.0110
Düking P, Holmberg HC, Sperlich B (2018) The potential usefulness of virtual reality systems for athletes: a short SWOT analysis. Front Physiol 9:18. https://doi.org/10.3389/FPHYS.2018.00128
Farrow M, Lutteroth C, Rouse PC et al (2018) Virtual-reality Exergaming improves performance during high-intensity interval training. Eur J Sport Sci 19(6):719–727. https://doi.org/10.1080/17461391.2018.154245
Feodoroff B, Konstantinidis I, Froböse I (2019) Effects of full body exergaming in virtual reality on Cardiovascular and muscular Parameters: cross-sectional experiment. JMIR Serious Games 7(3). https://doi.org/10.2196/12324
Garber CE, Blissmer B, Deschenes MR et al (2011) Quantity and quality of Exercise for developing and maintaining Cardiorespiratory, Musculoskeletal, and Neuromotor Fitness in apparently healthy adults: Guidance for Prescribing Exercise. Med Sci Sports Exerc 43(7):1334–1359. https://doi.org/10.1249/MSS.0B013E318213FEFB
Garcia JA, Schoene D, Lord SR et al (2016) A Bespoke Kinect stepping Exergame for improving physical and cognitive function in older people: a pilot study. Games Health J 5(6):382–388. https://doi.org/10.1089/G4H.2016.0070
Halson SL (2016) Stealing sleep: is Sport or Society to blame?’. Br J Sports Med 50(7):381–381. https://doi.org/10.1136/BJSPORTS-2015-094961
Hopkins WG (2006) Estimating sample size for magnitude-based inferences. SprotScience 10:63–70
Hotfiel T, Freiwald J, Hoppe MW et al (2018) Advances in Delayed-Onset muscle soreness (DOMS): part I: Pathogenesis and Diagnostics. Sportverletzung-Sportschaden 32(4):243–250. https://doi.org/10.1055/A-0753-1884/ID/JR884-50
Khundam C, Nöel F (2021) A study of physical fitness and enjoyment on virtual running for Exergames. Int J Comput Games Technol. https://doi.org/10.1155/2021/6668280
Lavie CJ, Ozemek C, Carbone S et al (2019) Sedentary behavior, Exercise, and Cardiovascular Health. Circul Res 124(5):799–815. https://doi.org/10.1161/CIRCRESAHA.118.312669
Lewis SF, Snell PG, Taylor WF et al (1985) Role of muscle Mass and Mode of Contraction in circulatory responses to Exercise. J Appl Physiol 58(1):146–151. https://doi.org/10.1152/JAPPL.1985.58.1.146
Liu W, Zeng N, Pope ZC et al (2019) Acute effects of Immersive virtual reality Exercise on young adults’ situational motivation. J Clin Med. https://doi.org/10.3390/jcm8111947. 8:1947
Lozano-Sánchez AM, Zurita-Ortega F, Ubago-Jiménez JL et al (2019) Videogames, physical activity practice, obesity, and sedentary habits in Schoolchildren aged 10 to 12 Years Old in Th. Retos 35(35):42–46. https://doi.org/10.47197/RETOS.V0I35.61865
Matos-Santos L, Farinatti P, Borges J et al (2017) Cardiovascular responses to Resistance Exercise performed with large and small muscle Mass. Int J Sports Med 38(12):883–889. https://doi.org/10.1055/S-0043-116671/ID/R6176-0026
McAuley ED, Duncan T, Tammen VV (2013) Psychometric properties of the intrinsic motivation inventory in a competitive Sport setting: a confirmatory factor analysis’. Res Q Exerc Sport 60(1):48–58. https://doi.org/10.1080/02701367.1989.10607413
Miyachi M, Yamamoto K, Ohkawara K et al (2010) METs in adults while playing active Video games: a metabolic Chamber Study’. Med Sci Sports Exerc 42(6):1149–1153. https://doi.org/10.1249/MSS.0B013E3181C51C78
Mouatt B, Smith AE, Mellow ML et al (2020) The use of virtual reality to influence motivation, affect, enjoyment, and Engagement during Exercise: a scoping review. Front Virtual Real 1:564664. https://doi.org/10.3389/FRVIR.2020.564664/BIBTEX
Moya-Ramon MM, Mateo-March I, Peña-González M et al (2022) Validity and reliability of different smartphones applications to measure HRV during short and ultra-short measurements in Elite athletes. Comput Methods Programs Biomed 217:106696. https://doi.org/10.1016/J.CMPB.2022.106696
Nédélec M, Halson S, Abaidia AE et al (2015) Stress, sleep and recovery in Elite Soccer: a critical review of the literature’. Sports Med 2015 45(10):10. https://doi.org/10.1007/S40279-015-0358-Z
O’Donovan C, Hussey J (2012) Active Video games as a form of Exercise and the Effect of Gaming experience: a preliminary study in healthy young. Adults’ Physiotherapy 98(3):205–210. https://doi.org/10.1016/J.PHYSIO.2012.05.001
Organización Mundial de la Salud. Actividad Física. 24 (2023) https://www.who.int/es/news-room/fact-sheets/detail/physical-activity
Panadero-Pérez N, Ruiz-San Román BM, Joya-Barroso M et al (2019) Digital Sedentarism as a Precursor to the Deterioration of Health Adolescents and Young People. 2019(3):368–83
Peng W, Hsuan Lin J, Crouse J, Cyberpsychology (2011) Behav Social Netw 14(11):681–688. https://doi.org/10.1089/CYBER.2010.0578
Polechoński J, Dȩbska M, Paweł G et al (2019) Exergaming can be a health-related aerobic physical activity. BioMed Res Int 1890527. https://doi.org/10.1155/2019/1890527
Qian J, McDonough DJ, Gao Z et al (2020) The effectiveness of virtual reality Exercise on Individual’s physiological, psychological and rehabilitative outcomes: a systematic review. Int J Environ Res Public Health 17(11):4133. https://doi.org/.3390/IJERPH17114133
Radhakrishnan U, Chinello F, Koumaditis K (2022) Investigating the effectiveness of immersive VR skill training and its link to physiological Arousal. Virtual Reality 27(2):1091–1115. https://doi.org/10.1007/S10055-022-00699-3
Ramos-Campo DJ, Ávila-Gandía V, Luque AJ et al (2019) Effects of Hour of Training and Exercise Intensity on Nocturnal autonomic modulation and sleep quality of amateur Ultra-endurance Runner’. Physiol Behav 198:134–139. https://doi.org/10.1016/J.PHYSBEH.2018.10.020
Redondo-Flórez L, Ramos-Campo DJ, Clemente-Suárez VJ (2022) Relationship between physical fitness and academic performance in University students. Int J Environ Res Public Health 19(22):14750. https://doi.org/10.3390/IJERPH192214750
Rivera-Torres S, Fahey TD, Rivera MA (2019) Adherence to Exercise Programs in older adults: informative report. Gerontol Geriatr 5:2333721418823604. https://doi.org/10.1177/2333721418823604
Roman-Viñas B, Serra-Majem L, Hagströmer M et al (2010) International Physical Activity Questionnaire: Reliability and Validity in a Spanish Population. European Journal of Sport Science 10(5):297–304. https://doi.org/1080/17461390903426667
Rubio-Arias JÁ, Rodríguez-Fernández R, Andreu-Caravaca L et al (2019) Effect of Sleep Quality on the prevalence of Sarcopenia in older adults: a systematic review with Meta-analysis. J Clin Med 8(12):2156. https://doi.org/10.3390/JCM8122156
Rutkowski S, Szary P, Sacha J et al (2021) Immersive virtual reality influences physiologic responses to Submaximal Exercise: a randomized, crossover trial. Front Physiol 12:1679. https://doi.org/10.3389/FPHYS.2021.702266/BIBTEX
Strøyer J, Essendrop M, Donbæk L et al (2007) Validity and reliability of self-assessed physical fitness using Visual Analogue scales. Percept Mot Skills 104(2):519–533. https://doi.org/10.2466/PMS.104.2.519-533
Thin AG, Brown C, Meenan P et al (2013) User experiences while playing dance-based exergames and the influence of different body motion Sensing technologies. Int J Comput Games Technol 603604. https://doi.org/10.1155/2013/603604
Tuveri E, Macis L, Sorrentino F et al (2016) Fitmersive games: Fitness Gamification through Immersive VR. Proc Workshop Adv Visual Interfaces 1:212–215. https://doi.org/10.1145/2909132.2909287
Xu W, Ning Liang H, He Q et al (2020) JMIR Serious Games 8(3):1–12. https://doi.org/10.2196/17972. Results and Guidelines From a Repeated-Measures Design Experiment Comparing Standing and Seated Full-Body Gesture-Based Immersive Virtual Reality Exergames: Within-Subjects Evaluation
Youngstedt SD, Kline CE (2006) Epidemiology of Exercise and Sleep. Sleep Biol Rhythms 4(3):215. https://doi.org/10.1111/J.1479-8425.2006.00235.X
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rubio-Arias, J.Á., Verdejo-Herrero, A., Andreu-Caravaca, L. et al. Impact of immersive virtual reality games or traditional physical exercise on cardiovascular and autonomic responses, enjoyment and sleep quality: a randomized crossover study. Virtual Reality 28, 64 (2024). https://doi.org/10.1007/s10055-024-00981-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10055-024-00981-6