
Abstract
Objective
To characterize the discs and vertebrae in detail over time in a group of adolescent individuals with varying training doses using magnetic resonance imaging (MRI).
Method
Thirty-five students were recruited from regular high schools (n=13) as well as schools with athlete competitive skiing programmes (n = 22). The thoraco-lumbar spine of all individuals was examined at baseline and at 2-year follow-up using the same 1.5T scanner and imaging protocol. The individuals were grouped based on their reported training dose: low-to-normal training dose (≤5 h/week, n = 11, mean age 16.5 ± 0.5 years) and high training dose (>5 h/week, n = 24, mean age 17.2 ± 0.6 years.)
Results
At baseline, the signal intensity in the discs and vertebrae were significantly lower in individuals reporting high compared to low-to-normal training dose. The vertebral signal changed significantly over the 2-year period in both groups. However, only individuals reporting low-to-normal training dose displayed an overall disc signal change. Interestingly, the regional analysis displayed at baseline high annular signals in the more training-active individuals followed by a reduction over the two-year period.
Conclusion
This study suggests that disc degeneration is manifested earlier in individuals reporting a higher training dose. Over a 2-year period, however, the degeneration process did not accelerate further. Also, a significant difference in the vertebral signal, at baseline and follow-up as well as over time, could be seen between groups of individuals reporting high versus low-to-normal training dose.
Similar content being viewed by others

Introduction
Disc degeneration and tissue changes in adjacent endplates and vertebrae have been demonstrated to be more common in persons suffering from long-standing low back pain [1]. However, the exact pathophysiology behind and risk factors for such changes have been demonstrated to be multifactorial. Smoking, high-risk occupation, education level, genetic factors, as well as axial load-bearing have been pointed out as risk factors for degenerative disorders causing back pain [2,3,4,5,6,7,8]. While degenerative changes usually manifest in a pronounced manner later in life, overloading of the spine during sports activities at a young age has been shown to accelerate the process [9, 10]. Although studies have reported a higher frequency of radiological changes in athletes than in controls [11, 12], only a few have characterized the spinal tissue changes in detail [9, 13].
New radiological analysis methods, which rely on data-driven analysis of magnetic resonance images (MRI), have recently been proposed for the objective assessment of disc characteristics [9, 13, 14]. These methods have been shown to detect not only gross degenerative disc changes, such as darkening of the disc [15], but also intradiscal changes. For example, an enhanced signal at the region of the outer annulus fibrosus and a concomitant decrease in the signal at the region of the nucleus pulposus have been shown to be associated with the presence of annular tears [13, 16]. Further, the methods have shown promise to reflect early changes of the discs associated with different physical training histories [9, 13] and should also have the feasibility to objectively assess possible alterations over time. However, such detailed studies of training-related spinal changes are lacking. MRI is also frequently used for the characterization of the vertebrae, where apophysis and endplate injuries have been shown to be more common in athletes than in controls [17, 18]. Another vertebral finding that is rather common in the adult population is hyper- or hypo-enhanced signal lesions, where the hyperenhancement is known to represent a fibrovascular or fatty change in the subchondral bone marrow, and the hypo-enhancement represents the replacement of bone with bony sclerosis resulting in little residual marrow [19]. It is not known if such bone marrow changes are commonly present in young individuals, related to training, or if the vertebrae display training-related changes over time.
In this 2-year follow-up of a group of adolescent individuals reporting various training doses, the discs, as well as the vertebrae, were characterized in detail with objective MRI analysis.
Method
Study group
All students that were competing at an elite level in downhill skiing at a sports Academy high school were invited to participate together with all first-year high-school students in two nearby towns. Individuals who reported a history of serious traumatic injury and surgery on the spine and pelvis hip joints, as well as pregnancy and any history of systemic disease, including inflammatory arthritis or pelvic inflammatory disorder, were excluded. Detailed disc analysis of the elite skiers at baseline has previously been reported, revealing differences from non-athlete controls, as well as between skiing disciplines [9]. In the present study, a subgroup of these individuals was characterized in detail after a 2-year follow-up to correlate changes over time with training dose. Only the individuals that agreed to participate in the follow-up study and had a complete set of sagittal MR images both at baseline and follow-up were included in the present study. Out of 102 recruited individuals (elite athletes n = 75, non-athletes n = 27), 43 individuals underwent a follow-up MRI examination after two years. In order to enable objective and detailed characterization of the spinal changes in the MR images without contamination of artefactual noise, an additional exclusion criterion was set up where spinal segments hampered by motion artefacts were excluded from the image analysis. Such artefacts appeared mostly due to pulsations of the blood and cerebrospinal fluid. After exclusion, 35 individuals displayed high image quality in all thoracic spine segments (elite athletes n = 22, non-athletes n = 13), out of which 17 individuals displayed high image quality also in all lumbar spine segments (elite athletes n = 9, non-athletes = 8), resulting in 17 individuals with high image quality for the whole spine. The participants were further sub-grouped according to their reported training doses into high (> 5 h training/week, n = 24 of which 22 were athletes at a competing level) and low-to-normal training dose (0–5 h training/week, n = 11). The baseline demographics for the groups can be seen in Table 1.
The study was conducted in accordance with the Declaration of Helsinki. Ethical approval for this study was obtained by the Institutional Ethics Review Board (ID NR 2020–01657).
MRI examinations
All included individuals were examined at baseline and follow-up at the department of radiology at Ostersund Hospital, Sweden, using the same MRI scanner (1.5 Tesla HDXt Signa Echospeed, General Electronics, Madison, USA). The thoraco-lumbar spine was examined with standardized MRI sequences, including a T1-weighted (T1w) sequence (FOV = 480 mm, slice thickness = 4 mm, TR = 560 ms, TE < 90 ms) and T2-weighted (T2w) sequence in the sagittal view (FOV = 480 mm, slice thickness = 4 mm, TR = 4463 ms, TE = 110 ms). The mean duration between examinations was 24.6 months (range 24–25 months).
Detailed MRI analysis
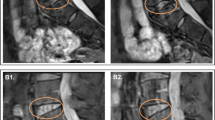
For each individual, seven discs and vertebrae (lumbar L5-L1; thoracal between L1 and T11) were analysed (Fig. 1). These spinal components were outlined manually (ITK-snap) on T1w images in three mid-sagittal slices of the spine. Subsequently, the delineations were transferred to the T2w images for detailed characterization of the disc and vertebral tissue. Each disc was further divided into five equally large subregions in the anterior–posterior direction (1: anterior annulus fibrosus, 2: border zone between annulus fibrosus and anterior part of nucleus pulposus, 3: central part of nucleus pulposus, 4: border zone between posterior part of nucleus pulposus and posterior annulus fibrosus and 5: posterior annulus fibrosus). The mean signal intensity in the different discs and vertebra was normalized to cerebral spinal fluid signal (Fig. 1), hereafter referred to as relative SI (rSI).

Delineation of discs and vertebrae included in the study, shown on a T2-weighted image. Disc and vertebra analysis was performed for the thoracic (between L1 and T11) and lumbar (L5-L1) spine separately, as well as for the whole spine. Cerebrospinal fluid signal was for normalization
Statistical analysis
Violin plots, displaying the probability density of the acquired data, were used to visualize differences between groups. Parametric (t test and chi-square) and nonparametric (Mann–Whitney U test) tests using p < 0.05 were used to evaluate statistical differences in demographics and MRI findings, respectively. The python distribution platform Anaconda (Anaconda Software Distribution. Computer software. Version 1.9.12. Anaconda Inc., February 2020) was used to perform statistical tests and for data visualization.
Results
Disc findings
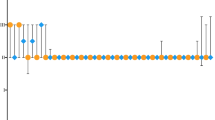
At baseline, there was a significant difference in disc rSI between individuals reporting low-to-normal compared to high training dose for the whole spine as well as for the lumbar and thoracic spine separately ( \* MERGEFORMAT Fig. 2), with the high training dose group having significantly lower signal. Over time, the disc rSI value decreased and individuals with a low-to-normal training dose displayed a significantly larger decrease for the whole spine compared to individuals with a high training dose. At follow-up, significant differences in disc rSI were no longer found between the groups.

Relative disc signal intensity (SI) at baseline vs. at 2-year follow-up for the whole spine and for the lumbar and thoracic level in individuals reporting low-to-normal training dose (p = 0.002, 0.002, 0.18) and high training dose (p = 0.35, 0.33, 0.47). At baseline, there was a statistical difference between the groups for whole, lumbar, and thoracic spine with p < 0.001, < 0.001, and 0.04, respectively. At follow-up, all p values were > 0.05. Violin widths are scaled by count
The subregional analysis revealed that the reduction of the disc signal was heterogeneous ( \* MERGEFORMAT Fig. 3) and showed different behaviours depending on the training dose. For individuals reporting low-to-normal training dose, the lumbar spine displayed a significant decrease in disc rSI over time at the central and posterior part of the nucleus pulposus, while individuals reporting high training dose displayed a significant decrease at the anterior and posterior annulus fibrosis ( \* MERGEFORMAT Fig. 3).

Subregional distribution of the disc signal intensity at baseline vs. at 2-year follow-up in the lumbar spine for a) all individuals (p < 0.05 for subregions 1, 2, and 5), b) individuals with low-to-normal training activity (p < 0.05 in subregions 3 and 4) and c) individuals with high training activity (p < 0.05 in subregions 1 and 5)
Multiple linear regression was performed to test if age or BMI could significantly predict signal intensity at baseline. It was found that BMI significantly predicted signal intensity in discs (R2 = 0.022, p = 0.012); however, it only explains 2% of the signal variation. Age did not significantly predict disc response.
Vertebral findings
The image analysis of the vertebrae revealed a significant difference in the relative SI (signal intensity) over time, which differed between groups with diverse training doses both at baseline and follow-up ( \* MERGEFORMAT Fig. 4). Also, the groups displayed different distribution patterns. At follow-up, the group with high training dose had a more skewed distribution towards lower values.

Vertebral signal intensity (SI) at baseline vs. at 2-year follow-up for the whole spine in all individuals (p < 0.001), individuals with low-to-normal training activity (p = 0.006), and individuals with high training activity (p = 0.002). At both baseline and follow-up, the difference between the groups was statistically significant (p < 0.001)
Multiple linear regression revealed that neither age nor BMI significantly predicted vertebrae response at baseline.
Discussion
This 2-year follow-up study displayed significant MRI changes over time in both discs and vertebrae associated with the training dose.
Individuals reporting a lower training dose displayed a general reduction in the disc signal over time, most probably reflecting normal ageing with a reduction in the hydration of the disc [9, 16, 20]. Such effect could not be statistically established in individuals reporting higher training doses, not even when focusing on the region of the nucleus pulposus alone. At baseline, these individuals displayed a lower disc signal in comparison to the less training-active individuals, probably reflecting an earlier onset of the degenerative cascade influenced by physical activity and age. Over the 2-year period, however, the process did not seem to progress rapidly towards more pronounced degeneration. The subregional analysis at baseline further revealed an enhanced signal in the annulus fibrosus in the more training-active individuals, most probably representing high signalling annular tears that are known to be displayed as high signal zones within the annular fibrosis on T2-weighted MR images [21]. It has been suggested that the presence of annular tears influences the speed of the degenerative process in the disc [22]. Due to the lack of sufficient evidence, however, this is a point of debate. Also, the hypothesis has been contradicted by the study of Farshad-Amacker et al., demonstrating in a large cohort follow-up study that an enhanced annular signal due to the presence of a tear in the annulus fibrosus is not a predictor for accelerated disc degeneration [23] In this study, it was shown that the enhancement in the annular signal, found in the more training-active individuals at baseline, was followed by a clear reduction over time. One could speculate that such behaviour reflects the healing of the annular tears [13, 16], where a thin layer of fibrous tissue gradually replaces the lesion, initially composed of vascularized granulation tissue [24].
The reduction in the annular signal and the lack of further accelerated disc degeneration over the two-year period may reflect the effect of injury prevention training, here attended by the included elite athletes after submission to the Ski Academy, for strengthening of important muscle groups and stabilization of the core. Others have shown the value of injury prevention training programmes [25,26,27]. Such systematic training form may have had an augmentative effect on the disc cells and the matrix production to stimulate tissue repair and maintenance of the discs.
The high-dose training also seemed to influence the vertebral tissue. Compared to low-to-normal training dose, individuals that reported a high training dose displayed lower vertebral signal. The lower signal might be related to a higher bone density [28]. Some authors have reported that the peak bone mineral density in the lumbar vertebrae occurs during the teens [29, 30], while others suggest that it is reached in the twenties or thirties [31,32,33]. Some studies have also reported an association between specific sports activities and bone mineral density during adolescence [34,35,36]. The vertebral findings might reflect a measurable bone mineral increase in both groups, more prominent in the high-dose training group, possibly influenced by physical activity and age. On the other hand, the presence of sclerotic changes in the vertebral tissue following the degenerative cascade may also explain the lower vertebral signal [37].
Overall, the findings from the present study highlight the intricate tissue response in the spine concerning training dose. A high dose may have caused negative effects, manifested as somewhat earlier degenerative disc changes. However, it also demonstrated positive effects, as no further disc degeneration was observed over the study period. Additionally, the study suggests possible positive effects on the vertebral tissue. It is important for adolescents to try to find an optimal training dose to prevent acute injuries, long-term tissue injuries, and pain problems. Not only the overall training dose but the type of training (load, time, frequency, etc.) plays a role in the influence on the intervertebral disc (13). Based on the study results, no exact optimal training dose for the studied sport, downhill skiing, could be determined. Neither could advice against a high training dose, with the included training moments, be advised. The present study hopefully inspires more longitudinal studies on adolescent individuals practicing different sports to develop more precise training advice and guidelines to prevent spinal problems.
Limitations
There were some limitations of the study. Several of the MR images displayed motion artefacts and were consequentially excluded from the analysis, which limited the statistical analysis and its power. In addition, the individuals that reported high training doses were slightly older than the individuals that reported low-to-normal training doses. Finally, even though a longitudinal difference between the groups could be statistically verified, the study lacks additional follow-ups to establish the findings over a longer period.
Conclusion
This study suggests that disc degeneration is manifested earlier in individuals reporting a higher training dose. Over a 2-year period, however, the degeneration process did not accelerate further. Also, a significant difference in the vertebral signal, at baseline and follow-up, as well as over time, could be seen between groups of individuals reporting high versus low-to-normal training dose.
References
Lagerstrand K, Brisby H, Hebelka H (2019) Low back pain patients and controls display functional differences in endplates and vertebrae measured with T2-mapping. Europ Spine J 28:234–240
Markotić V, Zubac D, Miljko M et al (2017) Level of education as a risk factor for extensive prevalence of cervical intervertebral disc degenerative changes and chronic neck pain. Cent Eur J Public Health 25:245–250. https://doi.org/10.21101/cejph.a4897
Hirose Y, Chiba K, Karasugi T et al (2008) A functional polymorphism in THBS2 that affects alternative splicing and MMP binding is associated with lumbar-disc herniation. Am J Hum Genet 82:1122–1129. https://doi.org/10.1016/j.ajhg.2008.03.013
Mio F, Chiba K, Hirose Y et al (2007) A functional polymorphism in COL11A1, which encodes the alpha 1 chain of Type XI collagen, is associated with susceptibility to lumbar disc herniation. Am J Hum Genet 81:1271–1277. https://doi.org/10.1086/522377
Luoma K, Riihimäki H, Raininko R et al (1998) Lumbar disc degeneration in relation to occupation. Scand J Work Environ Health 24:358–366. https://doi.org/10.5271/sjweh.356
Paul CPL, de Graaf M, Bisschop A et al (2017) Static axial overloading primes lumbar caprine intervertebral discs for posterior herniation. PLoS ONE 12:e0174278–e0174278. https://doi.org/10.1371/journal.pone.0174278
Rannou F, Corvol M, Revel M et al (2001) Disk degeneration and disk herniation: the contribution of mechanical stress. Revue du Rhumatisme 68:543–546. https://doi.org/10.1016/S1297-319X(01)00325-6
Green BN, Johnson CD, Snodgrass J et al (2016) Association between smoking and back pain in a cross-section of adult Americans. Curēus (Palo Alto, CA) 8:e806–e806. https://doi.org/10.7759/cureus.806
Lagerstrand K, Baranto A, Hebelka H (2021) Different disc characteristics between young elite skiers with diverse training histories revealed with a novel quantitative magnetic resonance imaging method. Eur Spine J 30:2082–2089. https://doi.org/10.1007/s00586-021-06869-2
Witwit WA, Kovac P, Sward A et al (2018) Disc degeneration on MRI is more prevalent in young elite skiers compared to controls. Knee Surg Sports Traumatol Arthrosc 26:325–332. https://doi.org/10.1007/s00167-017-4545-3
Rosendahl K, Strouse PJ (2016) Sports injury of the Pediatric musculoskeletal system. Radiologia Medica 121:431–441. https://doi.org/10.1007/s11547-015-0615-0
Baranto A, Hellstrom M, Cederlund CG et al (2009) Back pain and MRI changes in the Thoraco-lumbar spine of top athletes in four different sports: a 15-year follow-up study. Knee Surg Sports Traumatol Arthrosc 17:1125–1134. https://doi.org/10.1007/s00167-009-0767-3
Belavy DL, Brisby H, Douglas B et al (2020) Characterization of intervertebral disc changes in asymptomatic individuals with distinct physical activity histories using three different quantitative MRI techniques. J Clin Med 9:1841. https://doi.org/10.3390/jcm9061841
Lagerstrand K, Brisby H, Hebelka H (2021) Associations between high-intensity zones, endplate, and Modic changes and their effect on T2-mapping with and without spinal load. J Orthop Res 39:2703–2710. https://doi.org/10.1002/jor.25024
Waldenberg C, Hebelka H, Brisby H et al (2018) MRI histogram analysis enables objective and continuous classification of intervertebral disc degeneration. Eur Spine J 27:1042–1048. https://doi.org/10.1007/s00586-017-5264-7
Waldenberg C, Hebelka H, Brisby H et al (2019) Differences in IVD characteristics between low back pain patients and controls associated with HIZ as revealed with quantitative MRI. PLoS ONE 14:e0220952–e0220952. https://doi.org/10.1371/journal.pone.0220952
Moorman CT, Johnson DC, Pavlov H et al (2004) Hyperconcavity of the lumbar vertebral endplates in the elite football lineman. Am J Sports Med 32:1434–1439. https://doi.org/10.1177/0363546504264930
Sward L, Jacobsson BO, Karlsson L. Vertebral ring apophysis injury in athletes Is the etiology different in the thoracic and lumbar spine?
Modic M (2007) Modic type 1 and type 2 changes. J Neurosurg Spine 6:150–151. https://doi.org/10.3171/spi.2007.6.2.150
Trattnig S, Stelzeneder D, Goed S et al (2010) Lumbar intervertebral disc abnormalities: comparison of quantitative t2 mapping with conventional MR at 3.0 T. Eur Radiol 20:2715–22. https://doi.org/10.1007/s00330-010-1843-2
Aprill C, Bogduk N (1992) High-intensity zone: a diagnostic sign of painful lumbar disc on magnetic resonance imaging. Br J Radiol 65:361–369. https://doi.org/10.1259/0007-1285-65-773-361
Sharma A, Pilgram T, Wippold FJ (2009) Association between annular tears and disk degeneration: a longitudinal study. Am J Neuroradiol 30:500–506. https://doi.org/10.3174/ajnr.A1411
Farshad-Amacker NA, Hughes AP, Aichmair A et al (2014) Is an annular tear a predictor for accelerated disc degeneration? Eur Spine J 23:1825–1829. https://doi.org/10.1007/s00586-014-3260-8
Peng BG, Hou SX, Wu WW et al (2006) The pathogenesis and clinical significance of a high-intensity zone (HIZ) of lumbar intervertebral disc on mr imaging in the patient with discogenic low back pain. Eur Spine J 15:583–587. https://doi.org/10.1007/s00586-005-0892-8
Maurer E, Klinger C, Lorbeer R et al (2020) Long-term effect of physical inactivity on thoracic and lumbar disc degeneration—an MRI-based analysis of 385 individuals from the general population. Spine Journal 20:1386–1396. https://doi.org/10.1016/j.spinee.2020.04.016
Brisby H, Qun Wei A, Molloy T, et al. The Effect of Running Exercise on Intervertebral Disc Extracellular Matrix Production in a Rat Model.
Deng C, Xia W (2018) Effect of Tai Chi Chuan on degeneration of lumbar vertebrae and lumbar discs in middle-aged and aged people: a cross-sectional study based on magnetic resonance images. J Int Med Res 46:578–585. https://doi.org/10.1177/0300060517734115
Hatipoglu HG, Selvi A, Ciliz D et al (2007) Quantitative and diffusion MR imaging as a new method to assess osteoporosis. Am J Neuroradiol 28:1934–1937. https://doi.org/10.3174/ajnr.A0704
Bachrach LK, Hastie T, Wang M-C, et al. Bone Mineral Acquisition in Healthy Asian, Hispanic, Black, and Caucasian Youth: A Longitudinal Study*. 1999. https://academic.oup.com/jcem/article/84/12/4702/2864787
Sabatier J-P, Guaydier-Souquires G, Laroche D et al (1996) Bone mineral acquisition during adolescence and early adulthood: a study in 574 healthy females 10–24 years of age. Osteopor Int 6:141–8
Mein AL, Briffa NK, Dhaliwal SS et al (2004) Lifestyle influences on 9-year changes in BMD in young women. J Bone Miner Res 19:1092–1098. https://doi.org/10.1359/JBMR.040310
Pedrazzoni M, Girasole G, Bertoldo F et al (2003) Definition of a population-specific DXA reference standard in Italian women: The Densitometric Italian Normative Study (DINS). Osteoporos Int 14:978–982. https://doi.org/10.1007/s00198-003-1521-1
Berger C, Goltzman D, Langsetmo L et al (2010) Peak bone mass from longitudinal data: Implications for the prevalence, pathophysiology, and diagnosis of osteoporosis. J Bone Miner Res 25:1948–1957. https://doi.org/10.1002/jbmr.95
Fehily AM, Coles RJ, Evans WD, et al. Factors affecting bone density in young adults13. 1992. https://academic.oup.com/ajcn/article/56/3/579/4715423
Slemenda CW, Reister TK, Hui SL et al (1994) Influences on skeletal mineralization in children and adolescents: evidence for varying effects of sexual maturation and physical activity. J Pediatr 125:201–207. https://doi.org/10.1016/S0022-3476(94)70193-8
Tylavsky FA, Anderson JJB, Talmage R et al (1992) Are calcium intakes and physical activity patterns during adolescence related to radial bone mass of white college-age females? Osteopor Int 2:232–40
Määttä JH, Karppinen JI, Luk KDK et al (2015) Phenotype profiling of Modic changes of the lumbar spine and its association with other MRI phenotypes: a large-scale population-based study. The Spine J 15:1933–1942. https://doi.org/10.1016/j.spinee.2015.06.056
Funding
Open access funding provided by University of Gothenburg.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None of the authors have any potential conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rosenqvist, L., Hebelka, H., Baranto, A. et al. Detailed MRI evaluation of the spine: a 2-year follow-up study of young individuals reporting different training doses. Eur Spine J 32, 4145–4152 (2023). https://doi.org/10.1007/s00586-023-07961-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-023-07961-5