
Abstract
Purpose
We evaluated the impact of omitting mediastinal lymph node dissection (MLND) from the surgical treatment of non-small cell lung cancer (NSCLC) in older patients.
Methods
We collected data retrospectively on 2475 patients who underwent pulmonary resection for NSCLC at our hospital between June, 2006 and December 2018. The subjects of this analysis were 209 patients aged ≥ 75 years who underwent lobectomy for cN0–1 NSCLC. The patients were divided into two groups based on whether they underwent MLND (ND2 group) or not (group ND0–1).
Results
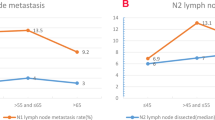
There were more patients aged ≥ 80 years in the ND0–1 group than in the ND2 group (p < 0.001). Patients in the ND0–1 group had clinically earlier stage lung cancers than those in the ND2 group (p = 0.053). We matched patient characteristics in the ND0–1 and ND2 groups by age, tumor diameter, cN, histology, and radiological findings. There were no significant differences in overall survival between the groups (p = 0.295). More patients in the ND2 group suffered complications (41.6% vs. 27.3%, p = 0.061) and arrhythmia episodes than those in the ND0–1 group (14.3% vs. 3.9%, p = 0.021).
Conclusion
MLND in older patients may not extend survival but it could lead to complications. Thus, the omission of MLND may be considered for patients of advanced age.


Similar content being viewed by others


References
Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65:87–108.
Masuda M, Okumura M, Doki Y, Endo S, Hirata Y, Kobayashi J, et al. Thoracic and cardiovascular surgery in Japan during 2014: annual report by the Japanese Association for Thoracic Surgery. Gen Thorac Cardiovasc Surg. 2016;64:665–97.
Darling GE, Allen MS, Decker PA, Ballman K, Malthaner RA, Inculet RI, et al. Randomized trial of mediastinal lymph node sampling versus complete lymphadenectomy during pulmonary resection in the patient with N0 or N1 (less than hilar) non-small cell carcinoma: results of the American College of Surgery Oncology Group Z0030 Trial. J Thorac Cardiovasc Surg. 2011;141:662–70.
Douillard JY, Rosell R, Lena MD, Carpagnano F, Ramlau R, Gonzáles-Larriba JL, et al. Adjuvant vinorelbine plus cisplatin versus observation in patients with completely resected stage IB-IIIA non-small-cell lung cancer (Adjuvant Navelbine International Trialist Association [ANITA]): a randomised controlled trial. Lancet Oncol. 2006;7:719–27.
Früh M, Rolland E, Pignon JP, Seymour L, Ding K, Tribodet H, et al. Pooled analysis of the effect of age on adjuvant cisplatin-based chemotherapy for completely resected non-small-cell lung cancer. J Clin Oncol. 2008;26:3573–81.
Nakao M, Ichinose J, Matsuura Y, Okumura S, Mun M. Outcomes after thoracoscopic surgery in octogenarian patients with clinical N0 non-small-cell lung cancer. Jpn J Clin Oncol. 2020;50:926–32.
Okami J, Higashiyama M, Asamura H, Goya T, Koshiishi Y, Sohara Y, et al. Pulmonary resection in patients aged 80 years or over with clinical stage I non-small cell lung cancer: prognostic factors for overall survival and risk factors for postoperative complications. J Thorac Oncol. 2009;4:1247–53.
Chida M, Minowa M, Karube Y, Eba S, Okada Y, Miyoshi S, et al. Worsened long-term outcomes and postoperative complications in octogenarians with lung cancer following mediastinal lymph-node dissection. Interact Cardiovasc Thorac Surg. 2009;8:89–92.
Wang Y, Wu N, Chen J, Lv C, Yan S, Li S, et al. Is radical mediastinal lymphadenectomy necessary for elderly patients with clinical N-negative non-small-cell lung cancer? A single center matched-pair study. J Surg Res. 2015;193:435–41.
Saji H, Ueno T, Nakamura H, Okumura N, Tsuchida M, Sonobe M, et al. A proposal for a comprehensive risk scoring system for predicting postoperative complications in octogenarian patients with medically operable lung cancer: JACS1303. Eur J Cardiothorac Surg. 2018;53:835–41.
Detterbeck F, Chansky K, Groome P, Bolejack V, Crowley V, Shemanski L, et al. The IASLC lung cancer staging project: methodology and validation used in the development of proposals for revision of the stage classification of NSCLC in the forthcoming (eighth) edition of the TNM classification of lung cancer. J Thorac Oncol. 2016;11:1433–46.
Goldstraw P, Chansky K, Crowley J, Rami-Porta R, Asamura H, Eberhardt WE, et al. The IASLC lung cancer staging project: proposals for revision of the TNM stage groupings in the forthcoming (eighth) edition of the TNM classification for lung cancer. J Thorac Oncol. 2016;11:39–51.
Charlson ME, Sax FL, MacKenzie CR, Fields SD, Braham RL, Douglas RG Jr. Resuscitation: how do we decide? A prospective study of physicians’ preferences and the clinical course of hospitalized patients. JAMA. 1986;255:1316–22.
Colinet B, Jacot W, Bertrand D, Lacombe S, Bozonnat MC, Daures JP, et al. A new simplified comorbidity score as a prognostic factor in non-small-cell lung cancer patients: description and comparison with the Charlson’s index. Br J Cancer. 2005;93:1098–105.
Kawashima M, Murakawa T, Shinozaki T, Ichinose J, Hino H, Konoeda C, et al. Significance of the Glasgow Prognostic Score as a prognostic indicator for lung cancer surgery. Interact Cardiovasc Thorac Surg. 2015;21:637–43.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205–13.
Okasaka T, Usami N, Taniguchi T, Kawaguchi K, Okagawa T, Suzuki H, et al. Can non-performance of radical systematic mediastinal lymphadenectomy be justified in elderly lung cancer patients? An evaluation using propensity-based survival analysis. Eur J Cardiothorac Surg. 2010;38:27–33.
Amar D. Postthoracotomy atrial fibrillation. Curr Opin Anaesthesiol. 2007;20:43–7.
Wu DH, Xu MY, Mao T, Cao H, Wu DJ, Shen YF. Risk factors for intraoperative atrial fibrillation: a retrospective analysis of 10,563 lung operations in a single center. Ann Thorac Surg. 2012;94:193–7.
Muranishi Y, Sonobe M, Menju T, Aoyama A, Chen-Yoshikawa TF, Sato T, et al. Atrial fibrillation after lung cancer surgery: incidence, severity, and risk factors. Surg Today. 2017;47:252–8.
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Tomohiro Maniwa and his coauthors have no conflicts of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Maniwa, T., Kimura, T., Ohue, M. et al. Mediastinal lymph node dissection in older patients with non-small cell lung cancer. Surg Today 52, 458–464 (2022). https://doi.org/10.1007/s00595-021-02373-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-021-02373-8