
Abstract
Objectives
To evaluate the diagnostic MRI compatibility of different fixed orthodontic retainers using a high-resolution 3D-sequence optimized for artifact reduction.
Materials and methods
Maxillary and mandibular retainers made of five different materials were scanned in vitro and in vivo at 3 T MRI using an MSVAT-SPACE sequence. In vitro, artifact volumes were determined for all maxillary and mandibular retainers (AVmax; AVmand). In vivo, two independent observers quantified the extent of artifacts based on the visibility of 124 dental and non-dental landmarks using a five-point rating scale (1 = excellent, 2 = good, 3 = acceptable, 4 = poor, 5 = not visible).
Results
Rectangular-steel retainers caused the largest artifacts (AVmax/AVmand: 18,060/15,879 mm3) and considerable diagnostic impairment in vivo (mean landmark visibility score ± SD inside/outside the retainer areas: 4.8 ± 0.8/2.9 ± 1.6). Smaller, but diagnostically relevant artifacts were observed for twistflex steel retainers (437/6317 mm3, 3.1 ± 1.7/1.3 ± 0.7). All retainers made of precious-alloy materials produced only very small artifact volumes (titanium grade 1: 70/46 mm3, titanium grade 5: 47/35 mm3, gold: 23/21 mm3) without any impact on image quality in vivo (each retainer: visibility scores of 1.0 ± 0.0 for all landmarks inside and outside the retainer areas).
Conclusions
In contrast to steel retainers, titanium and gold retainers are fully compatible for both head/neck and dental MRI when using MSVAT-SPACE.
Clinical relevance
This study demonstrates that titanium and gold retainers do not impair the diagnostic quality of head/neck and dental MRI when applying an appropriate artifact-reduction technique. Steel retainers, however, are not suitable for dental MRI and can severely impair image quality in head/neck MRI of the oral cavity.
Similar content being viewed by others

Introduction
Magnetic resonance imaging (MRI) plays a central role in radiology and its use has continued to increase substantially in recent years, including head and neck imaging [1, 2]. Furthermore, dental MRI is becoming increasingly important in different specialties of dentistry, including orthodontics [3,4,5], periodontology [6,7,8], endodontics [9,10,11,12], and implantology [13,14,15]. This trend is enhanced by recent technical advances [16,17,18,19].
However, the diagnostic benefits of head/neck and dental MRI can be severely compromised by metal-induced susceptibility artifacts originating from orthodontic appliances [20,21,22,23,24,25,26]. In this context, MRI artifacts caused by orthodontic retainers are of particular importance, as the number of patients permanently wearing fixed retainers continues to increase [27,28,29]. Therefore, detailed knowledge of artifacts caused by different retainer materials is crucial for patient care and provides an essential basis for both orthodontists and radiologists in clinical routine. So far, however, there is insufficient data available on MRI artifacts caused by retainers, as previous in vivo studies were mainly based on conventional two-dimensional (2D) sequences and only a maximum of two different retainers were included [21, 22, 25, 26, 30, 31].
As diagnostic limitations caused by retainer-associated MRI artifacts are becoming increasingly relevant in clinical routine, it is of great importance to implement modern MRI techniques that have proven to efficiently reduce metal-artifacts and to compare the extent of artifacts for different retainer materials. The present study for the first time used an MSVAT-SPACE (multiple slab acquisition with view angle tilting gradient based on a sampling perfection with application optimized contrasts using different flip angle evolution) sequence for the evaluation of retainer-associated artifacts. This sequence has proven to efficiently reduce metal-artifacts caused by different dental-materials [19, 32] and allows for high-resolution three-dimensional (3D) imaging of the craniomaxillofacial area [4]. MSVAT-SPACE was applied to quantify artifacts caused by five different retainer materials in vitro and in vivo. The selection of retainers was made based on widely used alloy compositions: two highly paramagnetic steel retainers and three retainers with low paramagnetic properties (titanium grade 1, titanium grade 5, and a gold-platin alloy) were included.
The aim of this combined in vitro and in vivo study was to evaluate the diagnostic MRI compatibility of different fixed orthodontic retainers using a high-resolution 3D-sequence optimized for artifact reduction.
Materials and methods
Study participant and ethics
For in vivo MRI, a 32-year-old male participant without contraindications to MRI was enrolled the study. The study was approved by the institutional ethics committee of the University of Heidelberg (approval number: S-452/2010), and written informed consent was obtained.
Retainers
Five common retainer types were included. For each retainer type, maxillary and mandibular alginate impressions were taken from the volunteer to create plaster models from super-hard dental stone (Hinrizit, Ernst Heinrichs GmbH, Goslar, Germany). All maxillary and mandibular canine-to-canine retainers were bent on these plaster models and then used for both in vitro and in vivo examinations. The weight of each retainer was measured to four decimal places using an analytical balance (R180D, Sartorius Research; Goettingen, Germany). The retainer volume (RV) was determined by dividing the mass by the density. The relevant information on alloy components, RV, and retainer dimensions is given in Table 1.
MRI examinations
In vitro and in vivo MRI scans were performed on a 3 Tesla MRI system (MAGNETOM Trio, Siemens Healthineers, Erlangen, Germany). A 3D T1-weighted MSVAT-SPACE prototype sequence was used for both in vivo and in vitro MRI examinations. This sequence was specifically optimized and evaluated for 3D MRI of the craniofacial area [19, 33]. Sequence parameters were echo time: 5.8 ms, repetition time: 800 ms, bandwidth: 625 Hz/pixel, number of averages: 1, echo train length: 100, field of view: 171 mm × 171 mm, acquisition matrix: 320 × 320, voxel size: 0.53 mm × 0.53 mm × 0.53 mm, number of sections: 256, and time of acquisition: 7:01 min.
For in vitro scans, a 16-channel multi-purpose coil (Variety, Noras MRI products GmbH, Hoechberg, Germany) was used, with retainers embedded in agar gel (Select Agar, ThermoFisher Scientific, Waltham, MA, USA) as described elsewhere [34].
For in vivo scans, maxillary and mandibular acrylic splints (Duran, Scheu Dental, Iserlohn, Germany) were fabricated for the volunteer. All in vivo examinations were performed in centric occlusion with lips and tongue in a resting position using a dedicated 15-channel dental coil (Mandibula, Noras MRI products GmbH, Hoechberg, Germany). MR images were taken (1) with empty splints to verify that the splints did not cause any artifacts and (2) with retainers attached to the splints, according to previous studies [20, 25, 35]. For each retainer material, both maxillary and mandibular retainers were inserted.
In vitro quantification of artifact volumes
Artifact volumes (AV) for all investigated maxillary and mandibular retainers (AVmax; AVmand) were quantified by a standardized semi-automated segmentation procedure [36] using Amira software (Version 6.4.0, ThermoFisher Scientific, Waltham, MA, USA). This workflow allowed for separate 3D identification of signal loss and pile-up artifacts. AV was obtained by adding signal loss and pile-up artifact volumes and subtracting the RV.
In vivo assessment of artifacts
All in vivo datasets were assessed by two independent observers (AJ and TH, both radiologists with seven years’ experience in head/neck and dental MRI). The extent of in vivo artifacts was quantified by assessing the visibility of pre-defined anatomic landmarks using an established five-point rating scale [37, 38]. The visibility of all landmarks was graded as follows: 1 = excellent, 2 = good, 3 = acceptable, 4 = poor, and 5 = not visible. For each retainer material, 124 landmarks were assessed, including dental and non-dental (head and neck related) landmarks inside and outside the retainer areas (Table 2).
Statistical analysis
For in vitro data, the ratio of artifact volume to retainer volume was calculated for both upper and lower jaw retainers (AV/RVmax; AV/RVmand). For in vivo analyses, weighted kappa (κ) with quadratic weights and the 95% confidence interval (CI) were calculated using SPSS Version 27 (SPSS Inc., Chicago, IL, USA) to determine the inter-rater reliability of landmark visibility scoring. For each retainer type, mean values and standard deviations (SD) of visibility scores were calculated for landmarks in areas with retainer and landmarks in areas without retainer. Furthermore, landmarks in areas with retainer were subdivided into upper jaw landmarks, lower jaw landmarks, incisal edges, pulp chambers, apical foramina, and non-dental landmarks.
Results
In vitro quantification of artifact volumes
The largest artifacts were observed for the rectangular steel retainer, with values of 18,060 mm3 for AVmax (proportion of pile-up artifacts: 3.1%) and 15,879 mm3 for AVmand (pile-up artifacts: 2.3%). The AV/RVmax ratio was 2270, compared to an AV/RVmand ratio of 3189.
For the twistflex steel retainer, AVmax was 7437 mm3 (pile-up artifacts: 5.0%) and AVmand was 6317 mm3 (pile-up artifacts: 2.5%). The corresponding AV/RVmax and AV/RVmand ratios were 1061 and 1222, respectively. Thus, artifacts caused by the twistflex steel retainer were considerable, yet substantially smaller than those observed for the conventional rectangular steel retainer.
Retainers made of titanium grade 1, titanium grade 5, and gold generally caused small artifacts. Titanium grade 1 revealed an AVmax of 70 mm3 (pile-up artifacts: 38.7%) and an AVmand of 46 mm3 (pile-up artifacts: 41.1%), with AV/RVmax and AV/RVmand ratios of 11 and 10, respectively. For the titanium grade 5 retainer, values of 47 mm3 for AVmax (pile-up artifacts: 42.7%) and 35 mm3 for AVmand (pile-up artifacts: 36.7%) were observed. Corresponding ratios between artifact and retainer volumes were 8 for AV/RVmax and 8 for AV/RVmand. The gold retainer caused an AVmax of 23 mm3 (pile-up artifacts: 34.1%), an AVmand of 21 mm3 (pile-up artifacts: 28.9%), an AV/RVmax ratio of 4, and an AV/RVmand ratio of 5.
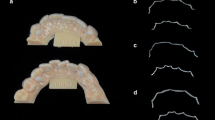
Figures 1 and 2 illustrate the extent of pile-up and signal-loss artifacts caused by all included maxillary and mandibular retainers.

3D volume rendering of artifact volumes of retainers. Rendered artifact volumes (blue: signal-loss artifacts; red: pile-up artifacts) and corresponding photographs are shown for maxillary retainers (upper two rows) and mandibular retainers (lower two rows). (a) Rectangular stainless steel. (b) Twistflex stainless steel. (c) Titanium grade 1. (d) Titanium grade 5. (e) Gold

Volume of pile-up and signal-loss artifacts of maxillary (a) and mandibular (b) retainers
In vivo assessment of dental and head/neck related landmarks
An excellent inter-rater reliability was observed for landmark visibility scoring of all included retainer materials, with κ-values (95% CI) of 0.954 (0.935–0.973) for rectangular steel, 0.940 (0.916–0.964) for twistflex steel, 1.000 (1.000–1.000) for titanium grade 1, 1.000 (1.000–1.000) for titanium grade 5, and 1.000 (1.000–1.000) for gold.
With the rectangular steel retainer inserted, large artifacts were observed in vivo (Fig. 3a) resulting in a strong impact on landmark visibility. The vast majority of predefined anatomical structures within the retainer areas were not visible, leading to a mean visibility score ± SD of 4.8 ± 0.8 (Fig. 4a). For landmarks outside the retainer areas, visibility score was 2.9 ± 1.6 (Fig. 4a). In areas with retainer, subgroup analyses revealed visibility scores of 4.8 ± 0.7 for upper jaw, 4.7 ± 0.9 for lower jaw (Fig. 4b), 5.0 ± 0.0 for incisal edges, 5.0 ± 0.0 for dental pulps, 4.2 ± 1.3 for apical foramina (Fig. 5a), and 4.8 ± 0.8 for non-dental landmarks (Fig. 5b).

Exemplary in vivo MRI images with different retainers inserted. Images show multi-planar reconstructions in sagittal (upper row) and transverse (lower row) orientation for different retainer materials: (a) Rectangular stainless steel. (b) Twistflex stainless steel. (c) Titanium grade 1. (d) Titanium grade 5. (e) Gold. The artifact margins of the two steel retainers are highlighted by dotted lines (a, b). The very small artifacts caused by titanium grade 1, titanium grade 5, and gold are marked by arrows on enlarged image sections (c–e)

Visibility scores of anatomical landmarks for areas with vs. without retainer (a) and for upper vs. lower jaw in retainer areas (b). Black dots represent mean values, and thin bars show standard deviations (if applicable)

Visibility scores of dental (a) and non-dental (b) landmarks within retainer areas. Black dots represent mean values, and thin bars show standard deviations (if applicable)
The twistflex steel retainer caused smaller in vivo artifacts in comparison to the conventional steel retainer (Fig. 3b). Within the retainer areas, average visibility score was 3.1 ± 1.7 (Fig. 4a). In areas without retainer, only minor diagnostic impairment was observed, leading to a visibility score of 1.3 ± 0.7 (Fig. 4a). Subgroups within the retainer areas showed visibility scores of 2.9 ± 1.6 for upper jaw, 3.4 ± 1.8 for lower jaw (Fig. 4b), 5.0 ± 0.0 for incisal edges, 4.1 ± 0.5 for dental pulps, 1.0 ± 0.0 for apical foramina (Fig. 5a), and 2.8 ± 1.6 for non-dental landmarks (Fig. 5b).
By contrast, retainers made of titanium grade 1, titanium grade 5, and gold did not cause any diagnostic impairment in vivo (Fig. 3c–e). Consequently, an excellent visibility of all included landmarks was achieved for these three retainer materials, with visibility scores of 1.0 ± 0.0 for all included dental and non-dental landmarks within and outside the retainer areas (Figs. 4a and b and 5a and b).
Discussion
To our knowledge, this study is the first to systematically evaluate MRI artifacts caused by several different orthodontic retainers both in vitro and in vivo using a high-resolution 3D MRI protocol optimized for artifact reduction. Results demonstrate that artifacts associated with titanium and gold retainers are negligible and do not have any influence on image quality in vivo, even directly adjacent to the retainer wires. Accordingly, retainers made of titanium and gold are fully compatible not only for head/neck MRI but also for dental MRI. By contrast, retainers made of stainless steel produce considerable (twistflex-steel) to severe (rectangular-steel) artifacts, even when using an established artifact reduction technique. Consequently, stainless steel retainers are not compatible for dental MRI and can also affect head/neck related landmarks outside the retainer area. These findings are of high clinical relevance, as most fixed orthodontic retainers are still made of stainless steel in today’s orthodontic practice, whereas titanium and gold retainers only account for a relatively small proportion [29, 39,40,41]. Furthermore, it is important to consider that retainer-associated MRI artifacts will play an even greater role in the future, since the numbers of MRI scans of the craniofacial area and of patients with fixed orthodontic retainers are increasing at the same time [1, 2, 27,28,29].
The present study has several methodological strengths. First, all in vitro and in vivo MRI scans were performed using state-of-the-art 3 T MRI techniques for head/neck imaging, including dedicated coil systems which have demonstrated high performance in previous studies [12, 18, 19, 33, 42, 43]. Consequently, a high signal-to-noise ratio was achieved allowing for scanning with isotropic voxels and high spatial resolution. The selection of retainer materials is an additional asset of this study: For in vitro and in vivo assessment of retainer-associated MRI artifacts, we chose clinically established retainers made of high-susceptibility materials (two stainless steel retainers) vs. low susceptibility materials (titanium grade 1, titanium grade 5, and gold) to include the “extreme ends” of artifact burdens that may be encountered in clinical routine. Furthermore, the use of a high-resolution 3D sequence offered important benefits for both in vitro and in vivo image analysis: from a clinical point of view, it must be noted that isotropic (3D) sequences are becoming increasingly important in head/neck MRI [44, 45] and also play a key role in dental MRI [6,7,8, 46,47,48,49]. In this context, the MSVAT-SPACE sequence used in this study has demonstrated high diagnostic value in several previous in vivo studies [4, 13, 43, 50]. Another important asset of this isotropic high-resolution sequence is that it enables precise quantification of retainer artifacts. Based on this methodological advantage, it was possible to quantify retainer artifact volumes in vitro by using a recently established, semi-automatic, threshold-based segmentation protocol [36] and to perform detailed 3D analyses of image quality in vivo by including small anatomical structures in direct proximity to the maxillary and mandibular retainers. To our knowledge, the present MRI study is the first to investigate the impact of retainer artifacts on the visibility of landmarks that play a pivotal role in dental MRI.
The capability of the applied MSVAT-SPACE sequence to reduce metal-induced artifacts is reflected by our results, particularly in comparison with our previous in vitro MRI study. In this previous study, MRI artifacts associated with the same twistflex steel retainers were quantified using a conventional SPACE sequence under otherwise identical conditions [34]. In direct comparison of these two studies, MSVAT-SPACE offers a reduction of artifact volumes of 53% for the maxillary twistflex steel retainer (SPACE vs. MSVAT-SPACE: 15,642 vs. 7437 mm3 for AVmax and 2235 vs. 1061 for AV/RVmax) and 53% for the mandibular twistflex steel retainer (SPACE vs. MSVAT-SPACE: AVmand 13,530 vs. 6317 mm3 for AVmand and 2602 vs. 1222 for AV/RVmand). These findings are also consistent with an in vitro study using dental implants in which MSVAT-SPACE revealed a 56% reduction of artifact volumes compared to SPACE [19]. Furthermore, our results are in line with a recent vitro and in vivo study by Sonesson et al. comparing a conventional 2D TSE sequence and a 2D TSE sequence with an included artifact reduction technique (view angle tilting and slice encoding for metal artifact correction) with regard to artifacts produced by a stainless steel retainer [31]. Results revealed considerably smaller artifacts for the TSE sequence optimized for artifact reduction in direct comparison with the conventional TSE sequence. Thus, our findings correspond well with earlier studies and emphasize that MRI sequences enabling an efficient reduction of metal-induced artifacts are of crucial importance in head/neck MRI as well as dental MRI.
Several previous studies have investigated MRI artifacts caused by different orthodontic materials. All these studies used conventional MRI-protocols without specific artifact reduction, except for the above-mentioned study by Sonesson et al. assessing the impact of view angle tilting and slice encoding for metal artifact correction in 2D TSE sequences [31]. Importantly, all previous studies included only one retainer type [22, 25, 26, 30, 31] or at most two different materials [21, 51, 52]. By contrast, the present study systematically compared five different retainer materials in vitro and in vivo using a 3D-SPACE sequence with MSVAT for artifact reduction:
-
For both included steel retainers, we found considerable artifact volumes in vitro leading to relevant diagnostic limitations in vivo. In this regard, it should be considered that substantial differences in artifacts between the two stainless steel retainers were observed which may be explained by the manufacturing process resulting in different martensitic properties between retainers of identical stainless steel alloys [51]. Despite these comparatively large differences between the rectangular-steel and the twistflex-steel retainer, our findings are in line with previous analyses on MRI-artifacts caused by steel retainers: Blankenstein et al. found large artifacts caused by a steel retainer on gradient echo and spin echo sequences in vitro [51]. In vitro und in vivo analyses by Tymofiyeva et al. revealed very strong artifacts on gradient echo and spin echo sequences leading to a considerable impairment of image quality in vivo [21]. Shalish et al. assessed a twistflex steel retainer on a dry skull using spin echo sequences and found severe MRI distortions in the regions of the tongue, mandibula, and maxilla [52]. In vivo analyses of Beau et al. based on a spin echo sequence showed massive MRI artifacts produced by a steel retainer that even exceeded the oral cavity [22]. Similarly, Zhylich et al. found non-diagnostic artifact scores in the oral and the pharyngeal regions caused by a steel retainer on spin echo and gradient echo sequences [25]. Finally, Ozawa et al. demonstrated strong MRI artifacts in the anterior oral cavity caused by a steel retainer on fast “cine mode” sequences in vivo [26]
-
The two titanium retainers caused only minimal artifacts in the present study, and importantly, these artifacts did not have any influence on image quality in vivo, even when assessing anatomical structures directly adjacent to the retainers (e.g., incisal edges and pulp chambers of teeth in the retainer area). These results are consistent with Blankenstein et al.’s in vitro study revealing no visible MRI artifacts for a titanium retainer scanned on gradient echo and spin echo sequences [51]. Similarly, an in vitro study by Roser et al. using a 3D SPACE sequence found only minimal artifacts caused by CAD/CAM retainers made of nickel-titanium and titanium grade 5 [34]. Moreover, our findings correspond well with in vitro and in vivo data from Tymofiyeva et al. demonstrating very small MRI artifacts caused by a nickel-titanium retainer on gradient echo and spin echo sequences resulting in only slight distortions [21]
-
Similar to the two titanium retainers, we found only very small artifact volumes for the gold retainer which also did not affect the diagnostic image quality in vivo. This is in accordance with a skull phantom-based study by Shalish et al. revealing no distortions on MR images acquired with spin echo sequences [52]. Furthermore, an in vivo study by Aizenbud et al. using standard sequences for brain imaging found no visible artifacts in association with a gold retainer [30]
Some limitations have to be considered for this study. Despite the aforementioned methodological strengths, it must be noted that MRI artifacts caused by orthodontic retainers depend on many influencing factors. In this regard, especially the retainer material and the applied MRI technique should be mentioned: although our analyses included more retainer materials than all previous in vitro and in vivo studies, there are further materials that should be investigated in future research. Furthermore, MRI artifacts are influenced by a wide range of factors that are specifically related to the setup of the MRI scanner used, including field strength, sequence properties, and coil systems. Accordingly, taking into account these influencing factors, the results of the present study can only be interpreted within the context of the specific methodological approach. However, it is very likely that our key findings (no diagnostic impairment for titanium and gold retainers vs. diagnostically relevant artifacts for stainless steel retainers) will be confirmed when using different MRI protocols including similar techniques for artifact suppression.
Conclusions
This study using a high-resolution 3D MSVAT-SPACE sequence optimized for artifact reduction provides important new information on the diagnostic compatibility of different retainer materials for head/neck MRI and dental MRI:
-
I.
Retainers made of gold or titanium produce only minimal artifacts which do not affect the diagnostic quality in both dental and head/neck MRI under clinical conditions
-
II.
Ferromagnetic steel retainers, however, cause relevant MRI artifacts of varying extent, even when applying a robust artifact suppression technique. These retainers severely impair image quality in proximity to orthodontic retainers (rectangular steel and twistflex-steel) and can also affect more distant anatomical structures (rectangular steel)
These findings are of major clinical relevance for orthodontists as well as radiologists and may contribute to an increased use of gold or titanium retainers in the future.
Data Availability
The datasets generated and analyzed in the current study are available from the corresponding author upon reasonable request.
References
Smith-Bindman R, Miglioretti DL, Johnson E, Lee C, Feigelson HS, Flynn M, Greenlee RT, Kruger RL, Hornbrook MC, Roblin D, Solberg LI, Vanneman N, Weinmann S, Williams AE (2012) Use of diagnostic imaging studies and associated radiation exposure for patients enrolled in large integrated health care systems, 1996–2010. JAMA 307:2400–2409. https://doi.org/10.1001/jama.2012.5960
Smith-Bindman R, Kwan ML, Marlow EC, Theis MK, Bolch W, Cheng SY, Bowles EJA, Duncan JR, Greenlee RT, Kushi LH, Pole JD, Rahm AK, Stout NK, Weinmann S, Miglioretti DL (2019) Trends in use of medical imaging in US health care systems and in Ontario, Canada, 2000–2016. JAMA 322:843–856. https://doi.org/10.1001/jama.2019.11456
Heil A, Lazo Gonzalez E, Hilgenfeld T, Kickingereder P, Bendszus M, Heiland S, Ozga AK, Sommer A, Lux CJ, Zingler S (2017) Lateral cephalometric analysis for treatment planning in orthodontics based on MRI compared with radiographs: a feasibility study in children and adolescents. PLoS One 12:e0174524. https://doi.org/10.1371/journal.pone.0174524
Juerchott A, Freudlsperger C, Weber D, Jende JME, Saleem MA, Zingler S, Lux CJ, Bendszus M, Heiland S and Hilgenfeld T (2020) In vivo comparison of MRI- and CBCT-based 3D cephalometric analysis: beginning of a non-ionizing diagnostic era in craniomaxillofacial imaging? Eur Radiol 30:1488–1497. https://doi.org/10.1007/s00330-019-06540-x
Maspero C, Abate A, Bellincioni F, Cavagnetto D, Lanteri V, Costa A, Farronato M (2019) Comparison of a tridimensional cephalometric analysis performed on 3 T-MRI compared with CBCT: a pilot study in adults. Prog Orthod 20:40. https://doi.org/10.1186/s40510-019-0293-x
Juerchott A, Sohani M, Schwindling FS, Jende JME, Kurz FT, Rammelsberg P, Heiland S, Bendszus M, Hilgenfeld T (2020) In vivo accuracy of dental magnetic resonance imaging in assessing maxillary molar furcation involvement: a feasibility study in humans. J Clin Periodontol 47:809–815. https://doi.org/10.1111/jcpe.13299
Juerchott A, Sohani M, Schwindling FS, Jende JME, Kurz FT, Rammelsberg P, Heiland S, Bendszus M, Hilgenfeld T (2020) Comparison of non-contrast-enhanced dental magnetic resonance imaging and cone-beam computed tomography in assessing the horizontal and vertical components of furcation defects in maxillary molars: an in vivo feasibility study. J Clin Periodontol 47:1485–1495. https://doi.org/10.1111/jcpe.13374
Probst M, Burian E, Robl T, Weidlich D, Karampinos D, Brunner T, Zimmer C, Probst FA, Folwaczny M (2021) Magnetic resonance imaging as a diagnostic tool for periodontal disease: a prospective study with correlation to standard clinical findings-is there added value? J Clin Periodontol 48:929–948. https://doi.org/10.1111/jcpe.13458
Iohara K, Fujita M, Ariji Y, Yoshikawa M, Watanabe H, Takashima A, Nakashima M (2016) Assessment of pulp regeneration induced by stem cell therapy by magnetic resonance imaging. J Endod 42:397–401. https://doi.org/10.1016/j.joen.2015.11.021
Juerchott A, Pfefferle T, Flechtenmacher C, Mente J, Bendszus M, Heiland S, Hilgenfeld T (2018) Differentiation of periapical granulomas and cysts by using dental MRI: a pilot study. Int J Oral Sci 10:17. https://doi.org/10.1038/s41368-018-0017-y
Lizio G, Salizzoni E, Coe M, Gatto MR, Asioli S, Balbi T, Pelliccioni GA (2018) Differential diagnosis between a granuloma and radicular cyst: effectiveness of magnetic resonance imaging. Int Endod J 51:1077–1087. https://doi.org/10.1111/iej.12933
Juerchott A, Jelinek C, Kronsteiner D, Jende JME, Kurz FT, Bendszus M, Heiland S, Hilgenfeld T (2022) Quantitative assessment of contrast-enhancement patterns of the healthy dental pulp by magnetic resonance imaging: a prospective in vivo study. Int Endod J 55:252–262. https://doi.org/10.1111/iej.13662
Hilgenfeld T, Juerchott A, Jende JME, Rammelsberg P, Heiland S, Bendszus M, Schwindling FS (2020) Use of dental MRI for radiation-free guided dental implant planning: a prospective, in vivo study of accuracy and reliability. Eur Radiol 30:6392–6401. https://doi.org/10.1007/s00330-020-07262-1
Probst FA, Schweiger J, Stumbaum MJ, Karampinos D, Burian E, Probst M (2020) Magnetic resonance imaging based computer-guided dental implant surgery-a clinical pilot study. Clin Implant Dent Relat Res 22:612–621. https://doi.org/10.1111/cid.12939
Schwindling FS, Juerchott A, Boehm S, Rues S, Kronsteiner D, Heiland S, Bendszus M, Rammelsberg P, Hilgenfeld T (2021) Three-dimensional accuracy of partially guided implant surgery based on dental magnetic resonance imaging. Clin Oral Implants Res 32:1218–1227. https://doi.org/10.1111/clr.13819
Prager M, Heiland S, Gareis D, Hilgenfeld T, Bendszus M, Gaudino C (2015) Dental MRI using a dedicated RF-coil at 3 Tesla. J Craniomaxillofac Surg 43:2175–2182. https://doi.org/10.1016/j.jcms.2015.10.011
Ludwig U, Eisenbeiss AK, Scheifele C, Nelson K, Bock M, Hennig J, von Elverfeldt D, Herdt O, Flugge T, Hovener JB (2016) Dental MRI using wireless intraoral coils. Sci Rep 6:23301. https://doi.org/10.1038/srep23301
Sedlacik J, Kutzner D, Khokale A, Schulze D, Fiehler J, Celik T, Gareis D, Smeets R, Friedrich RE, Heiland M, Assaf AT (2016) Optimized 14 + 1 receive coil array and position system for 3D high-resolution MRI of dental and maxillomandibular structures. Dentomaxillofac Radiol 45:20150177. https://doi.org/10.1259/dmfr.20150177
Hilgenfeld T, Prager M, Heil A, Schwindling FS, Nittka M, Grodzki D, Rammelsberg P, Bendszus M, Heiland S (2017) PETRA, MSVAT-SPACE and SEMAC sequences for metal artifact reduction in dental MR imaging. Eur Radiol 27:5104–5112. https://doi.org/10.1007/s00330-017-4901-1
Elison JM, Leggitt VL, Thomson M, Oyoyo U, Wycliffe ND (2008) Influence of common orthodontic appliances on the diagnostic quality of cranial magnetic resonance images. Am J Orthod Dentofacial Orthop 134:563–572. https://doi.org/10.1016/j.ajodo.2006.10.038
Tymofiyeva O, Vaegler S, Rottner K, Boldt J, Hopfgartner AJ, Proff PC, Richter EJ, Jakob PM (2013) Influence of dental materials on dental MRI. Dentomaxillofac Radiol 42:20120271. https://doi.org/10.1259/dmfr.20120271
Beau A, Bossard D, Gebeile-Chauty S (2015) Magnetic resonance imaging artifacts and fixed orthodontic attachments. Eur J Orthod 37:105–110. https://doi.org/10.1093/ejo/cju020
Wylezinska M, Pinkstone M, Hay N, Scott AD, Birch MJ, Miquel ME (2015) Impact of orthodontic appliances on the quality of craniofacial anatomical magnetic resonance imaging and real-time speech imaging. Eur J Orthod 37:610–617. https://doi.org/10.1093/ejo/cju103
Blankenstein FH, Asbach P, Beuer F, Glienke J, Mayer S, Zachriat C (2017) Magnetic permeability as a predictor of the artifact size caused by orthodontic appliances at 1.5 T magnetic resonance imaging. Clin Oral Investig 21:281–289. https://doi.org/10.1007/s00784-016-1788-1
Zhylich D, Krishnan P, Muthusami P, Rayner T, Shroff M, Doria A, Tompson B, Lou W, Suri S (2017) Effects of orthodontic appliances on the diagnostic quality of magnetic resonance images of the head. Am J Orthod Dentofacial Orthop 151:484–499. https://doi.org/10.1016/j.ajodo.2016.07.020
Ozawa E, Honda EI, Parakonthun KN, Ohmori H, Shimazaki K, Kurabayashi T, Ono T (2018) Influence of orthodontic appliance-derived artifacts on 3-T MRI movies. Prog Orthod 19:7. https://doi.org/10.1186/s40510-018-0204-6
Valiathan M, Hughes E (2010) Results of a survey-based study to identify common retention practices in the United States. Am J Orthod Dentofacial Orthop 137:170–7; discussion 177. https://doi.org/10.1016/j.ajodo.2008.03.023
Vandevska-Radunovic V, Espeland L, Stenvik A (2013) Retention: type, duration and need for common guidelines. A survey of Norwegian orthodontists. Orthodontics (Chic) 14:e110–7. https://doi.org/10.11607/ortho.964
Padmos JAD, Fudalej PS, Renkema AM (2018) Epidemiologic study of orthodontic retention procedures. Am J Orthod Dentofacial Orthop 153:496–504. https://doi.org/10.1016/j.ajodo.2017.08.013
Aizenbud D, Hazan-Molina H, Einy S, Goldsher D (2012) Craniofacial magnetic resonance imaging with a gold solder-filled chain-like wire fixed orthodontic retainer. J Craniofac Surg 23:e654–e657. https://doi.org/10.1097/SCS.0b013e3182710609
Sonesson M, Al-Qabandi F, Mansson S, Abdulraheem S, Bondemark L, Hellen-Halme K (2021) Orthodontic appliances and MR image artifacts: an exploratory in vitro and in vivo study using 1.5-T and 3-T scanners. Imaging Sci Dent 51:63–71. https://doi.org/10.5624/isd.20200199
Hilgenfeld T, Prager M, Schwindling FS, Nittka M, Rammelsberg P, Bendszus M, Heiland S, Juerchott A (2018) MSVAT-SPACE-STIR and SEMAC-STIR for reduction of metallic artifacts in 3 T head and neck MRI. AJNR Am J Neuroradiol 39:1322–1329. https://doi.org/10.3174/ajnr.A5678
Juerchott A, Saleem MA, Hilgenfeld T, Freudlsperger C, Zingler S, Lux CJ, Bendszus M, Heiland S (2018) 3D cephalometric analysis using magnetic resonance imaging: validation of accuracy and reproducibility. Sci Rep 8:13029. https://doi.org/10.1038/s41598-018-31384-8
Roser C, Hilgenfeld T, Sen S, Badrow T, Zingler S, Heiland S, Bendszus M, Lux CJ, Juerchott A (2021) Evaluation of magnetic resonance imaging artifacts caused by fixed orthodontic CAD/CAM retainers-an in vitro study. Clin Oral Investig 25:1423–1431. https://doi.org/10.1007/s00784-020-03450-x
Zachriat C, Asbach P, Blankenstein KI, Peroz I, Blankenstein FH (2015) MRI with intraoral orthodontic appliance-a comparative in vitro and in vivo study of image artifacts at 1.5 T. Dentomaxillofac Radiol 44:20140416. https://doi.org/10.1259/dmfr.20140416
Hilgenfeld T, Prager M, Schwindling FS, Jende JME, Rammelsberg P, Bendszus M, Heiland S, Juerchott A (2018) Protocol for the evaluation of MRI artifacts caused by metal implants to assess the suitability of implants and the vulnerability of pulse sequences. J Vis Exp 17:57394. https://doi.org/10.3791/57394
Liang X, Jacobs R, Hassan B, Li L, Pauwels R, Corpas L, Souza PC, Martens W, Shahbazian M, Alonso A, Lambrichts I (2010) A comparative evaluation of cone beam computed tomography (CBCT) and multi-slice CT (MSCT) part I. On subjective image quality. Eur J Radiol 75:265–269. https://doi.org/10.1016/j.ejrad.2009.03.042
Gaudino C, Cosgarea R, Heiland S, Csernus R, Beomonte Zobel B, Pham M, Kim TS, Bendszus M, Rohde S (2011) MR-imaging of teeth and periodontal apparatus: an experimental study comparing high-resolution MRI with MDCT and CBCT. Eur Radiol 21:2575–2583. https://doi.org/10.1007/s00330-011-2209-0
Andriekute A, Vasiliauskas A, Sidlauskas A (2017) A survey of protocols and trends in orthodontic retention. Prog Orthod 18:31. https://doi.org/10.1186/s40510-017-0185-x
Carneiro NCR, Nobrega MTC, Meade MJ, Flores-Mir C (2022) Retention decisions and protocols among orthodontists practicing in Canada: a cross-sectional survey. Am J Orthod Dentofacial Orthop 162:51–57. https://doi.org/10.1016/j.ajodo.2021.02.022
Jedlinski M, Mazur M, Schmeidl K, Grocholewicz K, Ardan R, Janiszewska-Olszowska J (2022) Orthodontic retention-protocols and materials-a questionnaire pilot study among Polish practitioners. Materials (Basel) 15:666. https://doi.org/10.3390/ma15020666
Hilgenfeld T, Prager M, Schwindling FS, Heil A, Kuchenbecker S, Rammelsberg P, Bendszus M, Heiland S (2016) Artifacts of implant-supported single crowns - impact of material composition on artifact volume on dental MRI. Eur J Oral Implantol 9:301–308
Hilgenfeld T, Kastel T, Heil A, Rammelsberg P, Heiland S, Bendszus M, Schwindling FS (2018) High-resolution dental magnetic resonance imaging for planning palatal graft surgery-a clinical pilot study. J Clin Periodontol 45:462–470. https://doi.org/10.1111/jcpe.12870
Widmann G, Henninger B, Kremser C, Jaschke W (2017) MRI sequences in head & neck radiology - state of the art. Rofo 189:413–422. https://doi.org/10.1055/s-0043-103280
Touska P, Connor SEJ (2019) Recent advances in MRI of the head and neck, skull base and cranial nerves: new and evolving sequences, analyses and clinical applications. Br J Radiol 92:20190513. https://doi.org/10.1259/bjr.20190513
Tymofiyeva O, Boldt J, Rottner K, Schmid F, Richter EJ, Jakob PM (2009) High-resolution 3D magnetic resonance imaging and quantification of carious lesions and dental pulp in vivo. MAGMA 22:365–374. https://doi.org/10.1007/s10334-009-0188-9
Tymofiyeva O, Rottner K, Jakob PM, Richter EJ, Proff P (2010) Three-dimensional localization of impacted teeth using magnetic resonance imaging. Clin Oral Investig 14:169–176. https://doi.org/10.1007/s00784-009-0277-1
Assaf AT, Zrnc TA, Remus CC, Schonfeld M, Habermann CR, Riecke B, Friedrich RE, Fiehler J, Heiland M, Sedlacik J (2014) Evaluation of four different optimized magnetic-resonance-imaging sequences for visualization of dental and maxillo-mandibular structures at 3 T. J Craniomaxillofac Surg 42:1356–1363. https://doi.org/10.1016/j.jcms.2014.03.026
Manoliu A, Ho M, Nanz D, Dappa E, Boss A, Grodzki DM, Liu W, Chhabra A, Andreisek G, Kuhn FP (2016) MR neurographic orthopantomogram: ultrashort echo-time imaging of mandibular bone and teeth complemented with high-resolution morphological and functional MR neurography. J Magn Reson Imaging 44:393–400. https://doi.org/10.1002/jmri.25178
Hilgenfeld T, Juerchott A, Deisenhofer UK, Weber D, Rues S, Rammelsberg P, Heiland S, Bendszus M, Schwindling FS (2019) In vivo accuracy of tooth surface reconstruction based on CBCT and dental MRI-a clinical pilot study. Clin Oral Implants Res 30:920–927. https://doi.org/10.1111/clr.13498
Blankenstein F, Truong BT, Thomas A, Thieme N, Zachriat C (2015) Predictability of magnetic susceptibility artifacts from metallic orthodontic appliances in magnetic resonance imaging. J Orofac Orthop 76:14–29. https://doi.org/10.1007/s00056-014-0258-0
Shalish M, Dykstein N, Friedlander-Barenboim S, Ben-David E, Gomori JM, Chaushu S (2015) Influence of common fixed retainers on the diagnostic quality of cranial magnetic resonance images. Am J Orthod Dentofacial Orthop 147:604–609. https://doi.org/10.1016/j.ajodo.2014.11.022
Acknowledgements
The authors would like to thank the Dietmar Hopp Foundation for their generous support of this research. Moreover, we thank Tobias Charlet for the assistance in image segmentation.
Funding
Open Access funding enabled and organized by Projekt DEAL. This study was supported by the Dietmar Hopp Foundation (grant number: 1DH2011152; grant holders: AJ and TH).
Author information
Authors and Affiliations
Contributions
AJ: conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, visualization, and writing—original draft. CJR: conceptualization, investigation, methodology, project administration, and writing—review and editing. MAS: methodology, software, and writing—review and editing. MN: methodology, resources, and writing—review and editing. CJL: resources, supervision, and writing—review and editing. SH: methodology, resources, and writing—review and editing. MB: resources, supervision, and writing—review and editing. TH: conceptualization, formal analysis, funding acquisition, methodology, project administration, visualization, and writing—review and editing. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval
All methods were performed in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by the local research ethics committee of the University of Heidelberg (approval number: S-452/2010).
Informed consent
Written informed consent was obtained from the participant included in the study.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Juerchott, A., Roser, C.J., Saleem, M.A. et al. Diagnostic compatibility of various fixed orthodontic retainers for head/neck MRI and dental MRI. Clin Oral Invest 27, 2375–2384 (2023). https://doi.org/10.1007/s00784-023-04861-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-023-04861-2