
Abstract
Purpose
This study aimed to assess the learning curve of robot-assisted intersphincteric resection for low rectal cancer.
Methods
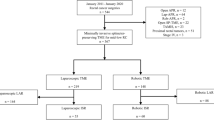
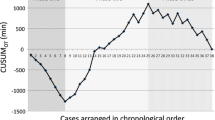
We retrospectively analyzed the clinical data of 89 patients who underwent robot-assisted intersphincteric resection. All surgeries were performed by the same group of surgeons at our institution between June 2016 and April 2021. The learning curve was evaluated using a cumulative sum analysis and the best-fit curve. The different stages of the learning curve were compared based on patient characteristics and short-term clinical outcomes to evaluate their impact on clinical efficacy.
Results
The minimum number of cases required to overcome the learning curve was 47. The learning curve was divided into the learning improvement and proficiency stages. Significant differences were observed in the operation time and the number of lymph nodes between the two stages (P < 0.05), whereas no significant differences were found in intraoperative blood loss, first postoperative exhaust time, postoperative complications, 3-year progression-free survival, overall survival, and local recurrence-free survival (P > 0.05).
Conclusion
Robotic-assisted intersphincteric resection for low rectal cancer exhibits a learning curve that can be divided into two stages: namely, learning improvement and proficiency. Achieving proficiency requires a minimum of 47 surgical cases.




Similar content being viewed by others

Data availability
The data used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Weber PA, Merola S, Wasielewski A, Ballantyne GH. Telerobotic-assisted laparoscopic right and sigmoid colectomies for benign disease. Dis Colon Rectum. 2002;45:1689–96.
Shah MF, Nasir IUI, Parvaiz A. Robotic surgery for colorectal cancer. Visc Med. 2019;35:247–50.
Yamauchi S, Shiomi A, Matsuda C, Takemasa I, Hanai T, Uemura M, et al. Robotic-assisted colectomy for right-sided colon cancer: short-term surgical outcomes of a multi-institutional prospective cohort study in Japan. Ann Gastroenterol Surg. 2023;7:932–9.
Schiessel R, Karner-Hanusch J, Herbst F, Teleky B, Wunderlich M. Intersphincteric resection for low rectal tumours. Br J Surg. 1994;81:1376–8.
Piozzi GN, Park H, Kim J-S, Choi H-B, Lee T-H, Baek S-J, et al. Anatomic landmarks for transabdominal robotic-assisted intersphincteric dissection for ultralow anterior resection. Dis Colon Rectum. 2021;64:e87–8.
Chi P, Huang S-H, Lin H-M, Lu X-R, Huang Y, Jiang W-Z, et al. Laparoscopic transabdominal approach partial intersphincteric resection for low rectal cancer: surgical feasibility and intermediate-term outcome. Ann Surg Oncol. 2015;22:944–51.
Huang S, Huang Y, Chi P, Lin H, Lu X, Xu Z, et al. Completely abdominal approach laparoscopic partial intersphincteric resection after neoadjuvant chemoradiation for initial cT3 Juxta-anal rectal cancer. J Laparoendosc Adv Surg Tech A. 2019;29:809–16.
Huang S, Chen M, Deng Y, Wang X, Lu X, Jiang W, et al. Mesorectal fat area and mesorectal area affect the surgical difficulty of robotic-assisted mesorectal excision and intersphincteric resection, respectively, in different ways. Colorectal Dis. 2020;22:1130–8.
Park SY, Lee SM, Park JS, Kim HJ, Choi G-S. Robot surgery shows similar long-term oncologic outcomes as laparoscopic surgery for mid/lower rectal cancer but is beneficial to ypT3/4 after preoperative chemoradiation. Dis Colon Rectum. 2021;64:812–21.
Jiang W-Z, Xu J-M, Xing J-D, Qiu H-Z, Wang Z-Q, Kang L, et al. Short-term outcomes of laparoscopy-assisted vs open surgery for patients with low rectal cancer: the LASRE randomized clinical trial. JAMA Oncol. 2022;8:1607–15.
Park JS, Lee SM, Choi G-S, Park SY, Kim HJ, Song SH, et al. Comparison of laparoscopic versus robot-assisted surgery for rectal cancers: the COLRAR randomized controlled trial. Ann Surg. 2023;278:31–8.
Jayne D, Pigazzi A, Marshall H, Croft J, Corrigan N, Copeland J, et al. Effect of robotic-assisted vs conventional laparoscopic surgery on risk of conversion to open laparotomy among patients undergoing resection for rectal cancer: the ROLARR randomized clinical trial. JAMA. 2017;318:1569–80.
Feng Q, Yuan W, Li T, Tang B, Jia B, Zhou Y, et al. Robotic versus laparoscopic surgery for middle and low rectal cancer (REAL): short-term outcomes of a multicentre randomised controlled trial. Lancet Gastroenterol Hepatol. 2022;7:991–1004.
Wang X, Zheng Z, Yu Q, Ghareeb WM, Lu X, Huang Y, et al. Impact of surgical approach on surgical resection quality in mid- and low rectal cancer. A Bayesian network meta-analysis. Front Oncol. 2021;11: 699200.
Park JS, Kim NK, Kim SH, Lee KY, Lee KY, Shin JY, et al. Multicentre study of robotic intersphincteric resection for low rectal cancer. Br J Surg. 2015;102:1567–73.
Piozzi GN, Khobragade K, Aliyev V, Asoglu O, Bianchi PP, Butiurca V-O, et al. International standardization and optimization group for intersphincteric resection (ISOG-ISR): modified Delphi consensus on anatomy, definition, indication, surgical technique, specimen description and functional outcome. Colorectal Dis. 2023. https://doi.org/10.1111/codi.16704.
Kayano H, Okuda J, Tanaka K, Kondo K, Tanigawa N. Evaluation of the learning curve in laparoscopic low anterior resection for rectal cancer. Surg Endosc. 2011;25:2972–9.
Zhang L, Hu C, Qin Q, Li R, Zhao J, Zhang Z, et al. Learning process analysis of robotic lateral pelvic lymph node dissection for local advanced rectal cancer: the CUSUM curve of 78 consecutive patients. Surg Today. 2023. https://doi.org/10.1007/s00595-023-02725-6.
Kuo L-J, Lin Y-K, Chang C-C, Tai C-J, Chiou J-F, Chang Y-J. Clinical outcomes of robot-assisted intersphincteric resection for low rectal cancer: comparison with conventional laparoscopy and multifactorial analysis of the learning curve for robotic surgery. Int J Colorectal Dis. 2014;29:555–62.
Aghayeva A, Baca B. Robotic sphincter saving rectal cancer surgery: a learning curve analysis. Int J Med Robot. 2020;16: e2112.
Odermatt M, Ahmed J, Panteleimonitis S, Khan J, Parvaiz A. Prior experience in laparoscopic rectal surgery can minimise the learning curve for robotic rectal resections: a cumulative sum analysis. Surg Endosc. 2017;31:4067–76.
Tang B, Li T, Gao G, Shi J, Li T. Learning curve of robotic-assisted total mesorectal excision for rectal cancer. Front Oncol. 2022;12: 931426.
Sugishita T, Tsukamoto S, Imaizumi J, Takamizawa Y, Inoue M, Moritani K, et al. Evaluation of the learning curve for robot-assisted rectal surgery using the cumulative sum method. Surg Endosc. 2022;36:5947–55.
Kuo L-J, Hung C-S, Wang W, Tam K-W, Lee H-C, Liang H-H, et al. Intersphincteric resection for very low rectal cancer: clinical outcomes of open versus laparoscopic approach and multidimensional analysis of the learning curve for laparoscopic surgery. J Surg Res. 2013;183:524–30.
Yamaguchi T, Kinugasa Y, Shiomi A, Sato S, Yamakawa Y, Kagawa H, et al. Learning curve for robotic-assisted surgery for rectal cancer: use of the cumulative sum method. Surg Endosc. 2015;29:1679–85.
Kim JC, Kim CW, Lee JL, Yoon YS, Park IJ, Kim JR, et al. Complete intersphincteric longitudinal muscle excision May Be key to reducing local recurrence during intersphincteric resection. Eur J Surg Oncol. 2021;47:1629–36.
Kneist W, Stein H, Rheinwald M. Da Vinci single-port robot-assisted transanal mesorectal excision: a promising preclinical experience. Surg Endosc. 2020;34:3232–5.
Acknowledgements
The authors thank the Department of Colorectal Surgery staff at Fujian Medical University Union Hospital (FMUUH, Fuzhou, China).
Funding
Joint Funds for the Innovation of Science and Technology, Fujian Province (2017Y9038, 2023Y9218, 2020Y9071); Fujian Provincial Health Technology Project (2020GGB022, 2020CXA025), Natural Science Foundation of Fujian Province (2022J01753, 2020J011030), Medical Science Research Foundation of Beijing Medical and Health Foundation(B20062DS), and Bethune Charitable Foundation (X-J-2018-004).
Author information
Authors and Affiliations
Contributions
YG, HP, HR, YH, JY, WJ, and PC conceived of the idea and designed the project. YG, JY, and HR collected data. YG and HP analyzed and interpreted the data. YG and SH drafted the manuscript. All authors have read and approved the final manuscript.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest.
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of Fujian Medical University Union Hospital. All procedures performed in this study (involving human participants) were under the ethical standards of the institutional and/or national research committee and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Consent for publication
We confirm that the manuscript has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed. We also confirm that the order of the authors listed in the manuscript has been approved by all the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Gao, Y., Pan, H., Ye, J. et al. Robotic intersphincteric resection for low rectal cancer: a cumulative sum analysis for the learning curve. Surg Today (2024). https://doi.org/10.1007/s00595-024-02841-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00595-024-02841-x