
Abstract
Purpose
In an osteoporotic vertebral body, cement-augmented pedicle screw fixation could possibly be optimized by the creation of an initial cavity. The aim of this study is to compare three test groups with regard to their loosening characteristics under cyclic loading.
Methods
Eighteen human, osteoporotic spine segments were divided in three groups. Flexibility tests and cyclic loading tests were performed with an internal fixator. The screws were fixed after creation a cavity and with cement (cavity-augmented group), without cavity and with cement (augmented group), and without cavity and without cement (control group). Cyclic loading up to 100,000 cycles was applied with a complex loading protocol. Screw loosening was measured with flexibility tests after implantation and after cyclic loading. Cement distribution was visualized from CT scans.
Results
In all groups, range of motion increased during cyclic loading, representing significant screw loosening after 100,000 cycles. In both augmented groups, screw loosening was less pronounced than in the control group. The cavity-augmented group showed only a slight tendency of screw loosening, but with smaller variations compared to both other groups. This may be explained with a trend for a more equal and homogeneous cement volume around each tip for the cavity-augmented group.
Conclusion
This study demonstrated that creating a cavity may allow a more equal fixation of all pedicle screws with slight reduction of loosening. However, augmentation only through a cannulated screw is almost equivalent, if care is taken that enough cement volume can be pushed out around the tip of the screw.
Similar content being viewed by others

Introduction
Significant progress has been made in the surgical treatment of spinal diseases over the last two decades. Minimally invasive procedures have been optimized as a result of research into innovative pedicle screw systems. Spinal diseases with osteoporotic vertebral bodies pose a particular challenge in this context, where pedicle screw loosening seems to be an issue [1, 2]. Successful use of an internal fixator largely depends on the creation of a solid bony connection between the pedicle screw and the vertebral body [3].
In patients with manifest osteoporosis, however, the anchoring of the pedicle screw in the weakened bone structure poses a problem, since the holding power of screws in bone depends largely on bone quality [4,5,6,7,8,9]. Changes in bone architecture as a result of osteoporosis often lead to post-operative complications when this technique is used, e.g. the loosening of pedicle screws and subsequent kyphosis and even fractures as result of this loosening [10].
Osteoporosis usually affects elderly patients. On account of demographic developments, the number of world population over 60 years is expected to increase from around 12.3% to 21.5% until 2050. In all European countries, the trend is growing [11]. As a result, the number of osteoporosis patients with associated clinical presentation is also expected to rise. According to studies by Melton et al., every third woman and every fifth man over the age of 50 will sustain a fracture due to osteoporosis [12, 13]. The clinical and epidemiologic/economic relevance of medical engineering solutions for this disease will thus significantly increase in future [14].
Pedicle screw systems have been continuously modified in order to compensate for reduced holding power in osteoporotic vertebral bodies. Many different screw designs, positions, diameters, lengths and insertion depths as well as different anchoring methods, torques and augmentation techniques have been tested [15,16,17,18,19,20,21,22,23,24,25,26].
Of these developments, cement augmentation has become an established standard in today's clinical practice. Augmentation of osteoporotic vertebrae in polymethylmethacrylate (PMMA)-assisted vertebroplasty can significantly increase pedicle screw pull-out forces to levels exceeding the strength of cortical bone [29].
In biomedical studies, satisfactory results have been achieved with the use of bone cement for screw augmentation in the treatment of osteoporotic spines [27,28,29,30,31]. Cook et al. showed that pull-out strength of cemented pedicle screws was up to 250% higher than that of non-cemented screws in control groups. Also, clinical evaluations have demonstrated that the frequency of screw pull-out and pedicle defects decreased when cement-augmented screws were used [32, 33].
A possible approach, using cement-augmented screws, is to create a cavity in the vertebral body, which is subsequently filled with a self-curing elastomer when the pedicle screw is implanted. In contrast to the conventional method, in which cement flows into the trabecular structure of the vertebra without creation of a cavity, a better anchoring in the bone and less loosening is expected (with the new method creating an initial cavity) [34].
Sandmann et al. verified that one advantage of balloon-guided cement augmentation of iliosacral screws in the treatment of insufficiency fractures of the sacrum was the much stronger bone–screw interface compared to other procedures and was biomechanically superior against vertical shear stress [35]. This last study explained an interesting method, but using a balloon kyphoplasty system is expensive for preparing the osteoporotic vertebral bone.
Therefore, we thought about a technique being simple and cheap. Performing a defined cavity in the vertebral body with a commercially produced thread cutter should have a positive effect on screw loosening in order to be augmented through the fenestrated screw. In our study concept, we compared monosegmental osteoporotic lumbar spine specimens divided in three groups with cement-augmented pedicle screws using the thread cutter, only cement augmented and without any augmentation. The focus is on the loosening behaviour of the three groups under continuous cyclic dynamic loading [36, 37]. An increase in range of motion (ROM) during cyclic loading—not pull-out strength—was chosen as a parameter for loosening.
The goal of this study was to demonstrate whether the creation of a cavity with subsequent cement augmentation has a positive effect on screw loosening.
Material and methods
Specimens and implants
A total of 18 fresh human motion segments from 16 osteoporotic lumbar spines in an age range between 50 and 87 years with a bone density between 35.5 and 79.8 mg Ca-HA/cm3 were distributed into three equal groups with matched age, bone density. Each group consisted of two lumbar spinal segments L2–L3, L3–L4 and L4–L5 equally distributed. Another selection criterion, with the help of x-rays, was a similar size of the vertebrae and the pedicles in order to allow the use of the same screw size with a diameter of 6.5 mm and a length of 45 mm.
All screws were polyaxially, cannulated and fenestrated with six holes in the distal third of the thread to allow augmentation with bone cement (KyphX®HV-RTM; Medtronic, Minneapolis, USA). The segments were bridged using a standard monosegmental internal fixator (Medtronic, Minneapolis, USA). The rigid screw connection of the fixator was achieved with two pre-bent longitudinal rods (5.5 mm in diameter, 50 mm in length) fixed in position with four locking screws.
Preparation and implantation
During preparation of the specimens, all osteoligamentous structures and the intervertebral disks were preserved [38]. Subsequently, the specimens were embedded in PMMA (Technovit 3040, Heraeus Kulzer, Wehrheim, Germany) for fixation in the testing machines.
Three different surgical techniques for implanting pedicle screws in human osteoporotic lumbar vertebrae were compared:
In a cavity-augmented group (with cavity and with cement in the vertebral body), a special thread cutter with a diameter of 6.5 mm and an extendable blade, which can produce by turning the cutter a cavity with a of diameter 10.5 mm in the distal third of the pre-drilled hole. This cavity could be filled with bone cement to augment the screw in a standardized cement volume (Fig. 1).

Schematic lateral view of the surgical procedure in the cavity-augmented group
In an augmented group (without cavity and with cement in the vertebral body), the screws were augmented with a standard cement augmentation using the experimental procedure based on the same principle as in the cavity-augmented group, but an ordinary thread cutter with a diameter of 6.5 mm was used before inserting the bone cement to guarantee the same study conditions (Fig. 2).

Schematic lateral view of the surgical procedure in the augmented group
For both cement augmentation, syringes were filled with 1.8 ml of bone cement (KyphX®HV-RTM; Medtronic, Minneapolis, USA), to ensure that 1.5 ml of bone cement can be injected as an anchoring medium between screw and bone (the rest remained in the screw core).
In a control group (without cavity and without cement in the vertebral body), also an ordinary thread cutter with a diameter of 6.5 mm was used (Fig. 3).

Schematic lateral view of the surgical procedure in the control group
After the implantation of the screws, the fixator rods were mounted and the correct position and the depth of cavities were checked by CT scanning corresponding to the "up-and-in" method according to Krag et al. [39].
Test procedure
Flexibility tests were performed in a custom-made spine loading simulator in the intact state, directly after implantation, and after different steps of dynamic loading (Fig. 4a) [40]. The specimens were loaded with pure moments of ± 3.75 Nm (recommended for osteoporotic specimens) in right/left lateral bending, flexion/extension and left/right axial rotation without follower load [38]. During loading, the specimens were allowed to move unconstrained in the five uncontrolled degrees of freedom. Two load cycles were applied for preconditioning, and the evaluation was carried out from the third cycle.

a The custom-made spine tester with a plastic model for the flexibility tests and an exemplary load–displacement curve of an evaluated specimen. b The dynamic material testing machine with a plastic model for the cyclic loading tests
For cyclic loading, each of the specimens was mounted in a dynamic material testing machine (Instron 8871, Instron Wolpert GmbH, Darmstadt, Germany) (Fig. 4b) [41, 42]. During cyclic loading, the specimens turned clockwise around its own axis (360°/min) and were loaded sinusoidally between 100 and 600 N with a lever arm of 0.03 m and a frequency of 5 Hz.
With this set-up, the specimen was turning around its axis clockwise and therefore passed through all positions, starting from flexion into more and more lateral bending to the left until it reaches extension (this point of time is presented in Fig. 4). Then, it continues more and more in to lateral bending to the right until if finally reaches flexion again. This further continues until the number of cycles has been reached.
Loosening of the implants was to be examined and evaluated on the basis of changes in ROM. Both range of motion (ROM) and neutral zone (NZ) of each specimen were normalized to the individual ROM value directly after implantation (100%). Normalization was carried out in order to quantify the effect after cyclic loading and to simplify comparability with regard to the primary stability directly after implantation.
ROM and NZ in the three tested groups were investigated and compared directly after implantation and after 20,000, 40,000, 60,000 and 100,000 loading cycles [41, 42]. In reality, 100,000 load cycles correspond to a load over a period of 3 months in the elderly [42].
Throughout the entire experiment, the specimens were kept moist with saline-soaked gauze [43].
Cement distribution
Cement distribution and the environment of the cement–screw complex in the vertebral body were checked by CT-scanning before and after cyclic loading. The CT sequences were analysed using reconstruction software (Amira® 5.2.2.).
The volume of the cement, which surrounds the screw, was quantified using the CT images. Since it was difficult to distinguish between the gray values of the isolated cement and screw, first the combined volume of the cement and fixation device was segmented. Then, the volume of the isolated fixation device (without cement) was subtracted to finally gain only the cement surrounding the screw. The volume of the isolated fixation device (12,066 ± 161 mm3) was obtained from the control group.
Statistical analysis
For statistical analysis, we compared only primary stability with the state after 100,000 cycles.
The Wilcoxon signed-rank test was used within each group. The Kruskal–Wallis test was used between the groups. The cement distribution of the two augmented groups was analysed with the Mann–Whitney U-Test. The level of significance was p ≤ 0.05, since we could not assume a normal distribution of measurement results with a sample size of n = 6 specimens per group. While this study was explorative, the p values were not corrected for multiple comparisons and therefore they only indicate trends.
The intermediate steps after 20,000 and 40,000 and 60,000 load cycles were evaluated only in order to detect a potential failure of the tested pedicle screws.
Results
Range of motion and loosening behaviour
Implantation of the fixator stabilized the bridged segments in each of the three motion planes in all groups compared to the intact state and cyclic loading increased continuously, in most cases significantly, the ROM, representing a strong trend of screw loosening (Figs. 5, 6, 7). In general, the increase during flexion/extension and lateral bending was greater than during axial rotation.

Comparison of normalized ROM values in % (median and ranges) at ± 3.75 Nm of the three groups (n = 6) after each test cycle in flexion/extension. *p ≤ 0.05

Comparison of normalized ROM values in % (median and ranges) at ± 3.75 Nm of the three groups (n = 6) after each test cycle in lateral bending. *p ≤ 0.05

Comparison of normalized ROM values in % (median and ranges) at ± 3.75 Nm of the three groups (n = 6) after each test cycle in axial rotation. *p ≤ 0.05
In flexion/extension, the ROM increased by 89% for the cavity-augmented group and 95% for the conventionally augmented group, which was much less for both than compared to the non-augmented control group with a nearly twofold increase by 173% (Fig. 5).
In lateral bending, the ROM increased even more by 101% for the cavity-augmented group and 102% for the conventionally augmented group, which was also much less than in the non-augmented control by 169% (Fig. 6).
In axial rotation the ROM the loosing effect seems to be fairly low for all groups, almost none for the augmented groups and slight but still significant for the non-augmented control by 54% (Fig. 7).
Interpreting these results, there seems to be a slight trend for less screw loosening for the cavity-augmented compared to the augmented group and a clear trend for superior conditions for the augmented groups compared to the non-augmented control group. However, these differences were statistically not significant probably due to the low number of tested specimens.
Cement distribution
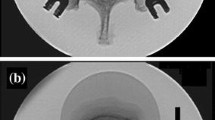
The evaluation of the CT scans with the implanted specimens showed in the cavity-augmented group an average cement volume of 4245 ± 1207 mm3 surrounding the four screws in each treated segment and in the augmented group an average cement volume of 3690 ± 1104 mm3 (Table1). The differences were statistically not significant.
The implanted specimens of the cavity-augmented group demonstrated a more equal cement distribution around the tip of all screws in the same vertebrae (Fig. 8). This is not necessarily the case for all specimens in the augmented group, where sometimes screw tips have less or almost no cement (e.g. specimen 1164 and 1496).

Reconstruction from CT scans of cement distribution around the screw tips of the cavity-augmented and the augmented group
It was further observed that loosening due to cyclic loading affected the entire cement–screw construct in the vertebral body but did not occur between screw and cement.
Discussion
This study showed a slight trend for less screw loosening when a screw is augmented in a prepared cavity, compared to when cement is only injected through a cannulated screw. But there is a clear trend of superior conditions for both augmented groups compared to the non-augmented control group.
The obvious advantage of the cavity seems to be a more equal cement distribution around each screw tip in the individual vertebra. Therefore, a more standardized cement volume can be expected. However, the blade, which creates the cavity, may smoothen the cement–bone interface because the bone material rubbed off is squeezed into the hollow spaces in the cancellous bone of the vertebra and creates a defined cement border. Therefore, it seems that also the augmented screws group may have an advantage, because the indentation of the cement in the cancellous bone may be more pronounced. This explains that the difference of the results is not as clear as maybe expected. As a quintessence, the effect of the cavity showed a slightly better fixation, which was not statistically significant between the groups.
Our findings are in line with clinical trials with similar procedures, e.g. a kyphoplasty for screw augmentation confirmed better results concerning loosening rates [35]. In biomechanical studies, satisfactory results have been achieved with the use of bone cement for screw augmentation in the treatment of osteoporotic spines [27,28,29,30,31]. PMMA-assisted vertebroplasty showed that augmentation of osteoporotic vertebrae can significantly increase pedicle screw pull-out forces to levels exceeding the strength of cortical bone [29]. It could also be shown that pull-out strength of cemented pedicle screws was up to 250% higher than that of non-cemented screws in control groups [8]. Other evaluations were able to demonstrate that the frequency of screw pull-out and pedicle defects decreased when cement-augmented screws were used [32, 33].
The literature also includes several studies on the strength of pedicle screw anchors in human osteoporotic vertebral bodies, but most of these studies are confined to the pull-out strength of screw fixation systems [8, 15, 27,28,29]. In this context, pull-out strength is regarded as an indicator of a temporarily stable screw–bone connection [7, 15,16,17, 20, 29, 44].
However, this kind of test only considers the primary stability and does not necessarily simulate realistic loading conditions which act on the screws.
In the meantime, more and more dynamic test methods have been established, such as toggle tests or more sophisticated set-ups by applying bending moments to single screws, which were implanted in isolated vertebrae [25, 31, 34, 45,46,47].
Bostelmann et al. performed a study with the purpose to assess the fixation effects of different augmentation techniques (including percutaneous cement application) and to investigate pedicle screw loosening under physiological cyclic cranio-caudal loading with single vertebral bodies. By the cranio-caudal cyclic loading, failure of the pedicle screws occurred by screw cut through the superior endplate and the characteristic "windshield-wiper effect", typically observed in clinical practice, could be reproduced [31]. Liebsch et al. established with their novel mechanical testing model a promising method for the standardized testing of pedicle screws regarding screw loosening for cases where the screw rotates around a point close to the screw entry point [47].
In this study, we used a more complex cyclic loading set-up with monosegmental cadaver specimens and complete instrumentation of fixators as already used in a previous study [37]. The specimens were tested at the start of the test in flexion. By rotating around its axis, this was continuously merging in lateral bending, afterwards merging into extension, then into lateral bending, finally coming back to flexion and so on. This mimics more closely the physiological conditions rather than a pull-out test or a toggle test with single screws.
Nevertheless, this method has its limitation. Patients probably move more after a fixation than simulated with the applied number of load cycles.
By using this cyclic testing method, however, we were able to observe a continuous screw loosening in all groups over 100,000 load cycles. These 100,000 cycles were able, because we applied the bending moments with a frequency of 5 Hz. This frequency was chosen to limit the total testing time to about 8 h, including preparation, the necessary radiographs and several flexibility tests [43]. With more load cycles, autolysis processes would have impaired the results. However, this number of load cycles correspond to an in vivo time period of 5–6 weeks for a young person and perhaps 3 months for an elderly person [41, 42]. A frequency of 5 Hz does not represent the situation in daily life, because we walk with roughly 1 Hz and we move during our daily activities, which results in higher bending moments with a much lower frequency in a very arbitrary way. Therefore, we do not allow relaxation of the bony structures as this might occur in vivo. Furthermore, we cannot simulate healing processes with an in vitro experiment. However, we believe this is an acceptable compromise as it rather represents a worst-case scenario.
In summary, this study demonstrated that creating a cavity at the tip of a screw may guarantee a more equal cement distribution of each screw in the same vertebra. However, augmentation only through a cannulated screw is almost equivalent, if care is taken that enough cement volume can be pushed out around the tip of the screw.
References
Galbusera F, Volkheimer D, Reitmaier S, Berger-Roscher N, Kienle A, Wilke HJ (2015) Pedicle screw loosening: a clinically relevant complication? Eur Spine J. https://doi.org/10.1007/s00586-015-3768-6
Reginster JY, Burlet N (2006) Osteoporosis: a still increasing prevalence. Bone 38(2 Suppl 1):S4-9. https://doi.org/10.1016/j.bone.2005.11.024
Esses SI, Sachs BL, Dreyzin V (1993) Complications associated with the technique of pedicle screw fixation A selected survey of ABS members. Spine (Phila Pa 1976) 18(15):2231–2238 (discussion 2238-2239)
Halvorson TL, Kelley LA, Thomas KA, Whitecloud TS 3rd, Cook SD (1994) Effects of bone mineral density on pedicle screw fixation. Spine (Phila Pa 1976) 19(21):2415–2420
Okuyama K, Abe E, Suzuki T, Tamura Y, Chiba M, Sato K (2001) Influence of bone mineral density on pedicle screw fixation: a study of pedicle screw fixation augmenting posterior lumbar interbody fusion in elderly patients. Spine J 1(6):402–407
Ponnusamy KE, Iyer S, Gupta G, Khanna AJ (2011) Instrumentation of the osteoporotic spine: biomechanical and clinical considerations. Spine J 11(1):54–63. https://doi.org/10.1016/j.spinee.2010.09.024
Paxinos O, Tsitsopoulos PP, Zindrick MR, Voronov LI, Lorenz MA, Havey RM, Patwardhan AG (2010) Evaluation of pullout strength and failure mechanism of posterior instrumentation in normal and osteopenic thoracic vertebrae. J Neurosurg Spine 13(4):469–476. https://doi.org/10.3171/2010.4.SPINE09764
Cook SD, Salkeld SL, Stanley T, Faciane A, Miller SD (2004) Biomechanical study of pedicle screw fixation in severely osteoporotic bone. Spine J 4(4):402–408. https://doi.org/10.1016/j.spinee.2003.11.010
Weiser L, Huber G, Sellenschloh K, Viezens L, Puschel K, Morlock MM, Lehmann W (2018) Time to augment?! Impact of cement augmentation on pedicle screw fixation strength depending on bone mineral density. Eur Spine J 27(8):1964–1971. https://doi.org/10.1007/s00586-018-5660-7
DeWald CJ, Stanley T (2006) Instrumentation-related complications of multilevel fusions for adult spinal deformity patients over age 65: surgical considerations and treatment options in patients with poor bone quality. Spine (Phila Pa 1976) 31(19 Suppl):S144-151. https://doi.org/10.1097/01.brs.0000236893.65878.39
United Nations (2015) World population prospects: the 2015 revision. Department of economic and social affairs, population division. https://www.un.org/en/development/desa/publications/world-population-prospects-2015-revision.html
Melton LJ 3rd, Atkinson EJ, O’Connor MK, O’Fallon WM, Riggs BL (1998) Bone density and fracture risk in men. J Bone Miner Res 13(12):1915–1923. https://doi.org/10.1359/jbmr.1998.13.12.1915
Melton LJ 3rd, Chrischilles EA, Cooper C, Lane AW, Riggs BL (2005) How many women have osteoporosis? JBMR Anniversary Classic. JBMR J Bone Miner Res 20(5):886–892. https://doi.org/10.1359/jbmr.2005.20.5.886
Kanis JA, Johnell O (2005) Requirements for DXA for the management of osteoporosis in Europe. Osteoporos Int 16(3):229–238. https://doi.org/10.1007/s00198-004-1811-2
Becker S, Chavanne A, Spitaler R, Kropik K, Aigner N, Ogon M, Redl H (2008) Assessment of different screw augmentation techniques and screw designs in osteoporotic spines. Eur Spine J 17(11):1462–1469. https://doi.org/10.1007/s00586-008-0769-8
Hasegawa T, Inufusa A, Imai Y, Mikawa Y, Lim TH, An HS (2005) Hydroxyapatite-coating of pedicle screws improves resistance against pull-out force in the osteoporotic canine lumbar spine model: a pilot study. Spine J 5(3):239–243. https://doi.org/10.1016/j.spinee.2004.11.010
Pfeiffer FM, Abernathie DL, Smith DE (2006) A comparison of pullout strength for pedicle screws of different designs: a study using tapped and untapped pilot holes. Spine (Phila Pa 1976) 31(23):E867-870. https://doi.org/10.1097/01.brs.0000244658.35865.59
Wittenberg RH, Lee KS, Shea M, White AA 3rd, Hayes WC (1993) Effect of screw diameter, insertion technique, and bone cement augmentation of pedicular screw fixation strength. Clin Orthop Relat Res 296:278–287
Wu ZX, Gong FT, Liu L, Ma ZS, Zhang Y, Zhao X, Yang M, Lei W, Sang HX (2012) A comparative study on screw loosening in osteoporotic lumbar spine fusion between expandable and conventional pedicle screws. Arch Orthop Trauma Surg 132(4):471–476. https://doi.org/10.1007/s00402-011-1439-6
Zdeblick T, Kunz D, Cooke MR M (1993) Pedicle screw pullout strength correlation with insertional torque. Spine 18(12):1673–1676
Weiser L, Dreimann M, Huber G, Sellenschloh K, Puschel K, Morlock MM, Rueger JM, Lehmann W (2016) Cement augmentation versus extended dorsal instrumentation in the treatment of osteoporotic vertebral fractures: a biomechanical comparison. Bone Joint J 98-B(8):1099–1105. https://doi.org/10.1302/0301-620X.98B8.37413
Liu D, Wu ZX, Pan XM, Fu SC, Gao MX, Shi L, Lei W (2011) Biomechanical comparison of different techniques in primary spinal surgery in osteoporotic cadaveric lumbar vertebrae: expansive pedicle screw versus polymethylmethacrylate-augmented pedicle screw. Arch Orthop Trauma Surg 131(9):1227–1232. https://doi.org/10.1007/s00402-011-1290-9
Hoppe S, Keel MJ (2017) Pedicle screw augmentation in osteoporotic spine: indications, limitations and technical aspects. Eur J Trauma Emerg Surg 43(1):3–8. https://doi.org/10.1007/s00068-016-0750-x
Chao KH, Lai YS, Chen WC, Chang CM, McClean CJ, Fan CY, Chang CH, Lin LC, Cheng CK (2013) Biomechanical analysis of different types of pedicle screw augmentation: a cadaveric and synthetic bone sample study of instrumented vertebral specimens. Med Eng Phys 35(10):1506–1512. https://doi.org/10.1016/j.medengphy.2013.04.007
Kueny RA, Kolb JP, Lehmann W, Puschel K, Morlock MM, Huber G (2014) Influence of the screw augmentation technique and a diameter increase on pedicle screw fixation in the osteoporotic spine: pullout versus fatigue testing. Eur Spine J 23(10):2196–2202. https://doi.org/10.1007/s00586-014-3476-7
Lindtner RA, Schmid R, Nydegger T, Konschake M, Schmoelz W (2018) Pedicle screw anchorage of carbon fiber-reinforced PEEK screws under cyclic loading. Eur Spine J 27(8):1775–1784. https://doi.org/10.1007/s00586-018-5538-8
Burval DJ, McLain RF, Milks R, Inceoglu S (2007) Primary pedicle screw augmentation in osteoporotic lumbar vertebrae: biomechanical analysis of pedicle fixation strength. Spine (Phila Pa 1976) 32(10):1077–1083. https://doi.org/10.1097/01.brs.0000261566.38422.40
Evans SL, Hunt CM, Ahuja S (2002) Bone cement or bone substitute augmentation of pedicle screws improves pullout strength in posterior spinal fixation. J Mater Sci Mater Med 13(12):1143–1145
Sarzier JS, Evans AJ, Cahill DW (2002) Increased pedicle screw pullout strength with vertebroplasty augmentation in osteoporotic spines. J Neurosurg 96(3 Suppl):309–312
Choma TJ, Pfeiffer FM, Swope RW, Hirner JP (2012) Pedicle screw design and cement augmentation in osteoporotic vertebrae: effects of fenestrations and cement viscosity on fixation and extraction. Spine (Phila Pa 1976) 37(26):E1628-1632. https://doi.org/10.1097/BRS.0b013e3182740e56
Bostelmann R, Keiler A, Steiger HJ, Scholz A, Cornelius JF, Schmoelz W (2017) Effect of augmentation techniques on the failure of pedicle screws under cranio-caudal cyclic loading. Eur Spine J 26(1):181–188. https://doi.org/10.1007/s00586-015-3904-3
Chang MC, Liu CL, Chen TH (2008) Polymethylmethacrylate augmentation of pedicle screw for osteoporotic spinal surgery: a novel technique. Spine (Phila Pa 1976) 33(10):E317-324. https://doi.org/10.1097/BRS.0b013e31816f6c73
Fransen P (2007) Increasing pedicle screw anchoring in the osteoporotic spine by cement injection through the implant. Technical note and report of three cases. J Neurosurg Spine 7(3):366–369. https://doi.org/10.3171/SPI-07/09/366
Schmoelz W, Keiler A, Konschake M, Lindtner RA, Gasbarrini A (2018) Effect of pedicle screw augmentation with a self-curing elastomeric material under cranio-caudal cyclic loading-a cadaveric biomechanical study. J Orthop Surg Res 13(1):251. https://doi.org/10.1186/s13018-018-0958-z
Sandmann GH, Stockle U, Freude T, Stuby FM (2018) Balloon guided cement augmentation of iliosacral screws in the treatment of insufficiency fractures of the sacrum - description of a new method and preliminary results. Acta Chir Orthop Traumatol Cech 85(2):85–88
Kettler A, Wilke HJ, Dietl R, Krammer M, Lumenta C, Claes L (2000) Stabilizing effect of posterior lumbar interbody fusion cages before and after cyclic loading. J Neurosurg 92(1 Suppl):87–92
Wilke HJ, Kaiser D, Volkheimer D, Hackenbroch C, Puschel K, Rauschmann M (2016) A pedicle screw system and a lamina hook system provide similar primary and long-term stability: a biomechanical in vitro study with quasi-static and dynamic loading conditions. Eur Spine J 25(9):2919–2928. https://doi.org/10.1007/s00586-016-4679-x
Wilke HJ, Wenger K, Claes L (1998) Testing criteria for spinal implants: recommendations for the standardization of in vitro stability testing of spinal implants. Eur Spine J 7(2):148–154
Krag MH (1976) (1991) Biomechanics of thoracolumbar spinal fixation. Rev Spine (Phila Pa 1976) 16(3 Suppl):S84-99
Wilke HJ, Claes L, Schmitt H, Wolf S (1994) A universal spine tester for in vitro experiments with muscle force simulation. Eur Spine J 3(2):91–97
Kettler A, Schmoelz W, Shezifi Y, Ohana N, Ben-Arye A, Claes L, Wilke HJ (2006) Biomechanical performance of the new BeadEx implant in the treatment of osteoporotic vertebral body compression fractures: restoration and maintenance of height and stability. Clin Biomech (Bristol, Avon) 21(7):676–682. https://doi.org/10.1016/j.clinbiomech.2006.02.005
Wilke HJ, Mehnert U, Claes LE, Bierschneider MM, Jaksche H, Boszczyk BM (2006) Biomechanical evaluation of vertebroplasty and kyphoplasty with polymethyl methacrylate or calcium phosphate cement under cyclic loading. Spine (Phila Pa 1976) 31(25):2934–2941. https://doi.org/10.1097/01.brs.0000248423.28511.44
Wilke H-J, Jungkunz B, Wenger K, Claes LE (1998) Spinal segment range of motion as a function of in vitro test conditions: effects of exposure period, accumulated cycles, angular-deformation rate, and moisture condition. Anat Rec 251(1):15–19
Liljenqvist U, Hackenberg L, Link T, Halm H (2001) Pullout strength of pedicle screws versus pedicle and laminar hooks in the thoracic spine. Acta Orthop Belg 67(2):157–163
Brasiliense LB, Lazaro BC, Reyes PM, Newcomb AG, Turner JL, Crandall DG, Crawford NR (2013) Characteristics of immediate and fatigue strength of a dual-threaded pedicle screw in cadaveric spines. Spine J 13(8):947–956. https://doi.org/10.1016/j.spinee.2013.03.010
Choma TJ, Frevert WF, Carson WL, Waters NP (2011) Pfeiffer FM (2011) Biomechanical analysis of pedicle screws in osteoporotic bone with bioactive cement augmentation using simulated in vivo multicomponent loading. Spine (Phila Pa 1976) 36(6):454–462. https://doi.org/10.1097/BRS.0b013e3181d449ec
Liebsch C, Zimmermann J, Graf N, Schilling C, Wilke HJ, Kienle A (2018) In vitro validation of a novel mechanical model for testing the anchorage capacity of pedicle screws using physiological load application. J Mech Behav Biomed Mater 77:578–585. https://doi.org/10.1016/j.jmbbm.2017.10.030
Acknowledgements
This study was supported by Medtronic (Minneapolis, USA). The authors gratefully acknowledge Dr. Benedikt Schlager for the determination of the cement volume, Laura Zengerle for the statistically evaluation and Karin Werner for their assistance in preparing the manuscript.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
The study was approved by the ethical committee board of the University of Ulm (No. 227/12).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Riesner, HJ., Blattert, T.R., Krezdorn, R. et al. Can cavity-based pedicle screw augmentation decrease screw loosening? A biomechanical in vitro study. Eur Spine J 30, 2283–2291 (2021). https://doi.org/10.1007/s00586-020-06676-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-020-06676-1