
Abstract
Purpose
There have been no adequate comparisons of the efficacy, safety, and efficiency of analgesia after laparoscopic colorectal resection (LAC), with and without epidural anesthesia (EDA).
Methods
This was a multicenter prospective observational study of patients undergoing LAC. The primary end point was the mean visual analog scale (VAS) score on postoperative days (PODs) 1–7. The secondary end points were the highest VAS, complication rate, days to first ambulation and fatigue, length of hospital stay, and time to commencement of surgery.
Results
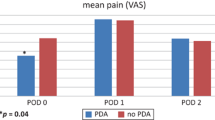
We compared an EDA group (Group E, n = 48) and a no-EDA group (Group O, n = 48) after matching. The mean VAS was not significantly different between the groups (28.7 vs. 30.1, p = 0.288). On assessing the secondary end points, the highest VAS was not significantly different between the groups. In fact, the VAS was lower in Group E only on POD 2. There was no difference in the incidence of complications, the time to first postoperative evacuation was shorter in Group E, and postoperative hospitalization was similar. The time to surgery was shorter in Group O.
Conclusion
These results suggest that LAC without EDA is a feasible option, but with the early and regular use of adjunctive measures to provide more stable analgesia.


Similar content being viewed by others

References
Fearon KC, Ljungqvist O, Von Meyenfeldt M, Revhaug A, Dejong CH, Lassen K, et al. Enhanced recovery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin Nutr. 2005;24:466–77.
Cummings KC, Zimmerman NM, Maheshwari K, Cooper GS, Cummings LC. Epidural compared with non-epidural analgesia and cardiopulmonary complications after colectomy: a retrospective cohort study of 20,880 patients using a national quality database. J Clin Anesth. 2018;47:12–8.
Kitano S, Inomata M, Mizusawa J, Katayama H, Watanabe M, Yamamoto S, et al. Survival outcomes following laparoscopic versus open D3 dissection for stage II or III colon cancer (JCOG0404): a phase 3, randomised controlled trial. Lancet Gastroenterol Hepatol. 2017;2:261–8.
Veldkamp R, Kuhry E, Hop WC, Jeekel J, Kazemier G, Bonjer HJ, et al. Laparoscopic surgery versus open surgery for colon cancer: short-term outcomes of a randomised trial. Lancet Oncol. 2005;6:477–84.
Hübner M, Blanc C, Roulin D, Winiker M, Gander S, Demartines N. Randomized clinical trial on epidural versus patient-controlled analgesia for laparoscopic colorectal surgery within an enhanced recovery pathway. Ann Surg. 2015;261:648–53.
Niraj G, Kelkar A, Hart E, Horst C, Malik D, Yeow C, et al. Comparison of analgesic efficacy of four-quadrant transversus abdominis plane (TAP) block and continuous posterior TAP analgesia with epidural analgesia in patients undergoing laparoscopic colorectal surgery: an open-label, randomised, non-inferiority trial. Anaesthesia. 2014;69:348–55.
Yoshida T, Homma S, Shibasaki S, Shimokuni T, Sakihama H, Takahashi N, et al. Postoperative analgesia using fentanyl plus celecoxib versus epidural anesthesia after laparoscopic colon resection. Surg Today. 2017;47:174–81.
Senagore AJ, Delaney CP, Mekhail N, Dugan A, Fazio VW. Randomized clinical trial comparing epidural anaesthesia and patient-controlled analgesia after laparoscopic segmental colectomy. Br J Surg. 2003;90:1195–9.
Turi S, Gemma M, Braga M, Monzani R, Radrizzani D, Beretta L. Epidural analgesia vs systemic opioids in patients undergoing laparoscopic colorectal surgery. Int J Colorectal Dis. 2019;34:915–21.
Eto K, Kondo I, Kosuge M, Ohkuma M, Haruki K, Neki K, et al. Enhanced recovery after surgery programs for laparoscopic colorectal resection may not need thoracic epidural analgesia. Anticancer Res. 2017;37:1359–64.
Pirrera B, Alagna V, Lucchi A, Berti P, Gabbianelli C, Martorelli G, et al. Transversus abdominis plane (TAP) block versus thoracic epidural analgesia (TEA) in laparoscopic colon surgery in the ERAS program. Surg Endosc. 2018;32:376–82.
Halabi WJ, Kang CY, Nguyen VQ, Carmichael JC, Mills S, Stamos MJ, et al. Epidural analgesia in laparoscopic colorectal surgery: a nationwide analysis of use and outcomes. JAMA Surg. 2014;149:130–6.
Irani JL, Hedrick TL, Miller TE, Lee L, Steinhagen E, Shogan BD, et al. Clinical practice guidelines for enhanced recovery after colon and rectal surgery from the American Society of Colon and Rectal Surgeons and the Society of American Gastrointestinal and Endoscopic Surgeons. Surg Endosc. 2023;37:5–30.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
We have no conflicts of interest to declare in association with the present study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kato, A., Numata, M., Izukawa, S. et al. Prospective observational study comparing the perioperative outcomes of laparoscopic colectomy with or without epidural anesthesia: the Kanagawa Yokohama Colorectal Cancer Study Group (KYCC) 1806. Surg Today (2024). https://doi.org/10.1007/s00595-024-02856-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00595-024-02856-4