
Abstract
Aims
To investigate the main feature and the association between euglycemic diabetic ketoacidosis (euDKA) /diabetic ketoacidosis (DKA) and sodium-dependent glucose transporters 2 inhibitors (SGLT-2i) from the FDA adverse event reporting system (FAERS).
Methods
Cases of SGLT-2i-associated with euDKA/DKA were extracted from the FAERS database and compared with the reports for other hypoglycemia agents (ATC10 class). Disproportionality analyses used the reporting odds ratio (ROR) and information components (IC). The lower limit of the IC 95% credibility interval for IC > 0 is considered a reported signal, with at least 3 cases.
Results
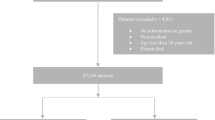
A total of 10,195 cases of euDKA (n = 1680) and DKA (n = 8515) associated with SGLT-2i were identified from the FAERS. The SGLT-2i was associated with higher reporting of euDKA and DKA compared to other hypoglycemia agents (ROR = 16.69 [95% CI 14.89–18.70], IC = 3.27 [95% CI 2.91–3.66] for euDKA; ROR = 16.44 [95% CI 15.72–17.20], IC = 3.19 [95% CI 3.05–3.34] for DKA). In available data, the median onset time of euDKA/DKA was 31 days, and canagliflozin had the longest onset time (96.5 days for euDKA and 75 days for DKA) compared with dapagliflozin and empagliflozin (p < 0.05). Male patients predominate in euDKA (51.9%), and female patients predominate in DKA (53.7%). Most patients discontinue the treatment (95.5% for euDKA, 93.9% for DKA), and approximately 49.0% (n = 3658) of patients had symptomatic remission after discontinuation of SGLT-2i, and 2.3% (n = 173) of patients had no remission. About 75.6% (n = 6126) of patients need hospitalization after euDKA/DKA.
Conclusions
Post-marketing data showed that SGLT-2i was significantly associated with higher reporting of euDKA/DKA. Although euDKA/DKA is rare, clinicians should be aware of SGLT-2i-associated euDKA/DKA events.

Similar content being viewed by others


Data availability
The data analyzed during the current study are available in the following resource available in the public domain: http://openvigil.pharmacology.uni-kiel.de/openvigilfda.php.
References
Brown E, Rajeev SP, Cuthbertson DJ, Wilding JPH (2019) A review of the mechanism of action, metabolic profile and haemodynamic effects of sodium-glucose co-transporter-2 inhibitors. Diabetes Obes Metab 21(Suppl):2. https://doi.org/10.1111/dom.13650
Zelniker TA, Braunwald E (2018) Cardiac and renal effects of sodium-glucose co-transporter 2 inhibitors in diabetes: JACC state-of-the-art review. J AM Coll Cardiol 72:1845–1855. https://doi.org/10.1016/j.jacc.2018.06.040
Furtado RHM, Bonaca MP, Raz I et al (2019) Dapagliflozin and in cardiovascular outcomes patients with type 2 diabetes mellitus and previous myocardial infarction. Circulation 139:2516–2527. https://doi.org/10.1161/CIRCULATIONAHA.119.039996
Mahaffey KW, Neal B, Perkovic V et al (2018) Canagliflozin for primary and secondary prevention of cardiovascular events: results from the CANVAS program (Canagliflozin cardiovascular assessment study). Circulation 137:323–334. https://doi.org/10.1161/CIRCULATIONAHA.117.032038
McGuire DK, Zinman B, Inzucchi SE et al (2020) Effects of empagliflozin on first and recurrent clinical events in patients with type 2 diabetes and atherosclerotic cardiovascular disease: a secondary analysis of the EMPA-REG OUTCOME trial Lancet. Diabetes Endocrinol 8:949–959. https://doi.org/10.1016/S2213-8587(20)30344-2
Benoit SR, Zhang Y, Geiss LS, Gregg EW, Albright A (2018) Trends in diabetic ketoacidosis hospitalizations and in-hospital mortality - United States, 2000–2014 MMWR. Morb Mortal Wkly Rep 67:362–365. https://doi.org/10.1558/mmwr.mm6712a3
Wright J, Ruck K, Rabbitts R et al (2009) Diabetic ketoacidosis (DKA) in Birmingham, UK, 2000–2009: an evaluation of risk factors for recurrence and mortality. Br J Diabetes Vasc Dis 9:278–282. https://doi.org/10.1177/1474651409353248
Garrett CJ, Choudhary P, Amiel SA, Fonagy P, Ismail K (2019) Recurrent diabetic ketoacidosis and a brief history of brittle diabetes research: contemporary and past evidence in diabetic ketoacidosis research including mortality, mental health and prevention. Diabet Med 36:1329–1335. https://doi.org/10.1111/dme.14109
Fukuda M, Nabeta M, Muta T, Fukami K, Takasu O (2020) Euglycemic diabetic ketoacidosis caused by canagliflozin: a case report. Int J Emerg Med 13:2. https://doi.org/10.1186/s12245-020-0261-8
Kelmenson DA, Burr K, Azhar Y, Reynolds P, Baker CA, Rasouli N (2017) Euglycemic diabetic ketoacidosis with prolonged glucosuria associated with the sodium-glucose cotransporter-2 canagliflozin. J Investig Med High Impact Case Rep 5:2324709617712736. https://doi.org/10.1177/2324709617712736
Lin YH (2018) Sodium-glucose cotransporter-2 inhibitors induced eu-glycemic diabetic ketoacidosis: the first report in a type 2 diabetic (T2D) Taiwanese and literature review of possible pathophysiology and contributing factors. J Formos Med Assoc 117:849–854. https://doi.org/10.1016/j.jfma.2018.02.004
Meyer EJ, Gabb G, Jesudason D (2018) SGLT2 inhibitor-associated euglycemic diabetic ketoacidosis: a South Australian clinical case series and Australian spontaneous adverse event notifications. Diabetes Care 41:e47–e49. https://doi.org/10.2337/dc17-1721
Peters AL, Buschur EO, Buse JB, Cohan P, Diner JC, Hirsch IB (2015) Euglycemic diabetic ketoacidosis: a potential complication of treatment with sodium-glucose cotransporter 2 inhibition. Diabetes Care 38:1687–1693. https://doi.org/10.2337/dc15-0843
Pontes JPJ, de Melo CS, Arantes FBB, de Souza RJTG, Módolo NSP, Navarro ELLH (2021) Perioperative euglycemic diabetic ketoacidosis following use of SGLT-2 inhibitors after cardiac surgery. J Clin Anesth 71:110201. https://doi.org/10.1016/j.jclinane.2021.110201
Böhm R, Höcker J, Cascorbi I, Herdegen T (2012) OpenVigil–free eyeballs on AERS pharmacovigilance data. Nat Biotechnol 30:137–138. https://doi.org/10.1038/nbt.2113
Böhm R, von Hehn L, Herdegen T et al (2016) Openvigil FDA inspection of U.S. American adverse drug events pharmacovigilance data and novel clinical applications. PLoS ONE 11:e0157753. https://doi.org/10.1371/journal.pone.0157753
Fadini GP, Bonora BM, Avogaro A (2017) SGLT2 inhibitors and diabetic ketoacidosis: data from the FDA Adverse Event Reporting System. Diabetologia 60:1385–1389. https://doi.org/10.1007/s00125-017-4301-8
Urban TJ, Nicoletti P, Chalasani N et al (2017) Minocycline hepatotoxicity: clinical characterization and identification of HLA-B∗35:02 as a risk factor. J Hepatol 67:137–144. https://doi.org/10.1016/j.jhep.2017.03.010
Brinker A, Cheng C, Chan V (2019) Association of noninfectious pneumonia with ustekinumab use. JAMA Dermatol 155:221–224. https://doi.org/10.1001/jamadermatol.2018.4118
Kitabchi AE, Umpierrez GE, Miles JM, Fisher JN (2009) Hyperglycemic crises in adult patients with diabetes. Diabetes Care 32:1335–1343. https://doi.org/10.2337/dc09-9032
Nasa P, Chaudhary S, Shrivastava PK, Singh A (2021) Euglycemic diabetic ketoacidosis: a missed diagnosis. World J Diabetes 12:514–523. https://doi.org/10.4239/wjd.v12.i5.514
Ehrmann D, Kulzer B, Roos T, Haak T, Al-Khatib M, Hermanns N (2020) Risk factors and prevention strategies for diabetic ketoacidosis in people with established type 1 diabetes. Lancet Diabetes Endocrinol 8:436–446. https://doi.org/10.1016/S2213-8587(20)30042-5
Dhatariya KK, Glaser NS, Codner E, Umpierrez GE (2020) Diabetic ketoacidosis. Nat Rev Dis Primers 6:40. https://doi.org/10.1038/s41572-020-0165-1
Noguchi Y, Tachi T, Teramachi H (2021) Detection algorithms and attentive points of safety signal using spontaneous reporting systems as a clinical data source. Brief Bioinform. https://doi.org/10.1093/bib/bbab347
Blau JE, Tella SH, Taylor SI, Rother KI (2017) Ketoacidosis associated with SGLT2 inhibitor treatment: analysis of FAERS data. Diabetes Metab Res Rev 33:10. https://doi.org/10.1002/dmrr.2924
Barski L, Eshkoli T, Brandstaetter E, Jotkowitz A (2019) Euglycemic diabetic ketoacidosis. Eur J Intern Med 63:9–14. https://doi.org/10.1016/j.ejim.2019.03.014
Ogawa W, Sakaguchi K (2016) Euglycemic diabetic ketoacidosis induced by SGLT2 inhibitors: possible mechanism and contributing factors. J Diabetes Invest 7:135–138. https://doi.org/10.1111/jdi.12401
Rosenstock J, Ferrannini E (2015) Euglycemic diabetic ketoacidosis: a predictable, detectable, and preventable safety concern with SGLT2 inhibitors. Diabetes Care 38:1638–1642. https://doi.org/10.2337/dc15-1380
Menghoum N, Oriot P, Hermans MP (2021) Clinical and biochemical characteristics and analysis of risk factors for euglycaemic diabetic ketoacidosis in type 2 diabetic individuals treated with SGLT2 inhibitors: a review of 72 cases over a 4.5 year period. Diabetes Metab Syndr 15:102275. https://doi.org/10.1016/j.dsx.2021.102275
Bonora BM, Avogaro A, Fadini GP (2018) Sodium-glucose co-transporter-2 inhibitors and diabetic ketoacidosis: an updated review of the literature. Diabetes Obes Metab 20:25–33. https://doi.org/10.1111/dom.13012
Limenta M, Ho CSC, Poh JWW, Goh S-Y, Toh DSL (2019) Adverse drug reaction profile of SGLT2 inhibitor-associated diabetic ketosis/ketoacidosis in Singapore and their precipitating factors. Clin Drug Investig 39:683–690. https://doi.org/10.1007/s40261-019-00794-5
Ata F, Yousaf Z, Khan AA et al (2021) SGLT-2 inhibitors associated euglycemic and hyperglycemic DKA in a multicentric cohort. Sci Rep 11:10293. https://doi.org/10.1038/s41598-021-89752-w
Sehgal V, Ulmer B (2019) Clinical conundrums in the management of diabetic ketoacidosis in the elderly. J Transl Int Med 7:10–14. https://doi.org/10.2478/jtim-2019-0003
Myers SR, Glaser NS, Trainor JL et al (2020) Frequency and risk factors of acute kidney injury during diabetic ketoacidosis in children and association with neurocognitive outcomes. JAMA Net Open 3:e2025481. https://doi.org/10.1001/jamanetworkopen.2020.25481
Acknowledgments
We would like to express our gratitude to professor Xiao Chen for his expert opinions on this subject.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. J.W., M.H. and K.Q. were involved in conceptualization; Z.H., W.Z. and K.L. contributed to methodology; Z.H., W.Z., K.L., S.Y., Y.L., J.M., S.G. and D.L. were involved in formal analysis and investigation; S.Y., Y.L., J.M. and K.L. contributed to writing—original draft preparation; Z.H., W.Z., S.Y. and K.L were involved in writing—review and editing.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Ethical approval
For this type of study, ethical approval is not required.
Informed consent
For this type of study, formal consent is not required.
Additional information
Managed by Giovanni Sartore.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
He, Z., Lam, K., Zhao, W. et al. SGLT-2 inhibitors and euglycemic diabetic ketoacidosis/diabetic ketoacidosis in FAERS: a pharmacovigilance assessment. Acta Diabetol 60, 401–411 (2023). https://doi.org/10.1007/s00592-022-02015-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00592-022-02015-6