
Abstract
Backgrounds
Carotid endarterectomy is considered a safe and effective method for preventing stroke in the short and long term in patients with severe carotid stenosis. The internal carotid artery (ICA) occlusion tolerance test was performed to evaluate cerebral tolerance during temporary carotid occlusion, defined as the capacity of the cerebral hemisphere to maintain adequate cerebral blood flow during occlusion of the ICA. Thus, the aim of the present study is to determine the importance of this test in patients undergoing carotid endarterectomy.
Methods
From August 2008 to May 2015, 115 consecutive patients (39 female, 77 male) were referred for carotid endarterectomy at the Santa Casa de Belo Horizonte by the main author.
Results
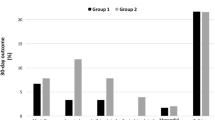
Of the 115 patients who participated in the study, 107 were submitted to carotid endarterectomy. Morbi-mortality was 2.7 %. The presence of deficits during the ICA occlusion tolerance test in less than 30 s was associated with the presence of complications. Among the 104 patients who showed no deficits during the test, only one case (0.9 %) presented complications, while among the three cases that showed deficits during the test and who were submitted to carotid endarterectomy, two cases presented complications (p < 0.0001).
Conclusions
The carotid endarterectomy under locoregional anesthesia is a safe surgical procedure. The internal carotid artery occlusion tolerance test can help identify high-risk patients who have been assigned this treatment.
Similar content being viewed by others


References
Aburahma AF, Mousa AY, Stone PA (2011) Shunting during carotid endarterectomy. J Vasc Surg 54(5):1502–1510
Bagan P, Vidal R, Martinod E, Destable MD, Tremblay B, Dumas JL, Azorin JF (2006) Cerebral ischemia during carotid artery cross-clamping: predictive value of phase-contrast magnetic resonance imaging. Ann Vasc Surg 20:747–752
Brott TG, Hobson RW 2nd, Howard G, Roubin GS, Clark WM, Brooks W, Mackey A, Hill MD, Leimgruber PP, Sheffet AJ, Howard VJ, Moore WS, Voeks JH, Hopkins LN, Cutlip DE, Cohen DJ, Popma JJ, Ferguson RD, Cohen SN, Blackshear JL, Silver FL, Mohr JP, Lal BK, Meschia JF, Investigators CREST (2010) Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med 363:11–23
Brott TG, Halperin JL, Abbara S, Bacharach JM, Barr JD, Bush RL, Cates CU, Creager MA, Moore WS, Panagos PD, Riles TS, Rosenwasser RH (2011) ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS guideline on the management of patients with extracranial carotid and vertebral artery disease: executive summary. Catheter Cardiovasc Interv 81:E75–E123
De Sousa AA, Dellaretti M, Faglioni W Jr, Carvalho GTC (2005) Monitoring of activated coagulation time in carotid endarterectomy. Surg Neurol 64:S1:6–S1:9
Guay JMD, Kopp SMD (2013) Cerebral monitors versus regional anesthesia to detect cerebral ischemia in patients undergoing carotid endarterectomy: a meta-analysis. Can J Anesth 60:266–279
Guy Bianchi P, Tolva V, Dalainas I, Bertoni G, Cireni L, Trimarchi S, Rampoldi V, Casana R (2012) Immediate conversion to CAS after neurological intolerance at cross-clamping test during CEA: a preliminary experience. Int Angiol 31(1):22–27
Herold S, Brown MM, Frackowiak RSJ, Mansfield AO, Thomas DJ, Marshall J (1988) Assessment of cerebral haemodynamic reserve: correlation between PET parameters and CO2 reactivity measured by the intravenous xenon injection technique. J Neurol Neurosurg Psychiatry 51:1045–1050
Howard VJ, Lutsep HL, Mackey A, Demaerschalk BM, Sam AD 2nd, Gonzales NR, Sheffet AJ, Voeks JH, Meschia JF, Brott TG, CREST investigators (2011) Influence of sex on outcomes of stenting versus endarterectomy: a subgroup analysis of the carotid revascularization endarterectomy versus stenting trial (CREST). Lancet Neurol 10:530–537
Howell SJ (2007) Carotid endarterectomy. Br J Anaesth 99(1):119–131
Jacob T, Hingorani A, Ascher E (2007) Carotid Artery Stump Pressure (CASP) in 1135 consecutive endarterectomies under general anesthesia: an old method that survived the test of times. J Cardiovasc Surg (Torino) 48:677–681
Luchetti M, Canella M, Zoppi M, Massei R (2008) Comparison of regional anesthesia versus combined regional and general anesthesia for elective carotid endarterectomy: a small exploratory study. Reg Anesth Pain Med 33:340–345
Lutz HJ, Michael R, Gahl B, Savolainen H (2008) Local versus general anaesthesia for carotid endarterectomy—improving the gold standard? Eur J Vasc Endovasc Surg 36(145–9):150–151
Mantese A, Timaran CH, Chiu D, Begg RJ, Brott TG (2010) The carotid revascularization endarterectomy versus stenting trial (CREST): stenting versus carotid endarterectomy for carotid disease. Stroke 41:S31–S34
Montisci R, Sanfilippo R, Bura R, Branca C, Piga M, Saba L (2013) Status of the circle of Willis and intolerance to carotid cross-clamping during carotid endarterectomy. Eur J Vasc Endovasc Surg 45:107–112
Monzani R (2009) General or locoregional anesthesia for elective carotid endarterectomy: which local anesthetic can we use? Minerva Anestesiol 75:1–2
Pandit JJ, Satya-Krishna R, Gration P (2007) Superficial or deep cervical plexus block for carotid endarterectomy: a systematic review of complications. Br J Anaesth 99(2):159–169
Rango P, Brown MM, Didier L, Howard VJ, Moore WS, Paciaroni M, Ringleb P, Rockman C, Caso V (2013) Management of carotid stenosis in women: Consensus document. Neurology 80:11
Rerkasem K, Rick Bond R, Rothwell PM (2005) Local versus general anaesthetic for carotid endarterectomy. Stroke 36:169–170
Sbarigia E, DarioVizza C, Antonini M, Speziale F, Maritti M, Fiorani B, Francesco Fedele F, Fiorani P (1999) Locoregional versus general anesthesia in carotid surgery: Is there an impact on perioperative myocardial ischemia? Results of a prospective monocentric randomized trial. J Vasc Surg 30:131–138
Stonenham MD, Knighton JD (1999) Regional anaesthesia for carotid endarterectomy. Review article. Br J Anaesthesia 82(6):910–919
Tawfic QA, Ismaili MA, Ahmed MA (2012) Prevention of intra-operative cerebral ischemia during carotid endarterectomy, loco-regional versus general anesthesia. Oman Med J 27(3):254–255
Ugurlucan M, Filik ME, Caglar IM, Zencirci E, Sayin OA, Aydiner O et al (2015) Carotid endarterectomy using a “home-constructed” shunt for patients intolerant to cross-clamping. Surg Today 45(3):284–289
Voeks JH, Howard G, Roubin GS, Malas MB, Cohen DJ, Sternbergh WC, Aronow HD, Eskandari MK, Sheffet AJ, Lal BK, Meschia JF, Brott TG, for the CREST Investigators (2011) Age and outcomes after carotid stenting and endarterectomy: the carotid revascularization endarterectomy versus stenting trial. Stroke 42:3484–3490
Youngberg JA (1987) Pro: regional anesthesia is preferable to general anesthesia for carotid artery surgery. J Cardiothoracic Anesth 1(5):479–482
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No funding was received for this research.
Conflict of interest
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required.
Additional information
Comments
This is an interesting paper from an experienced group inclusive of our good friend, Prof. Atos Alves de Sousa, whose loss is mourned by all of us who knew him.
This being said, the management strategy in these cases is unconventional, and there are several conclusions that we can draw, along with some unanswered questions. Let me explain. The paper presents the safety of loco-regional anesthesia for CEA, (which is well established) and points out, correctly, that most patents do not require placement of an indwelling shunt. The authors identify a high-risk subgroup, 11 patients who failed neurological exam within 30 s of open cross clamping, and state that these patients have failed “cerebrovascular reserve”. This is all very standard.
Now here is the curious part. Eight of these patients were closed back up without CEA and sent for endovascular treatment. It appears that they did well. The other three had a shunt placed at surgery, and two of these three suffered a stroke. This is at variance with the experience of others, myself included, where selective shunt placement is a help, not a hindrance, and where the results in shunted patients are equal to or even superior to those who are not shunted (1). So how can this be explained? We must consider two possibilities: embolic risk or the risk of insufficient flow during the CEA. First, the technique must be considered for possible embolic phenomena. One must assume that a clamped ICA, in these authors’ hands, might have been re-opened to place the shunt if the patient fails the “reserve” test. This is not how I do the operation, and represents a technical point to be considered. When I clamp a carotid, in particular the ICA, I never open it again to the brain until either the operation is done or the shunt has been successfully placed, to prevent clot formation in the vessel and potential embolization up the ICA. If a vessel that has been clamped for a minute or two is reopened and the brain exposed to flow, this adds an embolic risk. In this case, the poor outcome in shunted patients might be attributed to an unseen embolus and have nothing to do with the shunt itself. It is, of course, only speculation, since the exact technique they use is not specified here.
Second, it is curious that the shunts failed to protect these patients from stroke, and one must then ask if the flow was insufficient. The type of shunt used is not specified in the manuscript, but all type shunts I have used are sufficient to maintain adequate perfusion and to bring back a partial, if not complete, return to baseline monitoring values, whether EEG, SSEP, NIRS, TCD, or similar methods are used. This is why we use them! We frankly do not worry about shunt flow because we essentially never have a problem, even in patients with contralateral occlusion, major EEG changes at cross-clamping, or similar risks, all of whom must be considered as failures of cerebrovascular reserve as defined by these authors. So to evaluate shunt insufficiency in this manuscript, we must determine what type of shunt was used, how was the shunt flow evaluated (we use Doppler auscultation and return of baseline monitoring), did the patients’ clinical examinations on the contralateral side improve after the shunts were placed, and did the surgical team use shunts frequently enough to have facility and confidence in the technique?
This paper is fascinating from an experienced group and a dear friend, Prof. de Sousa. I do not personally perform CEA in this way, and when I encounter a failure of cerebrovascular reserve, it is customarily not a problem; we place an indwelling shunt with good results and a low morbidity and mortality, well below 2 % in our series. Shunt placement with an experienced team takes less than a minute, often less than 30 s. I do not recommend opening up patients, clamping and declamping their carotid tree, and then closing them to have an endovascular strategy. Such a technique exposes them to embolic risk, not to mention the risks attendant with a carotid surgical dissection and exposure, with no tangible benefit. The decision to stent a carotid is a decision that I believe should be made preoperatively.
1. Loftus CM: Carotid Artery Surgery: Principles and Technique. 2nd edition. New York, Informa Publishing 2006.
Christopher M. Loftus
Illinois, USA
M. Dellaretti et al. conclude, that immediate conversion of surgery to endovascular techniques can be considered as a treatment strategy, in cases of brain clamp intolerance when carotid shunting cannot be performed in a safe way. A limiting factor of this approach is the risk of underestimating aspects representing inclusion/exclusion criteria of CAS such as plaque morphology and echolucency or challenging vessel anatomy - carotid kinking etc. Another limit is the combination of discomfort and morbidity of the cervical wound as well as the groin femoral catheterization access.
Martin Sames
Czech Republic
Rights and permissions
About this article

Cite this article
Dellaretti, M., de Vasconcelos, L.T., Dourado, J. et al. The importance of internal carotid artery occlusion tolerance test in carotid endarterectomy under locoregional anesthesia. Acta Neurochir 158, 1077–1081 (2016). https://doi.org/10.1007/s00701-016-2789-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-016-2789-1