
Abstract
Ischemic stroke, which accounts for 87% of cerebrovascular accidents, is responsible for massive global burden both in terms of economic cost and personal hardship. Many stroke survivors face long-term disability—a phenotype associated with an increasing number of genetic variants. While clinical variables such as stroke severity greatly impact recovery, genetic polymorphisms linked to functional outcome may offer physicians a unique opportunity to deliver personalized care based on their patient’s genetic makeup, leading to improved outcomes. A comprehensive catalogue of the variants at play is required for such an approach. In this review, we compile and describe the polymorphisms associated with outcome scores such as modified Rankin Scale and Barthel Index. Our search identified 74 known genetic polymorphisms spread across 48 features associated with various poststroke disability metrics. The known variants span diverse biological systems and are related to inflammation, vascular homeostasis, growth factors, metabolism, the p53 regulatory pathway, and mitochondrial variation. Understanding how these variants influence functional outcome may be helpful in maximizing poststroke recovery.
Similar content being viewed by others


Introduction
Stroke is the leading neurological cause of disability-adjusted life years, globally [89]. Every year in the United States, nearly 800,000 people suffer from a new or recurrent stroke with 13.6% of patients expiring, making cerebrovascular accidents the 5th most common cause of death [277]. Fortunately, stroke incidence and mortality are declining, the latter steadily decreasing since the early 1900s, and more notably in the last four decades [150, 156]. Nonetheless, our aging population bears an increased lifetime risk of stroke, rising from 22.8% in 1990 to 24.9% in 2016, with a relative risk increase of 8.9% [336]. Considering that 50% of stroke survivors endure long-term disability, it is not surprising that the economic burden of stroke in the United States is projected to increase from $45.5 billion in 2014 to $129.3 billion by 2035 [79, 277]. Thus, increased efforts to understand, predict, and improve the functional outcome of stroke is essential.
Ischemic stroke (IS), which accounts for 87% of total stroke cases, carries a strong genetic basis with heritability estimates of 39% [22, 277]. The outcome of ischemic stroke is a multifactorial endpoint influenced by clinical and genetic variables [266, 277]. Most studies have implemented a candidate gene approach to examine associations between preselected polymorphisms and disability scores (see Outcome metrics below); however, many of the latest projects have been genome wide association studies (GWAS) attempting to validate prior findings and discover novel variants in a nonbiased fashion.
A comprehensive catalogue of known polymorphisms affecting poststroke recovery would serve as a roadmap for further studies, organizing relevant information for researchers to quickly grasp the state of the field and plan future directions. Furthermore, understanding the genetic underpinnings of ischemic stroke recovery can be leveraged for disability prediction, decision analysis, precision medicine, and drug target discovery. Understanding the polymorphisms and concomitantly affected molecular mechanisms is crucial to fully appreciate the impact on functional outcome. Here, we show that pertinent genes can be grouped by the following systems and processes: inflammation, vascular homeostasis, growth factors, metabolism, p53 regulatory pathway, and mitochondrial variation.
Inflammation
Cytochrome P450 pathway
Cytochrome (CYP) P450s are a class of monooxygenase enzymes that, among other functions, metabolize arachidonic acid (AA) into eicosanoids such as 20-hydroxyeicostetarenoic acid (20-HETE) (Fig. 1). 20-HETE is a potent vasoconstrictor involved in the autoregulation of cerebral blood flow. It is associated with increased IS severity in animal models as well as larger lesions and worse modified Barthel Index (mBI) scores [69, 128, 286]. CYP epoxygenase enzymes also act on AA; however, they produce epoxyeicosatrienoic acids (EETs) that affect cerebral perfusion through vasodilation and offer protective effects against ischemia as opposed to 20-HETE [69, 128].

Depicts the eicosanoid inflammatory pathway. Genes shown in red contain a SNP associated with worse functional outcome. The COX2 locus contains both risk and protective variants which are detailed in the gray boxes. Abbreviations are as follows: thromboxane A2 (TXA2), prostacyclin (PGI2), prostaglandin H2 (PGH2), 20-hydroxyeicostetarenoic acid (20-HETE), epoxyeicosatrienoic acids (EET), and dihydroxyeicosatrienoic acid (DHET)
CYP2C8 and CYP4A11
The synthesis of 20-HETE is catalyzed by enzymes of the CYP4 gene family, while EETs are produced by CYP2C and CYP2J isoforms [128]. Interactions between CYP2C8, CYP4A11, and EPHX2 single nucleotide polymorphisms (SNPs) were associated with IS risk as well as increased 20-HETE and decreased EET [312]. One study in a Chinese population reported a higher frequency of CYP2C8 rs17110453 CC in patients with neurologic deterioration (ND) defined as a change in NIHSS score 10-days after admission. The same report revealed similar findings regarding CYP4A11 rs9333025 GG (Supplemental Table 1) [309].
EPHX2
Downstream in the CYP eicosanoid pathway, EETs are converted to dihydroxyeicosatrienoic acid (DHETs) by soluble epoxide hydrolases (sEH) (Fig. 1). DHETs are generally less bioactive than their precursor, thus sEH acts to reduce the vasodilatory and protective effects of EETs [69, 72, 128]. Accordingly, genetic variants in EPHX2, which encodes sEH, worsen IS outcomes. The missense rs751141 GG variant is independently associated with carotid stenosis [307], plaque density [314], increased metabolism of EET to DHET, and increased ND ten days poststroke leading to worse 3-month modified Rankin Scale (mRS) scores [308, 309].
Cyclooxygenase pathway
COX2
Arachidonic acid is converted to prostaglandin H2 (PGH2) via cyclooxygenases encoded by COX-1 and COX-2. Various tissue-specific isomerases and synthases then generate PGH2 derivatives that trigger diverse biochemical cascades, examples of which include thromboxane A2 (TXA2) and prostacyclin (PGI2), synthesized by thromboxane synthase (TBXAS) and prostacyclin synthase (PTGIS), respectively (Fig. 1) [72]. With respect to cerebrovascular physiology, COX1 is implicated in the maintenance of vascular tone and vasodilator responses and evidence suggests that COX2 increases cerebral blood flow in accordance with neural activity [201, 202].
In addition to studies demonstrating that polymorphisms in COX genes affect IS risk, extensive investigations into how these changes affect functional outcome have also been conducted [326]. One group examined the effects of COX2 SNPs on a variety of functional outcome metrics including mRS, Glasgow Coma Scale (GCS), and BI at 90 days follow-up. Interestingly, they report an association between COX2 rs5275 TC and improved mRS, but not GCS or BI, while COX2 rs20417 GC was associated with better GCS scores but no other metrics [186]. Another group showed that COX-2 rs20417 CC was significant for ND [310] and a different investigation demonstrated that interactions between COX-2 rs20417, P2Y1 rs1371097, and GPIIIa rs2317676 were also associated with ND [311].
TXAS1 and PTGIS
The functional effects of SNPs in PTGIS and TBXAS1 were assessed alongside COX2 polymorphisms: TBXAS1 rs2267679 TT and PTGIS rs5602 CC occurred at a higher frequency in patients with ND. Furthermore, univariate analysis indicated that TBXAS1 rs41708 TT and PTGIS rs5629 CC were independently associated with ND [310].
Toll-like receptors
Toll-like receptors (TLRs) are pattern recognition receptors that are an integral component of the innate immune system and can be activated by exogenous danger-associated molecular patterns (DAMPs) or endogenous ligands produced by disease and injury [140]. TLRs are interconnected with eicosanoid inflammatory pathways and can activate calcium-dependent phospholipase A2 that in turn, produce arachidonic acid-containing phospholipids [72]. Localized to microglial [165] and astrocytic [31] surfaces, TLR4 is implicated in neuroinflammation and stroke recovery [46, 292]. Specifically, increased TLR4 expression at 18–72 h and 7-days poststroke is associated with worse 90-day mRS scores [34, 272, 302]. Although many genetic variants exist in TLR4, two linked SNPs, Asp299Gly and Thr399Ile, occur at significant frequencies, forming the 299/399 haplotype [203]. One study examined the effects of 299/399 on IS functional outcome (ISFO) and found it to be predictive of worse 3-month mRS scores [288]. Proinflammatory markers such as IL-1β, I-L6, and TNFα are associated with TLR4 levels [34, 305] and elevated C-reactive protein 3-months poststroke is associated with 299/399 [288]. Thus, TLR perturbations likely affect other innate immune system processes.
C-reactive protein
C-reactive protein (CRP) is not only an inflammatory biomarker but is also functionally active in compliment activation and Fc receptor binding, the latter of which stimulates cytokine release. Primarily synthesized in hepatocytes, transcriptional induction of CRP occurs in response to inflammatory cytokines including interleukin-6 (IL-6), interleukin-1 (IL-1) and tumor necrosis factor alpha (TNFα) [257]. Elevated CRP is a predictor of cardiovascular disease [67, 334], IS risk [328], and forecasts worse functional outcome (mRS) in acute IS patients according to multiple meta-analyses [127, 281]. Heritability estimates of baseline CRP levels range from 10 to 65% [233] and specific genetic variants affecting CRP levels have been studied in several disease contexts.
Many CRP SNPs have been described; however, only seven have been tested for their effects on ISFO. The minor allele of rs1130864, which is associated with elevated serum CRP in Han Chinese populations [149], demonstrated increased risk for poor outcome (3-month mRS) in the same ethnic group [108], It should be noted that rs1130864 has shown mixed associations with CRP levels in other populations [8, 9, 142, 148, 157], so caution is warranted when assuming the relationship shown in Guo et al. [108] will extrapolate to non-Asian cohorts. Two other SNPs, rs3093059 and rs11265260, were identified as independent risk factors for elevated CRP and worse 3-month mRS scores in Han Chinese patients. In addition, a haplotype analysis of five SNPs including the two previously mentioned was also included in the study and showed significance for poor outcome [306].
Cytokines
IL-1 and IL1RN
Interleukin-1 is an archetypal cytokine involved in a myriad of proinflammatory events that occur during acute brain injury. Pertinent examples include matrix metalloproteinase and platelet activation, augmented angiogenesis, diminished neurogenesis, and the induction of other cytokines [251]. IL-1⍺ and IL-1β are well-studied agonists of the IL-1 type I receptor (IL-1R1), while IL-1 receptor antagonist (IL-1Ra) is a potent endogenous inhibitor [246]. Preclinical studies investigating the therapeutic potential of IL-1Ra administration yielded promising results, yet in clinical trials, the use of IL-1Ra reduced inflammatory biomarkers but failed to show a clear association with improved functional outcome [250, 251]. IL1RN encodes IL-1Ra and contains a variable number tandem repeat polymorphism in which the minor allele (*2) increases IL-1Ra production [68]. Homozygotes (IL-1RN 2/2) had improved clinical outcomes (BI; 7-days, 1-month, 3-months, 1-year) in an IS study [105] and in Rezk et al. which had a cohort composed of patients with intracranial hemorrhage, subarachnoid hemorrhage, and IS [223]. Rezk et al. also reported that a biallelic variant in the promotor region of IL-1β (-511C/T; rs16944), known to increase secretion [217], was associated with worse BI scores at various timepoints out to 6-months poststroke. They demonstrated similar findings for an intronic polymorphism of IL-1⍺ (-889C/T) [223].
IL-6
Interleukin-6 is a pleiotropic cytokine capable of complex, context-dependent functionality [84, 154]. Regarding IS, the exact of role IL-6 remains nebulous. In vivo studies have shown through a variety of approaches including gene knockout [96], intracerebroventricular administration [182, 194], and receptor blockage [299] that IL-6 is neuroprotective [49]. Nonetheless, a plethora of evidence suggests IL-6 is elevated in stroke and is significantly correlated with lesion size [249, 263] and worse functional outcome [12, 42, 237].
A variant in the IL-6 promoter (− 174 G/C; rs1800795) is known to influence IL-6 levels; however, controversy exists regarding which allele increases IL-6 expression and IS risk [152, 268]. One group reported the GG genotype as protective: it was associated with decreased serum IL-6 levels as well as improved 7-day (NIHSS), 3-month (mRS, BI), and 6-month (mRS, BI) outcomes in an Indian population [50]. Contrarily, another study conducted in young patients yielded the opposite findings: the GG genotype was a risk factor for elevated RS at 7-days and 3-months poststroke [102]. The most recent investigation was inconclusive, finding no association between rs1800795 and poststroke IL-6 levels or 6-month mBI [301]. These inconsistencies may be attributed to population differences or experimental biases. Further investigation is warranted to properly elucidate the effects of rs1800795 on ISFO. IL-6 receptor polymorphism Asp358Ala (+ 48,892 A/C; rs8192284) which increases IL-6 levels [337] was shown to improve 3-month mRS scores suggesting that increased IL-6 levels is indeed therapeutic in poststroke recovery [130].
IL-10
Interleukin-10 is generally considered an anti-inflammatory cytokine and is expressed in response to brain injury. It acts by limiting proinflammatory cytokines and effector actions of T cells, monocytes, and macrophages [94]. Preclinical evidence suggest that IL-10 is neuroprotective and reduces infarct volume [24, 26, 169, 172, 256]. With some exceptions [51, 200], clinical studies indicate that low IL-10 levels accompany IS [87, 126, 248] or coincide with acute neurological deterioration [220, 276]. One relevant IL-10 gene promoter polymorphism (–1082 G/A; rs1800896) has mixed evidence regarding its influence on ischemic stroke risk [153, 315]; however, one group did find a significant association between rs1800896 GG and lower BI scores at 1-month and 3-months poststroke [192]. Other SNPs increase IS risk (rs1800872, rs1554286, rs3021094) [297], but remain untested in the context of functional outcome [155].
RETN
Resistin is a pro-inflammatory, atherogenic adipokine associated with acute cerebral infarction independent of obesity-related pathways [206]. Elevated serum resistin was linked to 5-year mortality and poststroke disability (mRS) [82, 163]. The -420 C/G (rs1862513) polymorphism in the promoter region of RETN leads to increased resistin levels [58, 162, 207]. Bouziana et al. reported that carriers of the minor allele present with more severe IS and experience higher in-hospital mortality [30]. Interestingly, the same group also found an association between -420G and improved 1-year mRS scores. The authors postulate the contradiction stems from selection bias whereby -420G carriers who endure increased risk of acute death may create artificial associations with long-term recovery [29].
circ-STAT3
Noncoding, circular RNAs (circRNAs) are ubiquitous in neural tissue and differentially expressed in stroke patients with subtype-specific profiles [78, 178, 208]. One group was able to predict IS outcomes by measuring only three circRNAs, thus demonstrating robust biomarker potential [333]. A growing number of associations between circRNA variants and human disease includes connections to atherosclerosis [41], multiple sclerosis [210], and coronary artery disease [330]. The only study investigating functional recovery reported that circ-STAT3 rs2293152 GG worsened poststroke disability (3-month mRS) [180]. Signal transducer and activator of transcription 3 (STAT3) molecules are regulated by Janus kinases 2 (JAK2). JAK2/STAT3 activation exacerbates neuroinflammation and inhibition of this pathway can mitigate cerebral ischemic injury and decrease infarct size after stroke [331]. Liu et al. posits that rs2293152 GG influences STAT3 levels by altering circ-STAT3 expression, or by modifying its ability to bind regulatory miRNAs [180].
Myeloperoxidase
Myeloperoxidase (MPO) is a heme-containing enzyme found in primary azurophilic granules of neutrophils. MPO augments innate immune system defense via production of reactive oxygen species (ROS) such as hypochlorous acid [11]. Considering that exuberant ROS production leads to host tissue damage, and that MPO levels increase poststroke [61], MPO inhibition as a therapeutic strategy has been posed and successfully tested in animal models [146]. A candidate gene approach was employed to examine the effects of MPO polymorphisms on ISFO and G463A (rs2333227) was associated with worse RS scores at follow-up (median interval: 11 days) [125]. Another variant, rs2107545 CC, led to poor 6-month outcomes (mRS, BI) [175].
Vascular homeostasis
Hemostasis
GPIIIa
Normal platelet functioning is essential for primary hemostasis and thrombosis [214]. Elevated platelet markers in early cerebrovascular studies led authors to postulate that increased platelet activity may be pathogenic, at least in certain stroke subtypes [238, 270, 271]. This notion meshes well with the contemporary practice of antiplatelet administration for treatment and prophylaxis of ischemic events. Platelet adhesion and aggregation is orchestrated in part by integrins, a class of glycoprotein signaling receptors [129]. The constellation of integrin species on human platelets includes αIIbβ3. This transmembrane protein offers binding sites for hemostasis-related ligands such as Von Willebrand factor, fibrinogen, fibronectin, and CD40 [229]. Experiments in nonhuman primate models showed microvascular preservation after αIIbβ3 inhibition, so genetic alterations to GPIIa and GPIIIb which encode the αIIb and β3 subunits may affect stroke outcome [5, 47, 129].
While multiple groups have reported that genetic variants in GPIIb/GPIIIa affect IS risk, evidence of their influence on functional outcome is less robust [176]. Initial investigations revealed that poststroke mortality is affected by the HPA-3 genotype of GPIIb with 80% of bb carriers surviving at follow-up, compared to 68% of ab, and 58% of aa carriers [47]. Another study showed that the A2 allele of GPIIIa rs5918 was significantly associated with poor BI scores at 90-days postadmission, but not mRS or GCS grades [186]. As previously mentioned, interactions between GPIIIa rs2317676, COX-2 rs20417, and P2Y1 rs1371097 were significant for ND ten days after admission [311]. P2Y1 is a G protein-coupled receptor classically known to activate platelet aggregation, but also participates in neuroinflammatory processes via IL-6 induction [92, 316]. These molecules certainly contribute to stroke pathophysiology considering that P2Y1 receptors are upregulated during cerebral ischemia and infarct size is reduced after P2 receptor antagonism [159, 269].
⍺2AP
Alpha-2-antiplasmin (⍺2AP) influences fibrinolysis via plasmin deactivation [1]. One ⍺2AP mutation, Arg407Lys (rs1057335), is associated with cardiovascular disease as demonstrated in Bridge et al. where carriers of 407Lys were at decreased risk for abdominal aortic aneurysm [35]. Relating to cerebral ischemia, a multivariate analysis indicated that IS and transient ischemic attack (TIA) patients with the minor allele were more likely to have long-term functional recovery (mRS, 6–12 months). These findings suggest a protective role for Arg407Lys, but the exact mechanisms underlying this effect remain obscure [296].
eNOS
Nitic oxide (NO) is a lilliputian signaling molecule and orthodox vasodilator with anti-proliferative and anti-thrombotic properties [88]. NO also facilitates synaptic plasticity and is neuroprotective at physiologic concentrations yet neurotoxic at higher levels [44]. Three isoforms of nitric oxide synthase (NOS) produce NO including endothelial (eNOS), neuronal, and inducible versions. NOS requires several cofactors including tetrahydrobiopterin (BH4), the synthesis of which is governed by rate-limiting enzyme, GTP cyclohydrolase 1 (GCH1) [90]. Polymorphisms affecting eNOS and GCH1 have been linked to adverse poststroke outcomes (Fig. 2a). For example, G894T (rs1799983) is a missense variant altering the active site of eNOS. Asian carriers of the T allele endure increased risk of IS, unlike Caucasians [56, 151]. However, one study found that Mediterranean patients with the mutation have worse functional outcomes (1-month mRS) [83]. Regarding GCH1, + 243C/T is a SNP in the 3'-UTR that decreases NO production leading to increased vascular events and death after IS (5-year follow-up) [262, 319].

has two components: a and b. a Shows the molecular pathway for nitric oxide (NO) synthesis and shows that genetic variants in GCH1 and eNOS lead to adverse outcomes after stroke. ✢ placed to clarify that the GCH1 variant led to death after IS but was not associated with a functional outcome metric. b Shows pathway for angiotensin II type 1 receptor (AT1R) agonism which is augmented by an angiotensin converting enzyme (ACE) polymorphism and leads to worse poststroke recovery
Atherosclerosis
ACE
The renin angiotensin system (RAS) is integral to vascular homeostasis and is also active in brain parenchyma, influencing learning and memory [65]. In the classical RAS axis, angiotensin converting enzyme (ACE) cleaves angiotensin I to produce the angiotensin II (ang II) (Fig. 2b). Overactivation of ang II type 1 receptor (AT1R) is implicated in stroke pathogenesis via proinflammatory, profibrotic, and vasoconstrictive effects. Increased oxidative stress also contributes to these proatherosclerotic changes [14]. ACE is a key player in aberrant RAS activity as evidenced by studies wherein pre-stroke ACE inhibition reduced ischemic stroke incidence [120] and severity [57], and improved poststroke recovery (BI at discharge) [116]. A 287-bp insertion/deletion (I/D) polymorphism within the ACE gene is known to affect serum ACE levels. Carriers of the D allele possess higher levels of ACE [224], incur increased risk of IS [323], and are subject to worse functional outcomes (BI at discharge) [189].
HDAC9
Histone deacetylases (HDACs) remove acetyl groups from lysine residues on histones and other regulatory proteins, promoting a heterochromatic configuration that dampens transcriptional activity [110]. HDAC inhibition is a common therapeutic approach and has shown promise in preclinical stroke models [160]. Several variants at the HDAC9 locus are associated with IS risk [111, 164, 267, 335]. Two of these variants, rs2074633 and rs28688791, are associated with unfavorable short-term outcome (3-month mRS) and are in linkage disequilibrium with another risk SNP, rs2107595 [282]. This variant is associated with common carotid intimal thickness, the presence of carotid plaque, and increased HDAC9 expression [17, 191]. Mechanistic studies found that HDAC9 represses cholesterol efflux and promotes atherosclerosis [45].
TNFRSF11B
Osteoprotegerin (OPG) is a member of the tumor necrosis receptor superfamily with roles in bone homeostasis, vascular inflammation, and calcification [274]. Whether OPG activity is beneficial or harmful in the context of vascular disease remains unclear. While OPG knockout accelerates calcific atherosclerosis in certain animal models [40], suggesting protective effects, preclinical stroke models showed reduced infarct volume and brain edema in OPG−/− mice, indicating a pathogenic role for OPG in cerebrovascular disease [240]. Clinically, OPG levels positively correlate with stroke severity [46], mortality [132], and poor functional outcome (3-month mRS) [254]. Two genetic variants in TNFRSF11B, which encodes OPG, are associated with increased serum OPG levels [260], IS occurrence [25], and worse poststroke recovery (rs2073617G, rs3134069C; 3-month mRS) [283]. In silico analysis projected that these SNPs are in histone modification regions, hence the altered OPG levels [283].
PDE4D
Cyclic adenosine monophosphate (cAMP) is a ubiquitous second messenger generated by adenylyl cyclase that facilitates diverse cellular processes in response to various stimuli. The breakdown of cAMP to inactive AMP is catalyzed by phosphodiesterase (PDE) enzymes [234]. A connection between stroke and PDEs was discovered when Gretarsdottir et al. reported that certain PDE4D haplotypes were associated with IS susceptibility. The authors posited atherosclerosis-related mechanisms as an explanation considering the strongest associations were among cardiogenic and carotid stroke subtypes [103]. A decade of additional studies summarized by meta-analysis confirmed that some PDE4D variants are indeed related to stroke [181]. And while cAMP does inhibit a variety of proatherosclerotic changes in vascular smooth muscles cells including proliferation [131], migration [95], and collagen deposition [81], it also mitigates neuroinflammation and increases BDNF expression [298]. PDE4D variant, SNP87 (rs2910829), although not related to IS incidence overall [170], was found to worsen functional outcomes (3-month mRS) [255].
OPN
Osteopontin (OPN) is a multifunctional phosphoglycoprotein that guides numerous signaling pathways and in the context of acute brain injury, balancing pro-inflammatory and anti-inflammatory responses to modulate neuroinflammation, apoptosis, and blood–brain barrier (BBB) integrity [329]. Some evidence also suggests that OPN potentiates atherosclerosis [294]. Nonetheless, several in vitro studies have indicated a neuroprotective role for OPN; specifically, OPN administration reduced infarct volume and lessened neurologic deficits in rodent models of IS [134]. Clinically, however, elevated OPN is associated with worse outcomes (3-month mRS [195], recurrence [93]). This correlation may be a reactive phenomenon in which compensatory increases in OPN occur in patients with more severe stroke. OPN polymorphism -443 C/T (rs11730582) was examined in IS patients and investigators reported that -443 CC was associated with decreased levels of a particular OPN isotope and that CC homozygotes experienced worse long-term functional recovery (12-month mRS and BI) reinforcing the notion that OPN is neuroprotective [135].
Growth factors
BDNF
Brain-derived neurotrophic factor (BDNF) is a highly expressed protein involved in numerous nervous system activities including neuroinflammation, neuronal survival, and plasticity [19]. BDNF administration in stroke animal models has demonstrated various benefits including reduction of infarct size [235] and improved functional outcome [198]. In humans, BDNF levels are negatively correlated with NIHSS scores [139] and low initial quantities are associated with worse mRS outcomes at 90-days [161, 280], 2-years, and 7-years poststroke [258].
BDNF is initially synthesized as a precursor protein (proBDNF) that is cleaved to separate a mature domain (mBDNF) and prodomain. All three molecules are bioactive and exhibit distinct, even opposing effects due to differing receptor affinity [71]. Among multiple SNPs in the BDNF gene, val66met (rs6252; G196A), which occurs in the prodomain, is the most studied variant in the context of IS. Molecularly, val66met reduces activity-dependent secretion of BDNF [18].
Val66met is implicated in the pathogenesis of many neuropsychiatric disorders [123] and multiple groups have reported associations with IS occurrence [141, 325, 327]. In aneurysmal subarachnoid hemorrhage, met66 is a negative prognostic factor [244]. Several studies have investigated the effects of val66met on ISFO, some of which are aggregated in a meta-analysis that reports an overall significant association between the met allele and unfavorable outcome as defined by study-dependent mRS cutoff values [193]. Nonetheless, other publications utilizing mRS as an outcome metric have yielded mixed results with some groups reporting negative findings [141]. Recently, two studies of large cohorts reported contrasting findings: Braun et al. found that poor outcome (mRS ≥ 3) was associated with met66 (n = 829) in a young American population (average age = 41.4) [33], while Zhou et al. described no such association in a Han Chinese population (mRS ≥ 2; n = 778; average age = 64) [327]. Differences in study parameters and population demographics may account for the incongruity.
Aside from mRS, other outcome measurements have bolstered the case for val66met as a risk factor for IS recovery. BI at 6-weeks postrehabilitation [232] and cognitive functional independence Measure (FIM) at discharge [112] are more likely to be compromised in patients carrying the met66 allele. In addition, more granular phenotypes have been studied as well. Specifically, val66met is associated with decreased motor function [52] and improvement [242, 278], rate of adaptation [122], and sensorimotor cortex activation after stroke [145]. In patients with dysphagia, the met66 allele was originally described as protective [85]; however, new evidence suggests the opposite [204]. Other BDNF SNPs, although less studied than val66met, have also been linked to poststroke disability. For example, rs11030119 is an intronic variant associated with favorable 7-year mRS [259]. And rs7124442, which is located the 3'-UTR and affects miR-922 binding, is significant for increased BDNF expression and improved NIHSS scores at 3-months poststroke [174].
IGF1
Insulin-like growth factor 1 (IGF1) is a polypeptide hormone that activates signaling pathways to promote growth, neurodevelopment, and neuroplasticity [295]. IGF1 decreases with age [138], but remains an important neuroprotective agent as evidenced by clinical studies that, minus one exception [13], show elevated serum IGF1 levels correlating with improved functional outcomes in stroke patients [2, 70]. In vivo stroke models also support this notion: IGF1 administration reduces infarct volume [236]. Regarding IGF1 genetics, multiple SNPs have been identified in addition to a 192 base pair CA repeat polymorphism in the promoter region that increases serum IGF1 concentrations [273] and decreases IS risk [225]. With respect to functional outcome, one study demonstrated that rs7136446 was significantly associated with lower IGF1 levels in healthy controls and worse mRS scores 2-years poststroke [3].
VEGF
Vascular endothelial growth factor (VEGF) is a signaling protein that stimulates angiogenesis and is neuroprotective as evidenced by preclinical models wherein VEGF administration reduces infarct volume and cognitive deficits after ischemic events [101]. Polymorphisms in VEGFA have been linked to cardiovascular disease including stroke [147, 285]. Regarding functional outcome, one group reported that + 936C/T (rs3025039) led to worse IS outcomes (3-month mRS) and that this variant is in linkage disequilibrium with nearby SNP, + 1451C/T (rs3025040), both of which occupy the 3'-UTR. Subsequent experimentation revealed that + 1451C/T lies within a crucial binding cite for regulatory miRNAs (miR-199a, miR-199b) with the minor allele decreasing miRNA binding affinity and reducing VEGFA expression [324]. A variant in the VEGFA receptor, VEGFR2 (+ 1719A/T; rs1870377T/A; Q472H), elevates serum VEGF [245], increases microvessel density [97], and improves 3-month mRS scores [168].
ANGPT1
While VEGF promotes early angiogenesis, Angiopoietin 1 (Ang1) acts later by decreasing vascular permeability and inflammation, leading to BBB preservation and periinfarct neovascularization after ischemic injury in preclinical studies [113, 265]. Accordingly, ischemic stroke patients with low plasma Ang1 levels at admission had worse 3-month mRS scores [98]. Two SNPs in the ANGPT1 3'-UTR reportedly alter IS risk, one of which also worsened poststroke recovery in a Chinese population (rs2507799; 1-month mRS) [53, 54]. Differential binding of miR-607 potentially explains why carriers of the T allele had decreased plasma Ang1 and poorer outcomes [53].
Metabolism
APOE
Apolipoprotein E (APOE) is a ubiquitously expressed glycoprotein found in a variety of central nervous system cell types, facilitating the transport and metabolism of cholesterol and other lipids [300]. After being secreted from cells, APOE becomes lipid-bound and carries cargo molecules to neuronal cell-surface APOE receptors such as low-density lipoprotein receptor (LDLR). Polymorphisms in two critical positions on the APOE gene generate three allelic variants: ε2, ε3, and ε4. APOE ε2 (APOE2) binding to LDLR is 50 times weaker than the other alleles, while APOE4 has enhanced binding to very low-density lipoprotein (VLDL) particles [300]. Consequently, pathologies are dichotomized by deficient or excessive lipoprotein processing. In the periphery, APOE2 is associated with Type-III hyperlipoproteinemia, and APOE4 with proatherogenic lipoprotein conditions [216, 300]. In brain parenchyma, APOE is involved in cerebrovascular function, glucose metabolism, and synaptic integrity and plasticity although the exact mechanisms underlying these relationships are poorly understood [300].
APOE4 genotype is a major risk factor for Alzheimer’s disease (AD), increasing Aβ plaque formation [219]. Contrarily, APOE2 is protective for AD and associated with reduced plaque burden [64]. APOE impacts cerebrovascular disease as well: cerebral amyloid angiopathy (CAA), which is modulated by APOE4 [222], increases risk for lobar intracranial hemorrhage (ICH) [230], the severity of which is impacted by APOE2 [39]. Although APOE influences IS risk [143], its effect on poststroke disability remains controversial.
Several studies have examined the relationship between APOE4 genotype and ISFO. A recent meta-analysis of relevant publications from 1998 to 2012 reported no overall statistically significant association [193]. This analysis included measurements from a variety of timepoints (1-month, 3-months, 1-year), quantified by various metrics (NIHSS, BI, RS, mRS, FIM, mortality). Another group reported negative findings regarding functional outcome, but found that males with the APOE4 allele endured higher 1-year mortality, poststroke [104].
Further negative findings outside of those encompassed in the meta-analysis include additional studies reporting no association between APOE4 and RS [185], or APOE4 and mRS [158, 289, 321]. Interestingly, APOE4 decreases age of ischemic stroke onset [158], and specific cognitive testing has shown that APOE4 delays the recovery of verbal memory functioning 1-year poststroke [289]. In addition, ε4 homozygosity leads to poststroke dementia [213]. Nonetheless, underwhelming evidence exists regarding the effects of APOE4 and ISFO.
APOE2 is less studied in the context of stroke outcome. Broderick et al. found that ε2 carriers treated with t-PA had better 3-month outcomes (mRS) [36]; however, a general effect on poststroke recovery has not been shown [321], only a sex-specific association whereby male carriers of the ε2 allele experienced increased disability (3-month mRS) [158].
MTHFR
Homocysteine is a member of the sulfur-containing amino acid metabolic pathway. Methylene tetrahydrofolate reductase (MTHFR) regenerates N5-methyl-tetrahydrofolate, so homocysteine can be used to replenish methionine, an essential amino acid (Fig. 3) [38]. Alterations to MTHFR efficiency can cause homocysteine buildup resulting in a multitude of pathologic effects including endothelial dysfunction, ROS generation, DNA repair suppression, and increased apoptosis [166]. Two well-studied variants, C667T and A1298C, reduce enzyme activity by 75% and 39%, respectively in homozygous carriers [279]. Both mutations increase ischemic stroke risk [4, 77] but have no known associations with poststroke recovery. He et al. examined rs868014, a SNP in the 3'-UTR, and reported increased miR-1203 binding leading to decreased MTHFR expression, heightened serum homocysteine, increased stroke incidence and severity, as well as worse functional outcomes (3-month ΔNIHSS). Interestingly, rs868014 was linked to A1298C [118].

Depicts methionine regeneration and its dependence on methylene tetrahydrofolate reductase (MTHFR), a genetic variant of which leads to worse functional outcomes after stroke. THF is abbreviation of tetrahydrofolate
COMT
Catechol-O-methyltransferase (COMT) metabolizes dopamine and thus inhibits its activity in the synaptic cleft [291]. Dopamine, which massively increases during ischemic stroke onset, influences motor activity, memory, and cognition among other functions. While dopamine-enhancing drugs almost universally improve sensorimotor function in a variety of animal stroke models, clinical trials have failed to reproduce the same success: dopamine augmentation failed to improve general disability tests such as BI in most trials and showed mixed results when motor-specific scales were used as outcome variables [100]. COMT contains a key polymorphism, val158met (rs4680), that decreases enzymatic activity, increasing dopamine in the synaptic cleft by as much as 38% [291]. This variant significantly worsens BI and Rivermead Motor Assessment (RMA) at 1-month and 6-months poststroke as well as FIM and Fugl-Meyer Assessment (FMA) at 3-months and 6-months poststroke [144, 171]. These findings suggest a harmful role of excess dopamine in IS recovery that contradicts preclinical models.
NOX4
NADPH oxidase (NOX) enzymes generate ROS that propagate redox dependent signaling pathways to execute numerous physiologic functions [275]. ROS abundance is an essential component of stroke pathophysiology causing lipid peroxidation, DNA damage, and apoptosis [205]. NOX4 is induced under hypoxic conditions and is especially harmful during cerebral ischemia [48]. NOX4 variant rs11018628 TC/CC is associated with decreased IS risk and improved functional recovery (ΔNIHSS at discharge) [119].
Hypothalamic-pituitary-thyroid axis
Tightly controlled by a precise feedback loop known as the hypothalamic-pituitary-thyroid (HPT) axis, thyroid hormones affect metabolism, development, and growth, influencing virtually every cell in the human body. The HPT axis is as follows: thyrotropin-releasing hormone (TSH) generated in the hypothalamus causes thyroid-stimulating hormone (TSH) secretion in the hypophysis, precipitating T3 and T4 synthesis in the thyroid gland at a 1:14 ratio. T4 is converted to the more biologically active T3 by deiodinase enzymes in extrathyroidal tissues [184]. Many studies investigating interplay between thyroid hormones and stroke outcome have been conducted. One meta-analysis revealed an overall association between poor mRS scores and low T3 levels [133]. Decreased T3 has also been associated with increased 1-year mortality [7] and worse NIHSS scores (~ 2–4 weeks) [322]. Thus, T3 appears to be neuroprotective in acute cerebrovascular disease. Regarding other HPT hormones, high T4 is prognostic for long-term disability [133] and although individual studies report mixed findings regarding the effects of TSH on ISFO, a meta-analysis found that initially elevated TSH levels improved 1-month and 3-month mRS scores [74].
DIO3
Given the impact thyroid hormones have on IS outcome, genetic variants affecting their transport and activity were postulated to influence poststroke disability. Deiodinase 3 (DIO3) is an enzyme that inactivates T3 in neurons—a process induced by hypoxic conditions [136]. One group found that DIO3 SNP rs945006 TT was associated with improved ISFO at 1-year follow up (mRS) [264]. The mechanisms by which rs945006 affects intraneural DIO3 activity are currently unknown.
OATP1C1
Organic anion transporting polypeptide 1C1 (OATP1C1) is a transmembrane protein specific for thyroid hormone transport in the brain and animal models indicate that inflammation reduces OATP1C1 mRNA expression in cerebral blood vessels [21, 293]. One group reported a relationship between rs10770704 CC and increased disability 1-year poststroke (mRS) [264], despite multiple studies reporting no direct effect of the SNP on thyroid hormone levels [73, 227].
p53 regulatory pathway
TP53 and MDM2
Neuronal apoptosis is a determinate of penumbra progression and highly influenced by the p53 regulatory pathway. A variety of stress signals including hypoxia and DNA damage can trigger p53 activation leading to cellular death, while p53 attenuation is therapeutic in animal models of IS [124]. Genetic variants affecting p53 and its regulators and downstream targets have been implicated in poststroke recovery. The arg72pro (rs1042522) SNP of TP53, which encodes p53, alters its proapoptotic functionality. Arg72 augments apoptosis, a seemingly hazardous modification for IS patients considering the arg/arg genotype worsens poststroke disability (3-month mRS) [99]. Murine double minute 2 (MDM2) is an E3 ubiquitin protein ligase and direct negative regulator of p53 (Fig. 4). The minor allele of MDM2 SNP309 (rs2279744) increases MDM2 expression, downregulates p53, and improves 3- and 12-month mRS scores [226] at the cost of increased tumor formation [27].

illustrates the various components of the p53 regulatory pathway and relevant polymorphisms associated with ISFO. Red arrows indicate negative regulation and the dotted arrow from p53 to XRCC1 denotes the indirect relationship between the two. ✢: as noted above, numerous MMP2 SNPs were found but did not endure Bonferroni correction
TUG1
Taurine-upregulated gene 1 (TUG1) is a long non-coding RNA induced by p53 and upregulated in IS (Fig. 4). In vitro studies indicate that TUG1 knockdown reduces neuronal apoptosis in oxygen–glucose deprivation (OGD) models, while decreased TUG1 expression is associated with worse cancer outcome metrics [55, 317]. One group showed that the C allele of rs2240183, a SNP in the TUG1 promoter region, led to increased TUG1 expression and IS risk which is in align with the aforementioned preclinical evidence [287]. However, Liu et al. reported the CC genotype as protective with respect to 3-month mRS scores [179], thus further investigation is required to confirm the effects of rs2240183 on TUG1 activity and resultant changes in IS risk and outcome.
WRAP53 and XRCC1
Ischemia–reperfusion injuries after stroke generate ROS leading to DNA damage [167]. WD40-encoding p53-antisense RNA (WRAP53) is a regulatory RNA that facilitates p53-mediated DNA repair and apoptosis (Fig. 4) [188]. Relating to stroke, it has been shown that WRAP53 is translocated to the nucleus upon hypoxic injury where it is essential for the assembly of DNA repair-related proteins and neuronal survival. A coding variant of WRAP53 (rs2287499; arg68gly) increases the rate of nuclear translocation and thus enhances repair. Homozygous carriers of the less efficient arg68 allele have larger infarct volumes and worse functional outcomes (3-month mRS) after IS [231]. X-ray repair cross-complementing protein 1 (XRCC1) is a scaffold protein for DNA repair enzymes integral to the DNA single strand break repair pathway [75], and in the context of base excision repair, is indirectly regulated by p53 (Fig. 4) [218]. In functional outcome studies, XRCC1 SNP rs25487 was shown to reduce IS susceptibility and improve short-term recovery (ΔNIHSS from admission to discharge) [117].
MMP2
Matrix metalloproteinases are proteolytic enzymes that cleave extracellular matrix proteins to aid in cell motility, tissue remodeling, and inflammatory responses [209]. In stroke, acute hypoxemia triggers MMP2 release from astrocytes and subsequent degradation of BBB integrity. If reperfusion is not accomplished, free radicals induce MMP9 production in microglia and pericytes further damaging the cerebrovasculature [304]. Accordingly, MMP inhibition abrogates BBB insult [228] and reduces apoptosis [107] in preclinical models. In addition, MMP2 and MMP9 exhibit intranuclear activity and can degrade DNA repair proteins including XRCC1, worsening DNA damage after ischemic events (Fig. 4) [303]. Evidence suggests that p53 regulates both MMP2 and MMP9 expression [23, 196]. Regarding ISFO, one study reported significant associations between nine MMP2 variants (Supplemental Table 5) and 3-month mRS scores after leveraging linkage disequilibrium parameters. These associations did not persist after Bonferroni correction [190]. Although no associations with MMP9 were discovered individually, gene–gene interactions between TP53 rs1042522, MDM2 rs2279744, and MMP9 rs3918242 were significant for ND (10-day NIHSS increase ≥ 2) and increased poststroke disability (3-month mRS) [313].
Mitochondrial variation
Haplogroups and UCP2
Mitochondria enable oxidative phosphorylation and are intimately involved in apoptosis, both of which are key processes affecting cell survival under ischemic conditions [247]. As a result, perturbations of the mitochondrial genome or nuclear genes encoding mitochondrial proteins impact poststroke recovery. Specifically, haplogroups N9 [43] and R0 [66] are protective for ND (14-day and 1-month ΔNIHSS, respectively), but are otherwise unstudied in the context of stroke. The association with N9 was identified in an pure IS cohort [43], while Cramer et al. discovered the R0 association in a population composed of 77% ischemic stroke patients [66]. With respect to nuclear DNA, one group found a highly protective variant (-866G/A, rs659366) in the UCP2 gene which encodes uncoupling protein 2, localized to the inner mitochondrial membrane. After recanalization, patients with the AA genotype were twenty times more likely to be functionally independent (3-month mRS). Preclinical studies suggest the uncoupling action of UCP2 reduces ROS generation and the A allele of -866G/A increases UCP2 expression [32, 76, 86].
mtDNA-CN
Mitochondrial DNA copy number (mtDNA-CN) is a proxy for mitochondrial function and has been linked to cardiovascular disease, neurodegeneration, and aging [183]. Low mtDNA-CN is associated with increased stroke incidence, severity, disability (1- and 3-month mRS), and mortality [16, 59, 253]. While the exact mechanism underlying these associations remains unclear, a role for mtDNA-CN in BBB preservation and inflammatory modulation has been postulated [59].
Genome-wide association studies
PATJ
As the name suggests, PALS1-associated tight junction protein (PATJ) is a macromolecule involved in tight junction formation and epithelial cell polarity [241]. PATJ is also implicated in the PI3K-Akt signaling pathway [20]. Previously unrelated to stroke, a recent meta-analysis of genome-wide association studies (GWAS) found 18 low-frequency intronic SNPs in the PATJ locus to be significantly associated with 3-month mRS scores. An additive model suggested that every G allele of the lead variant, rs76221407, led to a 0.4-point increase in mRS score [197]. It has been hypothesized that the mechanisms through which PATJ perturbations affect poststroke disability are related to altered angiogenesis, axonal regeneration, and BBB continuity [284].
LOC105372028
OC105372028 is an understudied gene of unknown biological significance. Söderholm et al., conducted a meta-analysis of GWAS data and established a connection between rs1842681, a variant at the locus, and ISFO (3-month mRS) albeit with a small effect size (OR = 1.12–1.40) [252]. The authors speculate that LOC105372028 affects brain plasticity through regulatory actions on PPP1R21 which in turn modulate protein phosphatase 1 (PP1) levels. PP1 is involved in many nervous system behaviors including learning and memory [199].
PTCH1
Söderholm et al. also reported suggestive findings regarding PTCH1 SNP, rs2236406 [252]. Although statistical significance wasn’t achieved, another group employed a candidate gene approach in a Chinese population to confirm its association with 3-month mRS [332]. PTCH1 is a cell surface receptor that initiates Sonic hedgehog (Shh) signaling which is canonically related to cellular differentiation and organogenesis, but also implicated in poststroke neurogenesis and recovery [320].
Structural variation
Genome wide approaches have also highlighted the impact of genetic imbalance on stroke outcome. Copy number variations (CNV) are large scale genomic alterations that can occur as benign polymorphisms or drive pathology in human disease [318]. CNV has been extensively studied in the context of vascular disease and is associated with increased stroke risk as well as certain stroke subtypes [106]. CNV of dose-sensitive genes independently contributed to unfavorable outcomes in IS patients (3-month mRS) [215]. Future studies aim to further elucidate the impact of CNV on stroke risk and outcome [62]. Mosaic loss of chromosome Y (mLOY) is an insidious progression of aneuploidy in somatic cells. Traditionally considered a marker of aging, mLOY has recently been linked to various pathologies including cancer, Alzheimer’s disease, and cardiovascular disease [109]. Recently, an mLOY polygenic risk score was associated with worse ISFO (3-month mRS) [137] (Fig. 5).

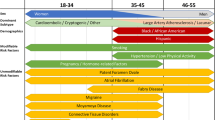
Maps genetic variants associated with 90-day mRS to a chromosomal ideogram. If the locus is bold, then the threshold for favorable outcome is mRS < 2, otherwise, the cutoff is mRS < 3. Red text indicates risk variants, while green text signifies protective variants. The font size of loci names is unchanging; however, the font size of a particular variant at that locus scales with absolute odds ratio. Absolute odds ratio permits protective and risk variants to be scaled together. For example, UCP2 rs659366 lessens likelihood of poor functional outcome with an odds ratio of 0.05, or absolute odds ratio of 20, therefore, it is given the largest font size and is colored green to indicate a large protective effect
Conclusions
Diverse biological processes are involved in poststroke recovery. Genetic alterations in pertinent systems can influence functional outcome as described by metrics such as mRS. Significant polymorphisms have been identified in genes related to the eicosanoid inflammatory pathway including those encoding cytochromes, cyclooxygenase, epoxide hydrolase, prostacyclin synthase, and thromboxane-A synthase. Altered proteins related to innate immunity including toll-like receptors, interleukins, C-reactive protein, and myeloperoxidase also affect IS outcome. Noncoding RNA variants regulating cytokine signaling are relevant as well. Proteins involved in primary hemostasis like GPIIIa and P2Y1 are vulnerable to genetic mutations affecting this phenotype, as are atherosclerosis-related proteins such as angiotensin converting enzyme. Significant variants have been found at the APOE, BDNF, and IGF1 loci, indicating that appropriate lipid metabolism and normal growth factor behavior are both crucial for poststroke recovery. Members of the HPT axis including dioxygenases and organic anion transporters have also been implicated. Several elements of the p53 pathway affect poststroke disability as well as various mitochondrial perturbations; markers of structural imbalance such as CNV and mLOY are among the most recently discovered effectors of stroke outcome.
Although these systems seem disconnected, links between different pathways may exist (Fig. 6). For example, IL-6 stimulates CRP secretion [121]. Thus, stroke recovery in patients with only the relevant IL-6 polymorphism (rs1800795) may have additional risk insofar as differential IL-6 levels could functionally mimic CRP rs1130864 which increases CRP levels in Han Chinese populations and leads to worse outcomes. In addition, there is evidence of IL-6-dependent secretion of prostaglandin E2 (PGE2)—a member of the cyclooxygenase pathway—in inflammatory states [28]. IL-6 also activates the hypothalamic–pituitary–adrenal axis which interacts with the HPT axis, so similar connections may exist between those systems as well [60, 211]. Further complexity can be postulated given that other inputs, such as P2Y1 receptor signaling [92] or decreased COMT activity [114], induce IL-6 release. As a result, changes in primary hemostasis or catecholamine metabolism may alter cytokine activity and thus function as a proxy for genetic variants in multiple systems [115]. TLR4 activates NF-κB signaling which stimulates the release of multiple inflammatory cytokines including IL-6 which may explains its large effect size on ISFO [177]; HDAC9 and TSH activate NF-κB signaling as well [10, 15]. BDNF also exemplifies the interconnectedness of these systems. Significant interactions between BDNF val66met and COMT val158met were reported in a study examining cortical plasticity [292]. Mechanistically, this can be explained by the fact that COMT val158met increases dopamine levels in the synaptic cleft [291] and that dopamine receptor activation increases BDNF expression [290]. There is also evidence that BDNF is induced by T3, suggesting a connection with the HPT axis [261].

Demonstrates potential interconnections between some of the biological systems implicated in ISFO. Arrows from one component to another are color-coded: black represent induction, grey indicates NF-κB signaling, and red denotes negative regulation. ✢: decreased COMT, specifically, induces IL-6 release
Studies investigating the genetics of ISFO have mostly utilized a candidate gene approach for which preselected variants are examined for associations with various outcome metrics. The limitations of this methodology include selection bias, high false positive rate, and low genetic coverage [63, 80]. Considering most studies related to this topic have employed a candidate gene approach, reported findings should be interpreted with appropriate caution. In 2017, the Genetics of Ischaemic Stroke Functional Outcome (GISCOME) network was established to pool genotypic and phenotypic data from multiple institutions to foster large-scale, genome-wide association studies [187]. Söderholm et al. was the first GWAS examining functional outcome using the GISCOME dataset and found a single significant intronic variant (rs1842681) which is not obviously related to polymorphisms previously identified by candidate gene studies. Mola-Caminal et al. also found a novel locus, PATJ [197], and aside from PATJ and IGF1 both contributing to the PI3K-Akt signaling pathway, there is no clear connection to prior genetic variants of interest. As shown here, no loci identified through candidate gene studies have been recapitulated by the recent GWAS which may indicate marginal significance of canonical variants, highlight the heterogeneity of population-specific associations, or reflect the shortcomings of a candidate gene approach. Cross validation experiments as seen in Zhu et al. [332] where suggestive GWAS findings were confirmed using a candidate gene approach are necessary to reinforce suspected variants.
Overall, our search identified 74 genetic variants spanning 48 features are associated with ISFO. Most variants led to worse functional outcome, while nearly twenty variants appear to have protective effects (Supplemental Table 1, 2, 3, 4, 5, 6, 7). Within a single locus, some SNPs may worsen outcome, while others improve it. No pattern is observable, it simply depends on what mechanisms are altered. Among studies that used mRS as an outcome metric, SNPs of UCP (OR = 0.05), IL-6 (OR = 0.1), and TUG1 (OR = 0.499) were the most protective, while variants at the TLR4 (OR = 14.16), CRP (OR = 4.70), and TP53 (OR = 3.89) loci increase risk the most (Fig. 5).
While the literature regarding ISFO has significantly expanded in recent years, further investigation is required to verify the genetic variants discovered thus far and elucidate connections between different biological systems. For precision medicine to become practical in poststroke care, polymorphisms associated with functional outcome must be inventoried and described in a granular fashion. Aggregating and summarizing the variants of interests will allow investigators to take the next steps: comparative analysis to determine the weighted influence of each polymorphism, genotype-guided treatment trials, and machine learning for outcome prediction.
Review criteria
A generalized search was conducted in PubMed with the following terms: (stroke OR ischemic stroke) AND (genotype OR genetic variant OR polymorphism) AND (functional outcome). Publications that examined associations between genetic polymorphisms and ischemic stroke functional outcome metrics (see below) were aggregated. Pediatric studies were excluded. Each gene of interest was further investigated in PubMed using the formula, ([gene of interest]) AND (ischemic stroke).
Outcome metrics
Several metrics exist to quantify and evaluate neurological functioning poststroke. Neurologic deterioration (ND) describes clinical worsening based on changes in impairment scores denoted by the Glasgow Coma Scale (GCS) or the NIH Stroke Scale (NIHSS) [212, 243]. Recovery status is commonly examined using the modified Rankin Scale (mRS) and the Barthel Index (BI). mRS output is a discrete value ranging from 0 to 6, assessing a patient’s ability to perform basic tasks such as ambulation, with zero meaning no disability and six indicating death. The original Rankin Scale (RS) was only from 1 to 5. The asymptomatic and death categories were added later. [37] BI tests a patient’s ability to complete various functional tasks and is scored on a scale from 0 to 100; higher scores imply independence [221]. A modified Barthel Index (mBI) was developed to enhance specificity by increasing the number of scoring categories [239] Functional Independence Measure (FIM) is another method of examining functional status. It contains 5 cognitive and 13 motor sections. Each item scored is from 1–7 and low scores indicate increased dependence [173] The Rivermead Motor Assessment (RMA) specifically tests motor function [6] and the Fugl-Meyer Assessment is a quantitative index to assess motor function and some sensation qualities [91].
References
Abdul S, Leebeek FWG, Rijken DC, Uitte de Willige S (2016) Natural heterogeneity of α2-antiplasmin: functional and clinical consequences. Blood. 127(5):538–545. https://doi.org/10.1182/blood-2015-09-670117
Åberg D, Jood K, Blomstrand C, Jern C, Nilsson M, Isgaard J, Aberg ND (2011) Serum IGF-I levels correlate to improvement of functional outcome after ischemic stroke. J Clin Endocrinol Metabol. https://doi.org/10.1210/jc.2010-2802
Aberg ND, Olsson S, Aberg D, Jood K, Stanne TM, Nilsson M, Blomstrand C, Svensson J, Isgaard J, Jern C (2013) Genetic variation at the IGF1 locus shows association with post-stroke outcome and to circulating IGF1. Eur J Endocrinol. 169(6):759–765. https://doi.org/10.1530/EJE-13-0486
Abhinand PA, Manikandan M, Mahalakshmi R, Ragunath PK (2017) Meta-analysis study to evaluate the association of MTHFR C677T polymorphism with risk of ischemic stroke. Bioinformation. 13(6):214–219. https://doi.org/10.6026/97320630013214
Takeo Abumiya, Robert Fitridge, Curt Mazur, Copeland Brian R, Koziol James A, Tschopp Juerg F, Pierschbacher Michael D, del Zoppo Gregory J (2000) Integrin αIIbβ3 inhibitor preserves microvascular patency in experimental acute focal cerebral ischemia. Stroke. 31(6):1402–1410. https://doi.org/10.1161/01.STR.31.6.1402
Adams SA, Ashburn A, Pickering RM, Taylor D (1997) The scalability of the rivermead motor assessment in acute stroke patients. Clin Rehabilit. 11(1):42–51. https://doi.org/10.1177/026921559701100107
Alevizaki M, Synetou M, Xynos K, Pappa T, Vemmos KN (2007) Low triiodothyronine: a strong predictor of outcome in acute stroke patients. Eur J Clin Investig. 37(8):651–657. https://doi.org/10.1111/j.1365-2362.2007.01839.x
Almeida OP, Norman PE, Allcock R, van Bockxmeer F, Hankey GJ, Jamrozik K, Flicker L (2009) Polymorphisms of the CRP gene inhibit inflammatory response and increase susceptibility to depression: the Health in Men Study. Int J Epidemiol. 38(4):1049–1059. https://doi.org/10.1093/ije/dyp199
Ancelin M-L, Farré A, Carrière I, Ritchie K, Chaudieu I, Ryan J (2015) C-reactive protein gene variants: independent association with late-life depression and circulating protein levels. Translat Psychiatry. 5(1):e499–e499. https://doi.org/10.1038/tp.2014.145
Antunes TT, Gagnon A, Langille ML, Sorisky A (2008) Thyroid-stimulating hormone induces interleukin-6 release from human adipocytes through activation of the nuclear factor-kappaB pathway. Endocrinology. 149(6):3062–3066. https://doi.org/10.1210/en.2007-1588
Aratani Y (2018) Myeloperoxidase: Its role for host defense, inflammation, and neutrophil function. Arch Biochem Biophys. 640:47–52. https://doi.org/10.1016/j.abb.2018.01.004
Aref HMA, Fahmy NA, Khalil SH, Ahmed MF, ElSadek A, Abdulghani MO (2020) Role of interleukin-6 in ischemic stroke outcome. Egypt J Neurol Psychiatry Neurosurg. 56(1):12. https://doi.org/10.1186/s41983-019-0121-8
Armbrust M, Worthmann H, Dengler R, Schumacher H, Lichtinghagen R, Eschenfelder CC, Endres M, Ebinger M (2017) Circulating insulin-like growth factor-1 and insulin-like growth factor binding protein-3 predict three-months outcome after ischemic stroke. Experim Clin Endocrinol Diabetes 125(7):485–491. https://doi.org/10.1055/s-0043-103965
Arroja MMC, Reid E, McCabe C (2016) Therapeutic potential of the renin angiotensin system in ischaemic stroke. Experim Translat Stroke Med. 8(1):8. https://doi.org/10.1186/s13231-016-0022-1
Asare Y et al (2020) Histone deacetylase 9 activates IKK to regulate atherosclerotic plaque vulnerability. Circul Res. 127(6):811–823. https://doi.org/10.1161/CIRCRESAHA.120.316743
Ashar FN, Zhang Y, Longchamps RJ, Lane J, Moes A, Grove ML, Mychaleckyj JC, Taylor KD, Coresh J, Rotter JI, Boerwinkle E, Pankratz N, Guallar E, Arking DE (2017) Association of mitochondrial DNA copy number with cardiovascular disease. JAMA Cardiol. 2(11):1247–1255. https://doi.org/10.1001/jamacardio.2017.3683
Azghandi S, Prell C, van der Laan SW, Schneider M, Malik R, Berer K, Gerdes N, Pasterkamp G, Weber C, Haffner C, Dichgans M (2015) Deficiency of the stroke relevant HDAC9 gene attenuates atherosclerosis in accord with allele-specific effects at 7p21.1. Stroke. 46(1):197–202. https://doi.org/10.1161/STROKEAHA.114.007213
Balkaya M, Cho S (2019) Genetics of stroke recovery: BDNF val66met polymorphism in stroke recovery and its interaction with aging. Neurobiol Dis. 126:36–46. https://doi.org/10.1016/j.nbd.2018.08.009
Bathina S, Das UN (2015) Brain-derived neurotrophic factor and its clinical implications. Arch Med Sci AMS. 11(6):1164–1178. https://doi.org/10.5114/aoms.2015.56342
Belinky F, Nativ N, Stelzer G, Zimmerman S, Iny Stein T, Safran M, Lancet D (2015) PathCards: multi-source consolidation of human biological pathways. Database J Biol Databases Curat. https://doi.org/10.1093/database/bav006
Bernal J, Guadaño-Ferraz A, Morte B (2015) Thyroid hormone transporters–functions and clinical implications. Nat Rev Endocrinol. 11(7):406–417. https://doi.org/10.1038/nrendo.2015.66
Bevan S, Traylor M, Adib-Samii P, Malik R, Paul NLM, Jackson C, Farrall M, Rothwell PM, Sudlow C, Dichgans M, Markus HS (2012) Genetic heritability of ischemic stroke and the contribution of previously reported candidate gene and genomewide associations. Stroke. 43(12):3161–3167. https://doi.org/10.1161/STROKEAHA.112.665760
Bian J, Sun Y (1997) Transcriptional activation by p53 of the human type IV collagenase (gelatinase A or matrix metalloproteinase 2) promoter. Mol Cell Biol. 17(11):6330–6338
de Bilbao F, Arsenijevic D, Moll T, Garcia-Gabay I, Vallet P, Langhans W, Giannakopoulos P (2009) In vivo over-expression of interleukin-10 increases resistance to focal brain ischemia in mice. J Neurochem. 110(1):12–22. https://doi.org/10.1111/j.1471-4159.2009.06098.x
Biscetti F, Straface G, Giovannini S, Santoliquido A, Angelini F, Santoro L, Porreca CF, Pecorini G, Ghirlanda G, Flex A (2013) Association between TNFRSF11B gene polymorphisms and history of ischemic stroke in Italian diabetic patients. Hum Genet. 132(1):49–55. https://doi.org/10.1007/s00439-012-1224-9
Bodhankar S, Chen Y, Vandenbark AA, Murphy SJ, Offner H (2014) Treatment of experimental stroke with IL-10-producing B-cells reduces infarct size and peripheral and CNS inflammation in wild-type B-cell-sufficient mice. Metab Brain Dis. 29(1):59–73. https://doi.org/10.1007/s11011-013-9474-3
Bond GL et al (2004) A single nucleotide polymorphism in the MDM2 promoter attenuates the p53 tumor suppressor pathway and accelerates tumor formation in humans. Cell. 119(5):591–602. https://doi.org/10.1016/j.cell.2004.11.022
Bouffi C, Bony C, Courties G, Jorgensen C, Noël D (2010) IL-6-dependent PGE2 secretion by mesenchymal stem cells inhibits local inflammation in experimental arthritis. PLOS One. 5(12):e14247. https://doi.org/10.1371/journal.pone.0014247
Bouziana S, Tziomalos K, Goulas A, Vyzantiadis T-A, Papadopoulou M, Panderi A, Ηatzitolios AΙ (2019) Effects of major adipokines and the -420 C > G resistin gene polymorphism on the long-term outcome of patients with acute ischemic stroke. Int J Neurosci. 129(10):978–985. https://doi.org/10.1080/00207454.2019.1596906
Bouziana SD, Tziomalos K, Goulas A, Vyzantiadis T-A, Panderi A, Ηatzitolios AΙ (2018) Major adipokines and the -420C>G resistin gene polymorphism as predictors of acute ischemic stroke severity and in-hospital outcome. J Stroke Cerebrovasc Dis 27(4):963–970. https://doi.org/10.1016/j.jstrokecerebrovasdis.2017.10.038
Bowman CC, Rasley A, Tranguch SL, Marriott I (2003) Cultured astrocytes express toll-like receptors for bacterial products. Glia. 43(3):281–291. https://doi.org/10.1002/glia.10256
Brand MD, Esteves TC (2005) Physiological functions of the mitochondrial uncoupling proteins UCP2 and UCP3. Cell Metabol. 2(2):85–93. https://doi.org/10.1016/j.cmet.2005.06.002
Braun RG, Kittner SJ, Ryan KA, Cole JW (2020) Effects of the BDNF Val66Met polymorphism on functional status and disability in young stroke patients. PLoS One. 15:12. https://doi.org/10.1371/journal.pone.0237033
Brea D, Blanco M, Ramos-Cabrer P, Moldes O, Arias S, Pérez-Mato M, Leira R, Sobrino T, Castillo J (2011) Toll-like receptors 2 and 4 in ischemic stroke: outcome and therapeutic values. J Cereb Blood Flow Metabol. 31(6):1424–1431. https://doi.org/10.1038/jcbfm.2010.231
Bridge KI, Macrae F, Bailey MA, Johnson A, Philippou H, Scott DJA, Ariens RAS (2014) The alpha-2-antiplasmin Arg407Lys polymorphism is associated with abdominal aortic aneurysm. Thromb Res. 134(3):723–728. https://doi.org/10.1016/j.thromres.2014.06.019
Broderick J, Lu M, Jackson C, Pancioli A, Tilley BC, Fagan SC, Kothari R, Levine SR, Marler JR, Lyden PD, Haley EC, Brott T, Grotta JC, NINDS t-PA Stroke Study Group (2001) Apolipoprotein E phenotype and the efficacy of intravenous tissue plasminogen activator in acute ischemic stroke. Annals Neurol. 49(6):736–744. https://doi.org/10.1002/ana.1058
Broderick Joseph P, Opeolu Adeoye, Jordan Elm (2017) Evolution of the modified rankin scale and its use in future stroke trials. Stroke. 48(7):2007–2012
Brosnan JT, Brosnan ME (2006) The sulfur-containing amino acids: an overview. J Nutrit 136(6):1636S-1640S. https://doi.org/10.1093/jn/136.6.1636S
Brouwers HB, Biffi A, Ayres AM, Schwab K, Cortellini L, Romero JM, Rost NS, Viswanathan A, Greenberg SM, Rosand J, Goldstein JN (2012) Apolipoprotein E genotype predicts hematoma expansion in lobar intracerebral hemorrhage. Stroke. 43(6):1490–1495. https://doi.org/10.1161/STROKEAHA.111.643262
Bucay N, Sarosi I, Dunstan CR, Morony S, Tarpley J, Capparelli C, Scully S, Tan HL, Xu W, Lacey DL, Boyle WJ, Simonet WS (1998) osteoprotegerin-deficient mice develop early onset osteoporosis and arterial calcification. Genes Develop. 12(9):1260–1268. https://doi.org/10.1101/gad.12.9.1260
Burd CE, Jeck WR, Liu Y, Sanoff HK, Wang Z, Sharpless NE (2010) Expression of Linear and Novel Circular Forms of an INK4/ARF-Associated Non-Coding RNA Correlates with Atherosclerosis Risk. PLoS Genet. 6(12):e1001233. https://doi.org/10.1371/journal.pgen.1001233
Bustamante A et al (2014) Prognostic value of blood interleukin-6 in the prediction of functional outcome after stroke: a systematic review and meta-analysis. J Neuroimmunol. 274(1–2):215–224. https://doi.org/10.1016/j.jneuroim.2014.07.015
Cai B et al (2015) Mitochondrial DNA haplogroups and short-term neurological outcomes of ischemic stroke. Scient Rep. 5:9864. https://doi.org/10.1038/srep09864
Calabrese V, Mancuso C, Calvani M, Rizzarelli E, Butterfield DA, Giuffrida Stella AM (2007) Nitric oxide in the central nervous system: neuroprotection versus neurotoxicity. Nat Rev Neurosci. 8(10):766–775. https://doi.org/10.1038/nrn2214
Cao Q, Rong S, Repa JJ, Clair R. St., Parks JS, Mishra N (2014) HDAC9 represses cholesterol efflux and generation of alternatively activated macrophages in atherosclerosis development. Arterioscler Thromb Vasc Biol. 34(9):1871–1879. https://doi.org/10.1161/ATVBAHA.114.303393
Cao Y, Cui C, Zhao H, Pan X, Li W, Wang K, Ma A (2019) Plasma Osteoprotegerin correlates with stroke severity and the occurrence of microembolic signals in patients with acute ischemic stroke. Dis Mark. https://doi.org/10.1155/2019/3090364
Carter Angela M, Catto Andrew J, Bamford John M, Grant Peter J (1999) Association of the platelet glycoprotein IIb HPA-3 polymorphism with survival after acute ischemic stroke. Stroke. 30(12):2606–2611. https://doi.org/10.1161/01.STR.30.12.2606
Casas AI, Geuss E, Kleikers PWM, Mencl S, Herrmann AM, Buendia I, Egea J, Meuth SG, Lopez MG, Kleinschnitz C, Schmidt HHHW (2017) NOX4-dependent neuronal autotoxicity and BBB breakdown explain the superior sensitivity of the brain to ischemic damage. Proc Natl Acad Sci. 114(46):12315–12320. https://doi.org/10.1073/pnas.1705034114
Caso JR, Pradillo JM, Hurtado O, Lorenzo P, Moro MA, Lizasoain I (2007) Toll-like receptor 4 is involved in brain damage and inflammation after experimental stroke. Circulation. 115(12):1599–1608. https://doi.org/10.1161/CIRCULATIONAHA.106.603431
Chakraborty B, Chowdhury D, Vishnoi G, Goswami B, Kishore J, Agarwal S (2013) Interleukin-6 gene -174 G/C promoter polymorphism predicts severity and outcome in acute ischemic stroke patients from north India. J Stroke Cerebrovasc Dis. 22(5):683–689. https://doi.org/10.1016/j.jstrokecerebrovasdis.2012.02.007
Chang L-T, Yuen C-M, Liou C-W, Lu C-H, Chang W-N, Youssef AA, Yip H-K (2010) Link between interleukin-10 level and outcome after ischemic stroke. Neuroimmunomodulation. 17(4):223–228. https://doi.org/10.1159/000290038
Chang WH, Park E, Lee J, Lee A, Kim Y-H (2017) Association between brain-derived neurotrophic factor genotype and upper extremity motor outcome after stroke. Stroke. 48(6):1457–1462. https://doi.org/10.1161/STROKEAHA.116.015264
Chen A-N, Zhong L-L, Ju K-J, Cao H (2021) Bioinformatics analysis of a functional ANGPT1 variant that interferes with miR-607 and its association with susceptibility and outcome of ischemic stroke in a han population. Ther Clin Risk Manag 17(2021):1045–1052. https://doi.org/10.2147/TCRM.S328964
Chen J, Yang T, Yu H, Sun K, Shi Y, Song W, Bai Y, Wang X, Lou K, Song Y, Zhang Y, Hui R (2010) A functional variant in the 3’-UTR of angiopoietin-1 might reduce stroke risk by interfering with the binding efficiency of microRNA 211. Hum Mol Genet. 19(12):2524–2533. https://doi.org/10.1093/hmg/ddq131
Chen S, Wang M, Yang H, Mao L, He Q, Jin H, Ye Z-M, Luo X-Y, Xia Y-P, Hu B (2017) LncRNA TUG1 sponges microRNA-9 to promote neurons apoptosis by up-regulated Bcl2l11 under ischemia. Biochem Biophys Res Commun. 485(1):167–173. https://doi.org/10.1016/j.bbrc.2017.02.043
Chen X-J, Qiu C-G, Kong X-D, Ren S-M, Dong J-Z, Gu H-P, Chen Y-W, Tao H-L, Sarbesh J (2018) The association between an endothelial nitric oxide synthase gene polymorphism and coronary heart disease in young people and the underlying mechanism. Mol Med Reports. 17(3):3928–3934. https://doi.org/10.3892/mmr.2017.8314
Chitravas N, Dewey HM, Nicol MB, Harding DL, Pearce DC, Thrift AG (2007) Is prestroke use of angiotensin-converting enzyme inhibitors associated with better outcome? Neurology. 68(20):1687–1693. https://doi.org/10.1212/01.wnl.0000261914.18101.60
Cho YM, Youn B-S, Chung SS, Kim KW, Lee HK, Yu K-Y, Park HJ, Shin HD, Park KS (2004) Common genetic polymorphisms in the promoter of resistin gene are major determinants of plasma resistin concentrations in humans. Diabetologia. 47(3):559–565. https://doi.org/10.1007/s00125-003-1319-x
Chong MR, Narula S, Morton R, Judge C, Akhabir L, Cawte N, Pathan N, Lali R, Mohammadi-Shemirani P, Shoamanesh A, O’Donnell M, Yusuf S, Langhorne P, Pare G (2021) Mitochondrial DNA copy number as a marker and mediator of stroke prognosis: observational and mendelian randomization analyses. Neurology. https://doi.org/10.1212/WNL.0000000000013165
Chrousos GP (1995) The hypothalamic-pituitary-adrenal axis and immune-mediated inflammation. N Engl J Med. 332(20):1351–1362. https://doi.org/10.1056/NEJM199505183322008
Cojocaru IM, Cojocaru M, Iliescu I, Botnaru L, Gurban CV, Sfrijan F, Tănăsescu R (2010) Plasma myeloperoxidase levels in patients with acute ischemic stroke. Romanian J Intern Med Revue Roumaine De Medecine Interne. 48(1):101–104
Cole JW et al (2021) The copy number variation and stroke (CaNVAS) risk and outcome study. PLOS One. 16(4):e0248791. https://doi.org/10.1371/journal.pone.0248791
Colhoun HM, McKeigue PM, Smith GD (2003) Problems of reporting genetic associations with complex outcomes. The Lancet. 361(9360):865–872. https://doi.org/10.1016/S0140-6736(03)12715-8
Corder EH, Saunders AM, Risch NJ, Strittmatter WJ, Schmechel DE, Gaskell PC, Rimmler JB, Locke PA, Conneally PM, Schmader KE (1994) Protective effect of apolipoprotein E type 2 allele for late onset Alzheimer disease. Nat Genet. 7(2):180–184. https://doi.org/10.1038/ng0694-180
Cosarderelioglu C, Nidadavolu LS, George CJ, Oh ES, Bennett DA, Walston JD, Abadir PM (2020) Brain renin-angiotensin system at the intersect of physical and cognitive frailty. Front Neurosci. https://doi.org/10.3389/fnins.2020.586314
Cramer SC, Procaccio V, GAIN Americas, and GAIN International Study Investigators (2012) Correlation between genetic polymorphisms and stroke recovery: analysis of the GAIN Americas and GAIN International Studies. Eur J Neurol. 19(5):718–724. https://doi.org/10.1111/j.1468-1331.2011.03615.x
Danesh J, Wheeler JG, Hirschfield GM, Eda S, Eiriksdottir G, Rumley A, Lowe GDO, Pepys MB, Gudnason V (2004) C-reactive protein and other circulating markers of inflammation in the prediction of coronary heart disease. N Engl J Med. 350(14):1387–1397. https://doi.org/10.1056/NEJMoa032804
Danis VA, Millington M, Hyland VJ, Grennan D (1995) Cytokine production by normal human monocytes: inter-subject variation and relationship to an IL-1 receptor antagonist (IL-1Ra) gene polymorphism. Clin Experim Immunol. 99(2):303–310. https://doi.org/10.1111/j.1365-2249.1995.tb05549.x
Davis CM, Liu X, Alkayed NJ (2017) Cytochrome P450 eicosanoids in cerebrovascular function and disease. Pharmacol Therapeut. 179:31–46. https://doi.org/10.1016/j.pharmthera.2017.05.004
De Smedt A, Brouns R, Uyttenboogaart M, De Raedt S, Moens M, Wilczak N, Luijckx G-J, De Keyser J (2011) Insulin-like growth factor I serum levels influence ischemic stroke outcome. Stroke. 42(8):2180–2185. https://doi.org/10.1161/STROKEAHA.110.600783
Deinhardt K, Chao MV (2014) Shaping neurons: long and short range effects of mature and proBDNF signalling upon neuronal structure. Neuropharmacology. https://doi.org/10.1016/j.neuropharm.2013.04.054
Dennis EA, Norris PC (2015) Eicosanoid storm in infection and inflammation. Nat Rev Immunol. 15(8):511–523. https://doi.org/10.1038/nri3859
van der Deure WM, Hansen PS, Peeters RP, Kyvik KO, Friesema ECH, Hegedüs L, Visser TJ (2008) Thyroid hormone transport and metabolism by organic anion transporter 1C1 and consequences of genetic variation. Endocrinology. 149(10):5307–5314. https://doi.org/10.1210/en.2008-0430
Dhital R, Poudel DR, Tachamo N, Gyawali B, Basnet S, Shrestha P, Karmacharya P (2017) Ischemic stroke and impact of thyroid profile at presentation: a systematic review and meta-analysis of observational studies. J Stroke Cerebrovasc Dis. 26(12):2926–2934. https://doi.org/10.1016/j.jstrokecerebrovasdis.2017.07.015
Dianov GL, Hübscher U (2013) Mammalian base excision repair: the forgotten archangel. Nucleic Acids Res. 41(6):3483–3490. https://doi.org/10.1093/nar/gkt076
Díaz-Maroto Cicuéndez I, Fernández-Díaz E, García-García J, Jordán J, Fernández-Cadenas I, Montaner J, Serrano-Heras G, Segura T (2017) The UCP2–866G/a polymorphism could be considered as a genetic marker of different functional prognosis in ischemic stroke after recanalization. Neuromol Med. 19:571–578. https://doi.org/10.1007/s12017-017-8470-x
Dong X, Wang J, Wang G, Wang J, Wang L, Du Y (2021) MTHFR A1298C gene polymorphism on stroke risk: an updated meta-analysis. Genes Environm. 43:40. https://doi.org/10.1186/s41021-021-00208-z
Dong Z, Deng L, Peng Q, Pan J, Wang Y (2020) CircRNA expression profiles and function prediction in peripheral blood mononuclear cells of patients with acute ischemic stroke. J Cell Physiol. 235(3):2609–2618. https://doi.org/10.1002/jcp.29165
Donkor ES (2018) Stroke in the 21st century: a snapshot of the burden, epidemiology, and quality of life. Stroke Res Treat. https://doi.org/10.1155/2018/3238165
Drago A, De Ronchi D, Serretti A (2007) Incomplete coverage of candidate genes: a poorly considered bias. Curr Genom. 8(7):476–483. https://doi.org/10.2174/138920207783591681
Dubey RK, Gillespie DG, Jackson EK (1999) Adenosine inhibits collagen and total protein synthesis in vascular smooth muscle cells. Hypertension. 33(1):190–194. https://doi.org/10.1161/01.HYP.33.1.190
Efstathiou SP, Tsiakou AG, Tsioulos DI, Panagiotou TN, Pefanis AV, Achimastos AD, Mountokalakis TD (2007) Prognostic significance of plasma resistin levels in patients with atherothrombotic ischemic stroke. Clinica Chimica Acta Int J Clin Chem. 378(1–2):78–85. https://doi.org/10.1016/j.cca.2006.10.023
Ellul J, Markoula S, Marousi S, Galidi A, Kyritsis AP, Papathanasopoulos P, Georgiou I (2011) Association of endothelial nitric oxide synthase polymorphism G894T with functional outcome in acute stroke patients. Neurol Res. 33(8):835–840. https://doi.org/10.1179/1743132811Y.0000000011
Erta M, Quintana A, Hidalgo J (2012) Interleukin-6, a major cytokine in the central nervous system. Int J Biol Sci. 8(9):1254–1266. https://doi.org/10.7150/ijbs.4679
Essa H, Vasant DH, Raginis-Zborowska A, Payton A, Michou E, Hamdy S (2017) The BDNF polymorphism Val66Met may be predictive of swallowing improvement post pharyngeal electrical stimulation in dysphagic stroke patients. Neurogastroenterol Motility. https://doi.org/10.1111/nmo.13062
Esterbauer H, Schneitler C, Oberkofler H, Ebenbichler C, Paulweber B, Sandhofer F, Ladurner G, Hell E, Strosberg AD, Patsch JR, Krempler F, Patsch W (2001) A common polymorphism in the promoter of UCP2 is associated with decreased risk of obesity in middle-aged humans. Nat Genet. 28(2):178–183. https://doi.org/10.1038/88911
van Exel E, Gussekloo J, de Craen AJM, Bootsma-van der Wiel A, Frölich M, Westendorp RGJ (2002) Inflammation and stroke: the Leiden 85-Plus Study. Stroke. 33(4):1135–1138. https://doi.org/10.1161/01.str.0000014206.05597.9e
Farah C, Michel LYM, Balligand J-L (2018) Nitric oxide signalling in cardiovascular health and disease. Nat Rev Cardiol. 15(5):292–316. https://doi.org/10.1038/nrcardio.2017.224
Feigin VL et al (2019) Global, regional, and national burden of neurological disorders, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. The Lancet Neurol. 18(5):459–480. https://doi.org/10.1016/S1474-4422(18)30499-X
Förstermann U, Sessa WC (2012) Nitric oxide synthases: regulation and function. Eur Heart J. https://doi.org/10.1093/eurheartj/ehr304
Fugl-Meyer AR, Jääskö L, Leyman I, Olsson S, Steglind S (1975) The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scandinavian J Rehabilit Med. 7(1):13–31
Fujita T, Tozaki-Saitoh H, Inoue K (2009) P2Y1 receptor signaling enhances neuroprotection by astrocytes against oxidative stress via IL-6 release in hippocampal cultures. Glia. 57(3):244–257. https://doi.org/10.1002/glia.20749
Ganz P, Amarenco P, Goldstein LB, Sillesen H, Bao W, Preston GM, Welch KMA, Steering Committee SPARCL (2017) Association of osteopontin, neopterin, and myeloperoxidase with stroke risk in patients with prior stroke or transient ischemic attacks: results of an analysis of 13 biomarkers from the stroke prevention by aggressive reduction in cholesterol levels trial. Stroke. 48(12):3223–3231. https://doi.org/10.1161/STROKEAHA.117.017965
Garcia JM, Stillings SA, Leclerc JL, Phillips H, Edwards NJ, Robicsek SA, Hoh BL, Blackburn S, Doré S (2017) Role of interleukin-10 in acute brain injuries. Front Neurol. 8:244. https://doi.org/10.3389/fneur.2017.00244
Gerthoffer WT (2007) Mechanisms of vascular smooth muscle cell migration. Circul Res. 100(5):607–621. https://doi.org/10.1161/01.RES.0000258492.96097.47
Gertz K et al (2012) Essential role of interleukin-6 in post-stroke angiogenesis. Brain 135(Pt 6):1964–1980. https://doi.org/10.1093/brain/aws075
Glubb DM et al (2011) Novel functional germline variants in the vascular endothelial growth factor receptor 2 gene and their effect on gene expression and microvessel density in lung cancer. Clin Cancer Res. 17(16):5257–5267. https://doi.org/10.1158/1078-0432.CCR-11-0379
Golledge J, Clancy P, Maguire J, Lincz L, Koblar S, McEvoy M, Attia J, Levi C, Sturm J, Almeida OP, Yeap BB, Flicker L, Norman PE, Hankey GJ (2014) Plasma angiopoietin-1 is lower after ischemic stroke and associated with major disability but not stroke incidence. Stroke. 45(4):1064–1068. https://doi.org/10.1161/STROKEAHA.113.004339
Gomez-Sanchez JC, Delgado-Esteban M, Rodriguez-Hernandez I, Sobrino T, Perez de la Ossa N, Reverte S, Bolaños JP, Gonzalez-Sarmiento R, Castillo J, Almeida A (2011) The human Tp53 Arg72Pro polymorphism explains different functional prognosis in stroke. J Experim Med. 208(3):429–437. https://doi.org/10.1084/jem.20101523
Gower A, Tiberi M (2018) The intersection of central dopamine system and stroke: potential avenues aiming at enhancement of motor recovery. Front Synaptic Neurosci. 10:18. https://doi.org/10.3389/fnsyn.2018.00018
Greenberg DA, Jin K (2013) Vascular endothelial growth factors (VEGFs) and stroke. Cell Mol Life Sci CMLS. 70(10):1753–1761. https://doi.org/10.1007/s00018-013-1282-8
Greisenegger S, Endler G, Haering D, Schillinger M, Lang W, Lalouschek W, Mannhalter C (2003) The (-174) G/C polymorphism in the interleukin-6 gene is associated with the severity of acute cerebrovascular events. Thromb Res. 110(4):181–186. https://doi.org/10.1016/s0049-3848(03)00376-1
Gretarsdottir S et al (2003) The gene encoding phosphodiesterase 4D confers risk of ischemic stroke. Nat Genet. 35(2):131–138. https://doi.org/10.1038/ng1245
Gromadzka G, Baranska-Gieruszczak M, Sarzynska-Dlugosz I, Ciesielska A, Czlonkowska A (2007) The APOE polymorphism and 1-year outcome in ischemic stroke: genotype-gender interaction. Acta Neurologica Scandinavica. 116(6):392–398. https://doi.org/10.1111/j.1600-0404.2007.00880.x
Gromadzka G, Sarzynska-Dlugosz I, Czlonkowska A (2007) IL1RN intron 2 polymorphism caused by variable number tandem repeats is associated with 1-year outcome in patients with ischaemic stroke. J Neurol Neurosurg Psychiatry. 78(2):183–186. https://doi.org/10.1136/jnnp.2006.093104
Grond-Ginsbach C, Erhart P, Chen B, Kloss M, Engelter ST, Cole JW (2018) Copy number variation and risk of stroke. Stroke. 49(10):2549–2554. https://doi.org/10.1161/STROKEAHA.118.020371
Gu Z, Kaul M, Yan B, Kridel SJ, Cui J, Strongin A, Smith JW, Liddington RC, Lipton SA (2002) S-nitrosylation of matrix metalloproteinases: signaling pathway to neuronal cell death. Science 297(5584):1186–1190. https://doi.org/10.1126/science.1073634
Guo J, Yu L, Zhang J, Chen N, Zhou M, He L (2014) CRP gene polymorphism predicts post-stroke functional outcome in Han Chinese. Acta Neurologica Scandinavica. 129(4):263–268. https://doi.org/10.1111/ane.12180
Guo X, Dai X, Zhou T, Wang H, Ni J, Xue J, Wang X (2020) Mosaic loss of human Y chromosome: what, how and why. Hum Genet. 139(4):421–446. https://doi.org/10.1007/s00439-020-02114-w
Haberland M, Montgomery RL, Olson EN (2009) The many roles of histone deacetylases in development and physiology: implications for disease and therapy. Nat Rev Genet. 10(1):32–42. https://doi.org/10.1038/nrg2485
Han Y, Sun W, Wang L, Tao S, Tian L, Hao Y, Zhang W, Wu S, Li S, Lv H, Zheng SL, Sun J, Xu J (2013) HDAC9 gene is associated with stroke risk in a Chinese population. Experim Biol Med. 238(7):842–847. https://doi.org/10.1177/1535370213494650
Han Z, Qi L, Xu Q, Xu M, Cai L, Wong J, Hu X, Luo X, Wang J, Zhang Y, Li Y, Wang QM (2020) BDNF Met allele is associated with lower cognitive function in poststroke rehabilitation. Neurorehabilit Neural Repair. 34(3):247–259. https://doi.org/10.1177/1545968320902127
Hansen TM, Moss AJ, Brindle NPJ (2008) Vascular endothelial growth factor and angiopoietins in neurovascular regeneration and protection following stroke. Curr Neurovasc Res. 5(4):236–245. https://doi.org/10.2174/156720208786413433
Hartung JE, Ciszek BP, Nackley AG (2014) β2- and β3-adrenergic receptors drive COMT-dependent pain by increasing production of nitric oxide and cytokines. Pain. 155(7):1346–1355. https://doi.org/10.1016/j.pain.2014.04.011
Hasbi A, Fan T, Alijaniaram M, Nguyen T, Perreault ML, O’Dowd BF, George SR (2009) Calcium signaling cascade links dopamine D1–D2 receptor heteromer to striatal BDNF production and neuronal growth. Proc Natl Acad Sci USA. 106(50):21377–21382. https://doi.org/10.1073/pnas.0903676106
Hassan Y, Al-Jabi SW, Aziz NA, Looi I, Zyoud SH (2011) Effect of prestroke use of angiotensin-converting enzyme inhibitors alone versus combination with antiplatelets and statin on ischemic stroke outcome. Clin Neuropharmacol. 34(6):234–240. https://doi.org/10.1097/WNF.0b013e3182348abe
He W, Huang P, Liu D, Zhong L, Yu R, Li J (2016) Polymorphism of the XRCC1 gene is associated with susceptibility and short-term recovery of ischemic stroke. Int J Environm Res Public Health. 13(10):E1016. https://doi.org/10.3390/ijerph13101016
He W, Lu M, Li G, Sun Z, Liu D, Gu L (2017) Methylene Tetrahydrofolate Reductase (MTHFR) rs868014 Polymorphism Regulated by miR-1203 Associates with Risk and Short Term Outcome of Ischemic Stroke. Cell Physiol Biochem. 41(2):701–710. https://doi.org/10.1159/000458429
He W, Wang Q, Gu L, Zhong L, Liu D (2018) NOX4 rs11018628 polymorphism associates with a decreased risk and better short-term recovery of ischemic stroke. Experim Therapeut Med. 16(6):5258–5264. https://doi.org/10.3892/etm.2018.6874
Heart Outcomes Prevention Evaluation Study Investigators, Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais G (2000) Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. N Engl J Med. 342(3):145–153. https://doi.org/10.1056/NEJM200001203420301
Heinrich PC, Castell JV, Andus T (1990) Interleukin-6 and the acute phase response. Biochem J. 265(3):621–636
Helm EE, Tyrell CM, Pohlig RT, Brady LD, Reisman DS (2016) The presence of a single-nucleotide polymorphism in the BDNF gene affects the rate of locomotor adaptation after stroke. Experim Brain Res. 234(2):341–351. https://doi.org/10.1007/s00221-015-4465-8
Hong C-J, Liou Y-J, Tsai S-J (2011) Effects of BDNF polymorphisms on brain function and behavior in health and disease. Brain Res Bull. 86(5–6):287–297. https://doi.org/10.1016/j.brainresbull.2011.08.019
Hong L-Z, Zhao X-Y, Zhang H-L (2010) p53-mediated neuronal cell death in ischemic brain injury. Neurosci Bull. 26(3):232–240. https://doi.org/10.1007/s12264-010-1111-0
Hoy A, Leininger-Muller B, Poirier O, Siest G, Gautier M, Elbaz A, Amarenco P, Visvikis S (2003) Myeloperoxidase polymorphisms in brain infarction. Association with infarct size and functional outcome. Atherosclerosis. 167(2):223–230. https://doi.org/10.1016/s0021-9150(02)00041-2
Hu Y, Zheng Y, Wu Y, Ni B, Shi S (2014) Imbalance between IL-17A-producing cells and regulatory T cells during ischemic stroke. Mediators Inflamm 2014(2014):813045. https://doi.org/10.1155/2014/813045
Hu Z, Lai J, Chen L, Yi Y, Li R, Liao W (2020) Can baseline C-reactive protein level predict functional outcome in acute ischaemic stroke? A meta-analysis. Biomarkers. 25(7):525–532. https://doi.org/10.1080/1354750X.2020.1817982
Huang H, Al-Shabrawey M, Wang M-H (2016) Cyclooxygenase- and cytochrome P450-derived eicosanoids in stroke. Prostagland Lipid Mediat. 122:45–53. https://doi.org/10.1016/j.prostaglandins.2015.12.007
Huang J et al (2019) Platelet integrin αIIbβ3: signal transduction, regulation, and its therapeutic targeting. J Hematol Oncol. 12(1):26. https://doi.org/10.1186/s13045-019-0709-6
Huang X, Ye Q, Zhu Z, Chen W, Chen Y, Li J, Sun J, Ye Z (2020) Association between a functional interleukin 6 receptor genetic variant and the risk and functional outcome of large artery atherosclerotic stroke. Int J Neurosci. 130(4):355–362. https://doi.org/10.1080/00207454.2019.1688810
Indolfi C, Avvedimento EV, Di Lorenzo E, Esposito G, Rapacciuolo A, Giuliano P, Grieco D, Cavuto L, Stingone AM, Ciullo I, Condorelli G, Chiariello M (1997) Activation of cAMP-PKA signaling in vivo inhibits smooth muscle cell proliferation induced by vascular injury. Nat Med. 3(7):775–779. https://doi.org/10.1038/nm0797-775
Jensen JK, Ueland T, Atar D, Gullestad L, Mickley H, Aukrust P, Januzzi JL (2010) Osteoprotegerin concentrations and prognosis in acute ischaemic stroke. J Intern Med. 267(4):410–417. https://doi.org/10.1111/j.1365-2796.2009.02163.x
Jiang X, Xing H, Wu J, Du R, Liu H, Chen J, Wang J, Wang C, Wu Y (2017) Prognostic value of thyroid hormones in acute ischemic stroke – a meta analysis. Scient Rep. 7:16256. https://doi.org/10.1038/s41598-017-16564-2
Jin Y-C, Lee H, Kim S-W, Kim I-D, Lee H-K, Lee Y, Han P-L, Lee J-K (2016) Intranasal delivery of RGD motif-containing osteopontin icosamer confers neuroprotection in the postischemic brain via αvβ3 integrin binding. Mol Neurobiol. 53(8):5652–5663. https://doi.org/10.1007/s12035-015-9480-z
Jing M, Li B, Hou X, Shoba J, Li C, Liang H, Zhang X, Liu E, Yang B, Meng X (2013) OPN gene polymorphism and the serum OPN levels confer the susceptibility and prognosis of ischemic stroke in Chinese patients. Cell Physiol Biochem 32(6):1798–1807. https://doi.org/10.1159/000356613
Jo S, Kalló I, Bardóczi Z et al (2012) Neuronal hypoxia induces Hsp40-mediated nuclear import of type 3 deiodinase as an adaptive mechanism to reduce cellular metabolism. J Neurosci. 32(25):8491–8500. https://doi.org/10.1523/JNEUROSCI.6514-11.2012
Johansson M, Pedersen A, Cole JW, Lagging C, Lindgren A, Maguire JM, Rost NS, Söderholm M, Worrall BB, Stanne TM, Jern C (2021) Genetic predisposition to mosaic chromosomal loss is associated with functional outcome after ischemic stroke. Neurol Genet 7(6):e634. https://doi.org/10.1212/NXG.0000000000000634
Junnila RK, List EO, Berryman DE, Murrey JW, Kopchick JJ (2013) The GH/IGF-1 axis in ageing and longevity. Nat Rev Endocrinol. 9(6):366–376. https://doi.org/10.1038/nrendo.2013.67
Karantali E, Kazis D, Papavasileiou V, Prevezianou A, Chatzikonstantinou S, Petridis F, McKenna J, Luca A-C, Trus C, Ciobica A, Mavroudis I (2021) Serum BDNF levels in acute stroke: a systematic review and meta-analysis. Medicina. https://doi.org/10.3390/medicina57030297
Kawai T, Akira S (2010) The role of pattern-recognition receptors in innate immunity: update on Toll-like receptors. Nat Immunol. 11(5):373–384. https://doi.org/10.1038/ni.1863
Keshavarz P, Saberi A, Sharafshah A, Asgari K, Rezaei S (2016) Association of BDNF G196A gene polymorphism with ischemic stroke occurrence and its 6-month outcome in an Iranian population. Topics Stroke Rehabilit. 23(4):254–260. https://doi.org/10.1080/10749357.2016.1141491
Kettunen T, Eklund C, Kähönen M, Jula A, Päivä H, Lyytikäinen L-P, Hurme M, Lehtimäki T (2011) Polymorphism in the C-reactive protein (CRP) gene affects CRP levels in plasma and one early marker of atherosclerosis in men: The Health 2000 Survey. Scandinavian J Clin Labor Investig. 71(5):353–361. https://doi.org/10.3109/00365513.2011.568123
Khan TA et al (2013) Apolipoprotein E genotype, cardiovascular biomarkers and risk of stroke: systematic review and meta-analysis of 14 015 stroke cases and pooled analysis of primary biomarker data from up to 60 883 individuals. Int J Epidemiol. 42(2):475–492. https://doi.org/10.1093/ije/dyt034
Kim B-R, Kim HY, Chun YI, Yun Y-M, Kim H, Choi D-H, Lee J (2016) Association between genetic variation in the dopamine system and motor recovery after stroke. Restorat Neurol Neurosci. 34(6):925–934. https://doi.org/10.3233/RNN-160667
Kim DY, Quinlan EB, Gramer R, Cramer SC (2016) BDNF Val66Met polymorphism is related to motor system function after stroke. Phys Ther. 96(4):533–539. https://doi.org/10.2522/ptj.20150135
Kim HJ, Wei Y, Wojtkiewicz GR, Lee JY, Moskowitz MA, Chen JW (2019) Reducing myeloperoxidase activity decreases inflammation and increases cellular protection in ischemic stroke. J Cereb Blood Flow Metab. 39(9):1864–1877. https://doi.org/10.1177/0271678X18771978
Kim OJ, Hong SH, Oh SH, Kim TG, Min KT, Oh D, Kim NK (2011) Association between VEGF polymorphisms and homocysteine levels in patients with ischemic stroke and silent brain infarction. Stroke. 42(9):2393–2402. https://doi.org/10.1161/STROKEAHA.110.607739
Komurcu-Bayrak E, Erginel-Unaltuna N, Onat A, Ozsait B, Eklund C, Hurme M, Laaksonen Mononen N (2009) Association of C-reactive protein (CRP) gene allelic variants with serum CRP levels and hypertension in Turkish adults. Atherosclerosis. 206(2):474–479. https://doi.org/10.1016/j.atherosclerosis.2009.03.030
Kong H, Qian Y-S, Tang X-F, Zhang J, Gao P-J, Zhang Y, Zhu D-L (2012) C-reactive protein (CRP) gene polymorphisms, CRP levels and risk of incident essential hypertension: findings from an observational cohort of Han Chinese. Hypertens Res. 35(10):1019–1023. https://doi.org/10.1038/hr.2012.89
Koton S, Sang Y, Schneider ALC, Rosamond WD, Gottesman RF, Coresh J (2020) Trends in stroke incidence rates in older US adults: an update from the Atherosclerosis Risk in Communities (ARIC) Cohort Study. JAMA Neurol. 77(1):109–113. https://doi.org/10.1001/jamaneurol.2019.3258
Kumar A, Misra S, Kumar P, Prasad K, Pandit AK, Chakravarty K, Kathuria P, Gulati A (2017) Association between endothelial nitric oxide synthase gene polymorphisms and risk of ischemic stroke: a meta-analysis. Neurol India. 65(1):22–34. https://doi.org/10.4103/0028-3886.198170
Kumar P, Yadav AK, Kumar A, Sagar R, Pandit AK, Prasad K (2015) Association between interleukin-6 (G174C and G572C) promoter gene polymorphisms and risk of ischaemic stroke: a meta-analysis. Annals Neurosci. 22(2):61–69. https://doi.org/10.5214/ans.0972.7531.220203
Kumar P, Yadav AK, Misra S, Kumar A, Chakravarty K, Prasad K (2016) Role of interleukin-10 (-1082A/G) gene polymorphism with the risk of ischemic stroke: a meta-analysis. Neurol Res. 38(9):823–830. https://doi.org/10.1080/01616412.2016.1202395
Kummer KK, Zeidler M, Kalpachidou T, Kress M (2021) Role of IL-6 in the regulation of neuronal development, survival and function. Cytokine. 144:155582. https://doi.org/10.1016/j.cyto.2021.155582
Küppers E, Beyer C (2001) Dopamine regulates brain-derived neurotrophic factor (BDNF) expression in cultured embryonic mouse striatal cells. Neuroreport. 12(6):1175–1179. https://doi.org/10.1097/00001756-200105080-00025
Lackland Daniel T, Roccella Edward J, Deutsch Anne F, Myriam Fornage, George Mary G, George Howard, Kissela Brett M, Kittner Steven J, Lichtman Judith H, Lisabeth Lynda D, Schwamm Lee H, Smith Eric E, Amytis Towfighi (2014) Factors influencing the decline in stroke mortality. Stroke. 45(1):315–353. https://doi.org/10.1161/01.str.0000437068.30550.cf
Ladenvall C, Jood K, Blomstrand C, Nilsson S, Jern C, Ladenvall P (2006) Serum C-reactive protein concentration and genotype in relation to ischemic stroke subtype. Stroke. 37(8):2018–2023. https://doi.org/10.1161/01.STR.0000231872.86071.68
Lagging C et al (2019) APOE ε4 is associated with younger age at ischemic stroke onset but not with stroke outcome. Neurology. 93(19):849–853. https://doi.org/10.1212/WNL.0000000000008459
Lämmer A, Günther A, Beck A, Krügel U, Kittner H, Schneider D, Illes P, Franke H (2006) Neuroprotective effects of the P2 receptor antagonist PPADS on focal cerebral ischaemia-induced injury in rats. Eur J Neurosci. 23(10):2824–2828. https://doi.org/10.1111/j.1460-9568.2006.04825.x
Langley B, Brochier C, Rivieccio MA (2009) Targeting histone deacetylases as a multifaceted approach to treat the diverse outcomes of stroke. Stroke. 40(8):2899–2905. https://doi.org/10.1161/STROKEAHA.108.540229
Lasek-Bal A, Jędrzejowska-Szypułka H, Różycka J, Bal W, Holecki M, Duława J, Lewin-Kowalik J (2015) Low concentration of BDNF in the acute phase of ischemic stroke as a factor in poor prognosis in terms of functional status of patients. Med Sci Monitor 21:3900–3905. https://doi.org/10.12659/msm.895358
Lau C-H, Muniandy S (2011) Adiponectin and resistin gene polymorphisms in association with their respective adipokine levels. Annals Hum Genet. 75(3):370–382. https://doi.org/10.1111/j.1469-1809.2010.00635.x
Lee KO, Lee KY, Lee CY, Kim JH, Kang J, Lee HY, Na SJ, Oh SH, Heo JH (2021) High serum levels of resistin is associated with acute cerebral infarction. The Neurologist. https://doi.org/10.1097/NRL.0000000000000362
Lee T et al (2016) Identification of PTCSC3 as a novel locus for large-vessel ischemic stroke: a genome-wide association study. J Am Heart Assoc. 5(3):e003003. https://doi.org/10.1161/JAHA.115.003003
Lehnardt S, Lachance C, Patrizi S, Lefebvre S, Follett PL, Jensen FE, Rosenberg PA, Volpe JJ, Vartanian T (2002) The toll-like receptor TLR4 Is necessary for lipopolysaccharide-induced oligodendrocyte injury in the CNS. J Neurosci. 22(7):2478–2486. https://doi.org/10.1523/JNEUROSCI.22-07-02478.2002
Lehotský J, Tothová B, Kovalská M, Dobrota D, Beňová A, Kalenská D, Kaplán P (2016) Role of homocysteine in the ischemic stroke and development of ischemic tolerance. Front Neurosci 10(2016):538. https://doi.org/10.3389/fnins.2016.00538
Lewén A, Matz P, Chan PH (2000) Free radical pathways in CNS injury. J Neurotrauma. 17(10):871–890. https://doi.org/10.1089/neu.2000.17.871
Li Z, Wang M, Gu J, Zhao L, Guo Y, Zhang Z, Liu X (2021) Missense variants in hypoxia-induced VEGFA/VEGFR2 signaling predict the outcome of large artery atherosclerotic stroke. Cell Mol Neurobiol. 41(6):1217–1225. https://doi.org/10.1007/s10571-020-00890-7
Liang Q-J, Jiang M, Wang X-H, Le L-L, Xiang M, Sun N, Meng D, Chen S-F (2015) Pre-existing interleukin 10 in cerebral arteries attenuates subsequent brain injury caused by ischemia/reperfusion. IUBMB LIFE. 67(9):710–719. https://doi.org/10.1002/iub.1429
Liang W, Zhang D, Mang J, He J, Liu H, Shao Y, Han F, Xu Z (2015) Association between phosphodiesterase 4D (PDE4D) SNP 87 and ischemic stroke: a meta-analysis. Int J Clin Experim Med. 8(2):1715–1725
Liepert J, Heller A, Behnisch G, Schoenfeld A (2013) Catechol-O-methyltransferase polymorphism influences outcome after ischemic stroke: a prospective double-blind study. Neurorehabil Neural Repair. 27(6):491–496. https://doi.org/10.1177/1545968313481282
Liesz A, Bauer A, Hoheisel JD, Veltkamp R (2014) Intracerebral interleukin-10 injection modulates post-ischemic neuroinflammation: an experimental microarray study. Neurosci Lett. 579:18–23. https://doi.org/10.1016/j.neulet.2014.07.003
Linacre JM, Heinemann AW, Wright BD, Granger CV, Hamilton BB (1994) The structure and stability of the functional independence measure. Arch Phys Med Rehabil. 75(2):127–132
Liu B, He W, Liu D (2019) Functional BDNF rs7124442 variant regulated by miR-922 is associated with better short-term recovery of ischemic stroke. Therapeut Clin Risk Manag. 15:1369–1375. https://doi.org/10.2147/TCRM.S225536
Liu D, Liu L, Song Z, Hu Z, Liu J, Hou D (2017) Genetic variations of oxidative stress related genes ALOX5, ALOX5AP and MPO modulate ischemic stroke susceptibility through main effects and epistatic interactions in a Chinese population. Cell Physiol Biochem 43(4):1588–1602. https://doi.org/10.1159/000482023
Liu H, Wang Y, Zheng J, Li G, Chen T, Lei J, Mao Y, Wang J, Liu W, Zhao G, Tacey M, Yan B (2017) Platelet glycoprotein gene Ia C807T, HPA-3, and Ibα VNTR polymorphisms are associated with increased ischemic stroke risk: evidence from a comprehensive meta-analysis. Int J Stroke 12(1):46–70. https://doi.org/10.1177/1747493016672085
Liu T, Zhang L, Joo D, Sun SC (2017) NF-κB signaling in inflammation. Signal Transduct Target Therapy. 2:17023. https://doi.org/10.1038/sigtrans.2017.23
Liu W, Yan G (2021) The emerging role of circular RNAs in cerebral vascular disorders. Eur Neurol. 84(4):230–236. https://doi.org/10.1159/000515807
Liu X, Wang L, Wang Q, Zhao J, Chang H, Zhu R (2021) Association between genetic variants in the lncRNA-p53 regulatory network and ischemic stroke prognosis. Neurotoxicity Res. 39(4):1171–1180. https://doi.org/10.1007/s12640-021-00357-7
Liu X, Wang Q, Zhao J, Chang H, Zhu R (2021) Inflammation-related circRNA polymorphism and ischemic stroke prognosis. J Mol Neurosci MN. 71(10):2126–2133. https://doi.org/10.1007/s12031-021-01889-5
Liu X, Zhu R, Li L, Deng S, Li Q, He Z (2013) Genetic polymorphism in PDE4D gene and risk of ischemic stroke in Chinese population: a meta-analysis. PloS One. 8(6):e66374. https://doi.org/10.1371/journal.pone.0066374
Loddick SA, Turnbull AV, Rothwell NJ (1998) Cerebral interleukin-6 is neuroprotective during permanent focal cerebral ischemia in the rat. J Cereb Blood Flow Metab. 18(2):176–179. https://doi.org/10.1097/00004647-199802000-00008
Longchamps RJ, Castellani CA, Yang SY, Newcomb CE, Sumpter JA, Lane J, Grove ML, Guallar E, Pankratz N, Taylor KD, Rotter JI, Boerwinkle E, Arking DE (2020) Evaluation of mitochondrial DNA copy number estimation techniques. PLoS One. 15(1):e0228166. https://doi.org/10.1371/journal.pone.0228166
Luongo C, Dentice M, Salvatore D (2019) Deiodinases and their intricate role in thyroid hormone homeostasis. Nat Rev Endocrinol. 15(8):479–488. https://doi.org/10.1038/s41574-019-0218-2
MacLeod MJ, De Lange RP, Breen G, Meiklejohn D, Lemmon H, Clair DS (2001) Lack of association between apolipoprotein E genoype and ischaemic stroke in a Scottish population. Eur J Clin Investig. 31(7):570–573. https://doi.org/10.1046/j.1365-2362.2001.00851.x
Maguire J, Thakkinstian A, Levi C, Lincz L, Bisset L, Sturm J, Scott R, Whyte S, Attia J (2011) Impact of COX-2 rs5275 and rs20417 and GPIIIa rs5918 polymorphisms on 90-day ischemic stroke functional outcome: a novel finding. J Stroke Cerebrovasc Dis. 20(2):134–144. https://doi.org/10.1016/j.jstrokecerebrovasdis.2009.10.011
Maguire JM et al (2017) GISCOME – genetics of ischaemic stroke functional outcome network: a protocol for an international multicentre genetic association study. Eur Stroke J. 2(3):229–237. https://doi.org/10.1177/2396987317704547
Mahmoudi S, Henriksson S, Corcoran M, Méndez-Vidal C, Wiman KG, Farnebo M (2009) Wrap53, a natural p53 antisense transcript required for p53 induction upon DNA damage. Mol Cell. 33(4):462–471. https://doi.org/10.1016/j.molcel.2009.01.028
Malueka RG, Dwianingsih EK, Sutarni S, Bawono RG, Bayuangga HF, Gofir A, Setyopranoto I (2018) The D allele of the angiotensin-converting enzyme (ACE) insertion/deletion (I/D) polymorphism is associated with worse functional outcome of ischaemic stroke. Int J Neurosci. 128(8):697–704. https://doi.org/10.1080/00207454.2017.1412962
Manso H, Krug T, Sobral J, Albergaria I, Gaspar G, Ferro JM, Oliveira SA, Vicente AM (2010) Variants of the matrix metalloproteinase-2 but not the matrix metalloproteinase-9 genes significantly influence functional outcome after stroke. BMC Med Genet. 11:40. https://doi.org/10.1186/1471-2350-11-40
Markus HS, Mäkelä K-M, Bevan S, Raitoharju E, Oksala N, Bis JC, O’Donnell C, Hainsworth A, Lehtimäki T (2013) Evidence HDAC9 genetic variant associated with ischemic stroke increases risk via promoting carotid atherosclerosis. Stroke. 44(5):1220–1225. https://doi.org/10.1161/STROKEAHA.111.000217
Marousi S, Ellul J, Antonacopoulou A, Gogos C, Papathanasopoulos P, Karakantza M (2011) Functional polymorphisms of interleukin 4 and interleukin 10 may predict evolution and functional outcome of an ischaemic stroke. Eur J Neurol. 18(4):637–643. https://doi.org/10.1111/j.1468-1331.2010.03228.x
Math N, Han TS, Lubomirova I, Hill R, Bentley P, Sharma P (2019) Influences of genetic variants on stroke recovery: a meta-analysis of the 31,895 cases. Neurol Sci. 40(12):2437–2445. https://doi.org/10.1007/s10072-019-04024-w
Matsuda S, Wen TC, Morita F, Otsuka H, Igase K, Yoshimura H, Sakanaka M (1996) Interleukin-6 prevents ischemia-induced learning disability and neuronal and synaptic loss in gerbils. Neurosci Lett. 204(1–2):109–112. https://doi.org/10.1016/0304-3940(96)12340-5
Meseguer E, Diallo D, Labreuche J, Charles H, Delbosc S, Mangin G, Monteiro Tavares L, Caligiuri G, Nicoletti A, Amarenco P (2020) Osteopontin predicts three-month outcome in stroke patients treated by reperfusion therapies. J Clin Med. 9(12):4028. https://doi.org/10.3390/jcm9124028
Meyer E, Vollmer J-Y, Bovey R, Stamenkovic I (2005) Matrix metalloproteinases 9 and 10 inhibit protein kinase C-potentiated, p53-mediated apoptosis. Cancer Res. 65(10):4261–4272. https://doi.org/10.1158/0008-5472.CAN-04-2908
Mola-Caminal M et al (2019) PATJ Low frequency variants are associated with worse ischemic stroke functional outcome. Circul Res. 124(1):114–120. https://doi.org/10.1161/CIRCRESAHA.118.313533
Müller HD, Hanumanthiah KM, Diederich K, Schwab S, Schäbitz W-R, Sommer C (2008) Brain-derived neurotrophic factor but not forced arm use improves long-term outcome after photothrombotic stroke and transiently upregulates binding densities of excitatory glutamate receptors in the rat brain. Stroke. 39(3):1012–1021. https://doi.org/10.1161/STROKEAHA.107.495069
Munton RP, Vizi S, Mansuy IM (2004) The role of protein phosphatase-1 in the modulation of synaptic and structural plasticity. FEBS Letts. 567(1):121–128. https://doi.org/10.1016/j.febslet.2004.03.121
Nayak AR, Kashyap RS, Purohit HJ, Kabra D, Taori GM, Daginawala HF (2009) Evaluation of the inflammatory response in sera from acute ischemic stroke patients by measurement of IL-2 and IL-10. Inflamm Res 58(10):687–691. https://doi.org/10.1007/s00011-009-0036-4
Niwa K, Araki E, Morham SG, Ross ME, Iadecola C (2000) Cyclooxygenase-2 contributes to functional hyperemia in whisker-barrel cortex. J Neurosci. 20(2):763–770. https://doi.org/10.1523/JNEUROSCI.20-02-00763.2000
Niwa K, Haensel C, Ross ME, Iadecola C (2001) Cyclooxygenase-1 participates in selected vasodilator responses of the cerebral circulation. Circul Res. 88(6):600–608. https://doi.org/10.1161/01.res.88.6.600
Noreen M, Shah MAA, Mall SM, Choudhary S, Hussain T, Ahmed I, Jalil SF, Raza MI (2012) TLR4 polymorphisms and disease susceptibility. Inflamm Res. 61(3):177–188. https://doi.org/10.1007/s00011-011-0427-1
Oh HM, Kim T-W, Park H-Y, Kim Y, Park G-Y, Im S (2021) Role of rs6265 BDNF polymorphisms and post-stroke dysphagia recovery-a prospective cohort study. Neurogastroenterol Motility 33(1):e13953. https://doi.org/10.1111/nmo.13953
Olmez I, Ozyurt H (2012) Reactive oxygen species and ischemic cerebrovascular disease. Neurochem Int. 60(2):208–212. https://doi.org/10.1016/j.neuint.2011.11.009
Opatrilova R et al (2018) Adipokines in neurovascular diseases. Biomed Pharmacother Biomed Pharmacother. 98:424–432. https://doi.org/10.1016/j.biopha.2017.12.074
Osawa H et al (2004) The G/G genotype of a resistin single-nucleotide polymorphism at -420 increases type 2 diabetes mellitus susceptibility by inducing promoter activity through specific binding of Sp1/3. Am J Hum Genet. 75(4):678–686. https://doi.org/10.1086/424761
Ostolaza A, Blanco-Luquin I, Urdánoz-Casado A, Rubio I, Labarga A, Zandio B, Roldán M, Martínez-Cascales J, Mayor S, Herrera M, Aymerich N, Gallego J, Muñoz R, Mendioroz M (2020) Circular RNA expression profile in blood according to ischemic stroke etiology. Cell Biosci. 10(1):34. https://doi.org/10.1186/s13578-020-00394-3
Page-McCaw A, Ewald AJ, Werb Z (2007) Matrix metalloproteinases and the regulation of tissue remodelling. Nat Rev Mol Cell Biol. 8(3):221–233. https://doi.org/10.1038/nrm2125
Paraboschi EM, Cardamone G, Soldà G, Duga S, Asselta R (2018) Interpreting non-coding genetic variation in multiple sclerosis genome-wide associated regions. Front Genet 9(2018):647. https://doi.org/10.3389/fgene.2018.00647
Paragliola RM, Corsello A, Papi G, Pontecorvi A, Corsello SM (2021) Cushing’s syndrome effects on the thyroid. Int J Mol Sci. 22(6):3131. https://doi.org/10.3390/ijms22063131
Park TH et al (2020) Neurologic deterioration in patients with acute ischemic stroke or transient ischemic attack. Neurology. 95(16):2178–2191. https://doi.org/10.1212/WNL.0000000000010603
Pendlebury Sarah T, Debbie Poole, Annette Burgess, Julia Duerden, Rothwell Peter M (2020) APOE-ε4 genotype and dementia before and after transient ischemic attack and stroke. Stroke. 51(3):751–758. https://doi.org/10.1161/STROKEAHA.119.026927
Periayah MH, Halim AS, Mat Saad AZ (2017) Mechanism action of platelets and crucial blood coagulation pathways in hemostasis. Int J Hematol Oncol Stem Cell Res. 11(4):319–327
Pfeiffer D et al (2019) Genetic imbalance is associated with functional outcome after ischemic stroke. Stroke. 50(2):298–304. https://doi.org/10.1161/STROKEAHA.118.021856
Phillips MC (2014) Apolipoprotein E isoforms and lipoprotein metabolism. IUBMB Life. 66(9):616–623. https://doi.org/10.1002/iub.1314
Pociot F, Mølvig J, Wogensen L, Worsaae H, Nerup J (1992) A TaqI polymorphism in the human interleukin-1 beta (IL-1 beta) gene correlates with IL-1 beta secretion in vitro. Eur J Clin Investig. 22(6):396–402. https://doi.org/10.1111/j.1365-2362.1992.tb01480.x
Poletto M, Legrand AJ, Fletcher SC, Dianov GL (2016) p53 coordinates base excision repair to prevent genomic instability. Nucleic Acids Res. 44(7):3165–3175. https://doi.org/10.1093/nar/gkw015
Polvikoski T, Sulkava R, Haltia M, Kainulainen K, Vuorio A, Verkkoniemi A, Niinistö L, Halonen P, Kontula K (1995) Apolipoprotein E, dementia, and cortical deposition of beta-amyloid protein. N Engl J Med. 333(19):1242–1247. https://doi.org/10.1056/NEJM199511093331902
Protti GG, Gagliardi RJ, Forte WCN, Sprovieri SRS (2013) Interleukin-10 may protect against progressing injury during the acute phase of ischemic stroke. Arquivos De Neuro-Psiquiatria. 71(11):846–851. https://doi.org/10.1590/0004-282X20130168
Quinn Terence J, Peter Langhorne, Stott David J (2011) Barthel index for stroke trials. Stroke. 42(4):1146–1151. https://doi.org/10.1161/STROKEAHA.110.598540
Rannikmäe K, Kalaria RN, Greenberg SM, Chui HC, Schmitt FA, Samarasekera N, Salman RA-S, Sudlow CL (2014) APOE associations with severe CAA-associated vasculopathic changes – collaborative meta-analysis. J Neurol Neurosurg Psychiatry. 85(3):300–305. https://doi.org/10.1136/jnnp-2013-306485
Rezk NA, Mohamad HS (2015) Influence of interleukin-1 gene cluster polymorphisms on the susceptibility and outcomes of acute stroke in Egyptian patients. Cell Biochem Biophys. 71(2):637–647. https://doi.org/10.1007/s12013-014-0243-7
Rigat B, Hubert C, Alhenc-Gelas F, Cambien F, Corvol P, Soubrier F (1990) An insertion/deletion polymorphism in the angiotensin I-converting enzyme gene accounting for half the variance of serum enzyme levels. J Clin Investig. 86(4):1343–1346. https://doi.org/10.1172/JCI114844
van Rijn MJE, Slooter AJC, Bos MJ, Catarino CFBS, Koudstaal PJ, Hofman A, Breteler MMB, van Duijn CM (2006) Insulin-like growth factor I promoter polymorphism, risk of stroke, and survival after stroke: the Rotterdam study. J Neurol Neurosurg Psychiatry. 77(1):24–27. https://doi.org/10.1136/jnnp.2005.067447
Rodríguez C, Ramos-Araque ME, Domínguez-Martínez M, Sobrino T, Sánchez-Morán I, Agulla J, Delgado-Esteban M, Gómez-Sánchez JC, Bolaños JP, Castillo J, Almeida A (2018) Single-nucleotide polymorphism 309T>G in the MDM2 promoter determines functional outcome after stroke. Stroke. 49(10):2437–2444. https://doi.org/10.1161/STROKEAHA.118.022529
Roef GL, Rietzschel ER, De Meyer T, Bekaert S, De Buyzere ML (2013) Associations between single nucleotide polymorphisms in thyroid hormone transporter genes (MCT8, MCT10 and OATP1C1) and circulating thyroid hormones. Clinica Chimica Acta Int J Clin Chem 425:227–232. https://doi.org/10.1016/j.cca.2013.08.017
Rosenberg GA, Estrada EY, Dencoff JE (1998) Matrix metalloproteinases and TIMPs are associated with blood-brain barrier opening after reperfusion in rat brain. Stroke. 29(10):2189–2195. https://doi.org/10.1161/01.str.29.10.2189
Ruggeri Zaverio M, Loredana Mendolicchio G (2007) Adhesion mechanisms in platelet function. Circul Res. 100(12):1673–1685. https://doi.org/10.1161/01.RES.0000267878.97021.ab
Samarasekera N, Smith C, Al-Shahi Salman R (2012) The association between cerebral amyloid angiopathy and intracerebral haemorrhage: systematic review and meta-analysis. J Neurol Neurosurg Psychiatry. 83(3):275–281. https://doi.org/10.1136/jnnp-2011-300371
Sánchez-Morán I, Rodríguez C, Lapresa R, Agulla J, Sobrino T, Castillo J, Bolaños JP, Almeida A (2020) Nuclear WRAP53 promotes neuronal survival and functional recovery after stroke. Sci Adv. https://doi.org/10.1126/sciadv.abc5702
Santoro M, Siotto M, Germanotta M, Bray E, Mastrorosa A, Galli C, Papadopoulou D, Aprile I (2020) BDNF rs6265 polymorphism and its methylation in patients with stroke undergoing rehabilitation. Int J Mol Sci. https://doi.org/10.3390/ijms21228438
Sas AA, Vaez A, Jamshidi Y, Nolte IM, Kamali Z, Spector D (2017) Genetic and environmental influences on stability and change in baseline levels of C-reactive protein: a longitudinal twin study. Atherosclerosis. 265:172–178. https://doi.org/10.1016/j.atherosclerosis.2017.08.008
Sassone-Corsi P (2012) The Cyclic AMP Pathway. Cold Spring Harbor Perspect Biol. 4(12):a011148. https://doi.org/10.1101/cshperspect.a011148
Schäbitz WR, Sommer C, Zoder W, Kiessling M, Schwaninger M, Schwab S (2000) Intravenous brain-derived neurotrophic factor reduces infarct size and counterregulates Bax and Bcl-2 expression after temporary focal cerebral ischemia. Stroke. 31(9):2212–2217. https://doi.org/10.1161/01.str.31.9.2212
Serhan A, Aerts JL, Boddeke EWGM, Kooijman R (2020) Neuroprotection by insulin-like growth factor-1 in rats with ischemic stroke is associated with microglial changes and a reduction in neuroinflammation. Neuroscience. 426:101–114. https://doi.org/10.1016/j.neuroscience.2019.11.035
Shaafi S, Sharifipour E, Rahmanifar R, Hejazi S, Andalib S, Nikanfar M, Baradarn B, Mehdizadeh R (2014) Interleukin-6, a reliable prognostic factor for ischemic stroke. Iranian J Neurol. 13(2):70–76
Shah AB, Beamer N, Coull BM (1985) Enhanced in vivo platelet activation in subtypes of ischemic stroke. Stroke. 16(4):643–647. https://doi.org/10.1161/01.STR.16.4.643
Shah S, Vanclay F, Cooper B (1989) Improving the sensitivity of the Barthel Index for stroke rehabilitation. J Clin Epidemiol. 42(8):703–709. https://doi.org/10.1016/0895-4356(89)90065-6
Shimamura M, Nakagami H, Osako MK, Kurinami H, Koriyama H, Zhengda P, Tomioka H, Tenma A, Wakayama K, Morishita R (2014) OPG/RANKL/RANK axis is a critical inflammatory signaling system in ischemic brain in mice. Proc Natl Acad Sci. 111(22):8191–8196. https://doi.org/10.1073/pnas.1400544111
Shin K, Straight S, Margolis B (2005) PATJ regulates tight junction formation and polarity in mammalian epithelial cells. J Cell Biol 168(5):705–711. https://doi.org/10.1083/jcb.200408064
Shiner CT, Pierce KD, Thompson-Butel AG, Trinh T, Schofield PR, McNulty PA (2016) BDNF genotype interacts with motor function to influence rehabilitation responsiveness poststroke. Front Neurol 7(2016):69. https://doi.org/10.3389/fneur.2016.00069
Shkirkova K, Saver JL, Starkman S, Wong G, Weng J, Hamilton S, Liebeskind DS, Eckstein M, Stratton S, Pratt F, Conwit R, Sanossian N, FAST-MAG Trial Coordinators and Investigators (2018) Frequency, predictors, and outcomes of prehospital and early postarrival neurological deterioration in acute stroke: exploratory analysis of the FAST-MAG randomized clinical trial. JAMA Neurol. 75(11):1364–1374. https://doi.org/10.1001/jamaneurol.2018.1893
Siironen J, Juvela S, Kanarek K, Vilkki J, Hernesniemi J, Lappalainen J (2007) The Met allele of the BDNF Val66Met polymorphism predicts poor outcome among survivors of aneurysmal subarachnoid hemorrhage. Stroke. 38(10):2858–2860. https://doi.org/10.1161/STROKEAHA.107.485441
Silva IP, Salhi A, Giles KM, Vogelsang M, Han SW, Ismaili N, Lui KP, Robinson EM, Wilson M, Shapiro RL, Pavlick A, Zhong J, Kirchhoff T, Osman I (2016) Identification of a novel pathogenic germline KDR variant in melanoma. Clin Cancer Res. 22(10):2377–2385. https://doi.org/10.1158/1078-0432.CCR-15-1811
Sims JE, Smith DE (2010) The IL-1 family: regulators of immunity. Nat Rev Immunol 10(2):89–102. https://doi.org/10.1038/nri2691
Sims NR, Muyderman H (2010) Mitochondria, oxidative metabolism and cell death in stroke. Biochimica Et Biophysica Acta. 1:80–91. https://doi.org/10.1016/j.bbadis.2009.09.003
Singh HV, Pandey A, Shrivastava AK, Raizada A, Singh SK, Singh N (2013) Prognostic value of neuron specific enolase and IL-10 in ischemic stroke and its correlation with degree of neurological deficit. Clinica Chimica Acta Int J Clin Chem. 419:136–138. https://doi.org/10.1016/j.cca.2013.02.014
Smith CJ, Emsley HC, Gavin CM, Georgiou RF, Vail A, Barberan EM, del Zoppo GJ, Hallenbeck JM, Rothwell NJ, Hopkins SJ, Tyrrell PJ (2004) Peak plasma interleukin-6 and other peripheral markers of inflammation in the first week of ischaemic stroke correlate with brain infarct volume, stroke severity and long-term outcome. BMC Neurol. 4:2. https://doi.org/10.1186/1471-2377-4-2
Smith CJ, Hulme S, Vail A, Heal C, Parry-Jones AR, Scarth S, Hopkins K, Hoadley M, Allan SM, Rothwell NJ, Hopkins SJ, Tyrrell PJ (2018) SCIL-STROKE (Subcutaneous Interleukin-1 receptor antagonist in ischemic stroke): a randomized controlled phase 2 trial. Stroke. 49(5):1210–1216. https://doi.org/10.1161/STROKEAHA.118.020750
Sobowale OA, Parry-Jones AR, Smith CJ, Tyrrell PJ, Rothwell NJ, Allan SM (2016) Interleukin-1 in stroke. Stroke. 47(8):2160–2167. https://doi.org/10.1161/STROKEAHA.115.010001
Söderholm M et al (2019) Genome-wide association meta-analysis of functional outcome after ischemic stroke. Neurology. https://doi.org/10.1212/WNL.0000000000007138
Song L, Liu T, Song Y, Sun Y, Li H, Xiao N, Xu H, Ge J, Bai C, Wen H, Zhang Y, Hui R, Chen J (2020) mtDNA Copy number contributes to all-cause mortality of lacunar infarct in a Chinese prospective stroke population. J Cardiovasc Translat Res. 13(5):783–789. https://doi.org/10.1007/s12265-019-09943-9
Song TJ, Kim J, Yang SH, Park JH, Lee HS, Nam CM, Lee OH, Kim YD, Nam HS, Heo JH (2012) Association of plasma osteoprotegerin levels with stroke severity and functional outcome in acute ischaemic stroke patients. Biomarkers 17(8):738–744. https://doi.org/10.3109/1354750X.2012.727027
Song Y, Wang C, Wu Y, Lin J, Wang P, Du W, Liu L, Lin J, Wang Y, Wang Y, Liu G (2017) Phosphodiesterase 4D polymorphisms associate with the short-term outcome in ischemic stroke. Scient Rep. 7(1):42914. https://doi.org/10.1038/srep42914
Spera PA, Ellison JA, Feuerstein GZ, Barone FC (1998) IL-10 reduces rat brain injury following focal stroke. Neurosci Lett. 251(3):189–192. https://doi.org/10.1016/S0304-3940(98)00537-0
Sproston NR, Ashworth JJ (2018) Role of C-reactive protein at sites of inflammation and infection. Front Immunol 9:754. https://doi.org/10.3389/fimmu.2018.00754
Stanne TM, Åberg ND, Nilsson S, Jood K, Blomstrand C, Andreasson U, Blennow K, Zetterberg H, Isgaard J, Svensson J, Jern C (2016) Low circulating acute brain-derived neurotrophic factor levels are associated with poor long-term functional outcome after ischemic stroke. Stroke. 47(7):1943–1945. https://doi.org/10.1161/STROKEAHA.115.012383
Stanne TM, Tjärnlund-Wolf A, Olsson S, Jood K, Blomstrand C, Jern C (2014) Genetic variation at the BDNF locus: evidence for association with long-term outcome after ischemic stroke. PloS one. 9(12):e114156. https://doi.org/10.1371/journal.pone.0114156
Straface G et al (2011) Assessment of the Genetic Effects Of Polymorphisms In The Osteoprotegerin Gene, TNFRSF11B, on serum osteoprotegerin levels and carotid plaque vulnerability. Stroke. 42(11):3022–3028. https://doi.org/10.1161/STROKEAHA.111.619288
Sui L, Ren W-W, Li B-M (2010) Administration of thyroid hormone increases reelin and brain-derived neurotrophic factor expression in rat hippocampus in vivo. Brain Res. 1313:9–24. https://doi.org/10.1016/j.brainres.2009.12.010
Tang L, Zhang L, Ding H, Tu W, Yan J (2010) GTP cyclohydrolase 1 gene 3’-UTR C+243T variant predicts worsening outcome in patients with first-onset ischemic stroke. J Huazhong University Sci Technol Med Sci = Hua Zhong Ke Ji Da Xue Xue Bao. Yi Xue Ying De Wen Ban = Huazhong Keji Daxue Xuebao. Yixue Yingdewen Ban. 30(6):694–698. https://doi.org/10.1007/s11596-010-0642-y
Tarkowski E, Rosengren L, Blomstrand C, Wikkelsö C, Jensen C, Ekholm S, Tarkowski A (1995) Early intrathecal production of interleukin-6 predicts the size of brain lesion in stroke. Stroke. 26(8):1393–1398. https://doi.org/10.1161/01.str.26.8.1393
Taroza S, Rastenytė D, Podlipskytė A, Patamsytė V, Mickuvienė N (2019) Deiodinases, organic anion transporter polypeptide polymorphisms and ischemic stroke outcomes. J Neurol Sci. 407:116457. https://doi.org/10.1016/j.jns.2019.116457
Thurston G, Rudge JS, Ioffe E, Zhou H, Ross L, Croll SD, Glazer N, Holash J, McDonald DM, Yancopoulos GD (2000) Angiopoietin-1 protects the adult vasculature against plasma leakage. Nat Med. 6(4):460–463. https://doi.org/10.1038/74725
Torres-Aguila NP et al (2019) Clinical variables and genetic risk factors associated with the acute outcome of ischemic stroke: a systematic review. J Stroke. 21(3):276–289. https://doi.org/10.5853/jos.2019.01522
Traylor M et al (2012) Genetic risk factors for ischaemic stroke and its subtypes (the METASTROKE collaboration): a meta-analysis of genome-wide association studies. Lancet Neurol. 11(11):951–962. https://doi.org/10.1016/S1474-4422(12)70234-X
Tso AR, Merino JG, Warach S (2007) Interleukin-6 −174G/C Polymorphism and Ischemic Stroke. Stroke. 38(11):3070–3075. https://doi.org/10.1161/STROKEAHA.107.492231
Tu J, Wang L-P (2009) Therapeutic potential of extracellular ATP and P2 receptors in nervous system diseases. Neurosci Bull. 25(1):27–32. https://doi.org/10.1007/s12264-009-1020-2
Uchiyama S, Takeuchi M, Osawa M, Kobayashi I, Maruyama S, Aosaki M, Hirosawa K (1983) Platelet function tests in thrombotic cerebrovascular disorders. Stroke. 14(4):511–517. https://doi.org/10.1161/01.STR.14.4.511
Uchiyama S, Yamazaki M, Maruyama S, Handa M, Ikeda Y, Fukuyama M, Itagaki I (1994) Shear-induced platelet aggregation in cerebral ischemia. Stroke. 25(8):1547–1551. https://doi.org/10.1161/01.str.25.8.1547
Urra X, Cervera A, Obach V, Climent N, Planas AM, Chamorro A (2009) Monocytes are major players in the prognosis and risk of infection after acute stroke. Stroke. 40(4):1262–1268. https://doi.org/10.1161/STROKEAHA.108.532085
Vaessen N, Heutink P, Janssen JA, Witteman JC, Testers L, Hofman A, Lamberts SW, Oostra BA, Pols HA, van Duijn CM (2001) A polymorphism in the gene for IGF-I: functional properties and risk for type 2 diabetes and myocardial infarction. Diabetes. 50(3):637–642. https://doi.org/10.2337/diabetes.50.3.637
Van Campenhout A, Golledge J (2009) Osteoprotegerin, vascular calcification and atherosclerosis. Atherosclerosis. 204(2):321–329. https://doi.org/10.1016/j.atherosclerosis.2008.09.033
Vermot A, Petit-Härtlein I, Smith SME, Fieschi F (2021) NADPH oxidases (NOX): an overview from discovery, molecular mechanisms to physiology and pathology. Antioxidants (Basel, Switzerland). 10(6):890. https://doi.org/10.3390/antiox10060890
Vila N, Castillo J, Dávalos A, Esteve A, Planas AM, Chamorro Á (2003) Levels of anti-inflammatory cytokines and neurological worsening in acute ischemic stroke. Stroke. 34(3):671–675. https://doi.org/10.1161/01.STR.0000057976.53301.69
Virani Salim S et al (2020) Heart disease and stroke statistics—(2020) Update: a report from the American Heart Association. Circulation. 141(9):e139–e596. https://doi.org/10.1161/CIR.0000000000000757
van der Vliet R, Ribbers GM, Vandermeeren Y, Frens MA, Selles RW (2017) BDNF Val66Met but not transcranial direct current stimulation affects motor learning after stroke. Brain Stimul. 10(5):882–892. https://doi.org/10.1016/j.brs.2017.07.004
Wan L, Li Y, Zhang Z, Sun Z, He Y, Li R (2018) Methylenetetrahydrofolate reductase and psychiatric diseases. Translat Psychiatry. 8(1):1–12. https://doi.org/10.1038/s41398-018-0276-6
Wang J, Gao L, Yang Y-L, Li Y-Q, Chang T, Man M-H, Zhang X-Y, Guo S-C, Li L-H (2017) Low serum levels of brain-derived neurotrophic factor were associated with poor short-term functional outcome and mortality in acute ischemic stroke. Mol Neurobiol. 54(9):7335–7342. https://doi.org/10.1007/s12035-016-0236-1
Wang L, Li Y, Wang C, Guo W, Liu M (2019) C-reactive protein, infection, and outcome after acute ischemic stroke: a registry and systematic review. Curr Neurovasc Res. 16(5):405–415. https://doi.org/10.2174/1567202616666191026122011
Wang M et al (2019) HDAC9 polymorphisms predict susceptibility, severity, and short-term outcome of large artery atherosclerotic stroke in chinese population. J Mol Neurosci MN. 67(1):165–171. https://doi.org/10.1007/s12031-018-1221-0
Wang M, Gu M, Li Z, Lian X, Shen H, Dai Z, Zhang Z, Liu X (2020) TNFRSF11B polymorphisms predict poor outcome after large artery atherosclerosis stroke. Gene. 743:144617. https://doi.org/10.1016/j.gene.2020.144617
Wang W-J, Lyu T-J, Li Z (2021) Research progress on PATJ and underlying mechanisms associated with functional outcomes after stroke. Neuropsychiatr Dis Treat. 17:2811–2818. https://doi.org/10.2147/NDT.S310764
Wang Y, Huang Q, Liu J, Wang Y, Zheng G, Lin L, Yu H, Tang W, Huang Z (2017) Vascular endothelial growth factor A polymorphisms are associated with increased risk of coronary heart disease: a meta-analysis. Oncotarget. 8(18):30539 https://doi.org/10.18632/oncotarget.15546
Ward NC, Croft KD, Blacker D, Hankey GJ, Barden A, Mori TA, Puddey IB, Beer CD (2011) Cytochrome P450 metabolites of arachidonic acid are elevated in stroke patients compared with healthy controls. Clin Sci. 121(11):501–507. https://doi.org/10.1042/CS20110215
Wei Y, Yang J, He Y, Shi X, Zeng Z (2019) A functional polymorphism in the promoter of TUG1 is associated with an increased risk of ischaemic stroke. J Cell Mol Med. 23(9):6173–6181. https://doi.org/10.1111/jcmm.14499
Weinstein JR, Schulze J, Lee RV, Phillips H, Zierath D, Tanzi P, Shibata D, Cain KC, Becker KJ (2014) Functional polymorphisms in toll-like receptor 4 are associated with worse outcome in acute ischemic stroke patients. Neuroreport. 25(8):580–584. https://doi.org/10.1097/WNR.0000000000000140
Werden E, Khlif MS, Bird LJ, Cumming T, Bradshaw J, Khan W, Pase M, Restrepo C, Veldsman M, Egorova N, Patel SK, Gottlieb E, Brodtmann A (2019) APOE ɛ4 carriers show delayed recovery of verbal memory and smaller entorhinal volume in the first year after ischemic stroke. J Alzheimer’s Dis JAD. 71(1):245–259. https://doi.org/10.3233/JAD-190566
Williams SN, Undieh AS (2009) Dopamine D1-like receptor activation induces brain-derived neurotrophic factor protein expression. Neuroreport. 20(6):606–610. https://doi.org/10.1097/WNR.0b013e32832a0a98
Witte AV, Flöel A (2012) Effects of COMT polymorphisms on brain function and behavior in health and disease. Brain Res Bull. 88(5):418–428. https://doi.org/10.1016/j.brainresbull.2011.11.012
Witte AV, Kürten J, Jansen S, Schirmacher A, Brand E, Sommer J, Flöel A (2012) Interaction of BDNF and COMT polymorphisms on paired-associative stimulation-induced cortical plasticity. J Neurosci 32(13):4553–4561. https://doi.org/10.1523/JNEUROSCI.6010-11.2012
Wittmann G, Szabon J, Mohácsik P, Nouriel SS, Gereben B, Fekete C, Lechan RM (2015) Parallel regulation of thyroid hormone transporters OATP1c1 and MCT8 during and after endotoxemia at the blood-brain barrier of male rodents. Endocrinology. 156(4):1552–1564. https://doi.org/10.1210/en.2014-1830
Wolak T (2014) Osteopontin – A multi-modal marker and mediator in atherosclerotic vascular disease. Atherosclerosis. 236(2):327–337. https://doi.org/10.1016/j.atherosclerosis.2014.07.004
Wrigley S, Arafa D, Tropea D (2017) Insulin-like growth factor 1: at the crossroads of brain development and aging. Front Cell Neurosci. 11:14. https://doi.org/10.3389/fncel.2017.00014
Wzorek J, Karpiński M, Wypasek E, Michalski M, Szczudlik A, Malinowski KP, Undas A (2018) Alpha-2-antiplasmin Arg407Lys polymorphism and cryptogenic ischemic cerebrovascular events: Association with neurological deficit. Neurologia I Neurochirurgia Polska. 52(3):352–358. https://doi.org/10.1016/j.pjnns.2017.12.009
Xie G, Myint PK, Zaman MJS, Li Y, Zhao L, Shi P, Ren F, Wu Y (2013) Relationship of serum interleukin-10 and its genetic variations with ischemic stroke in a Chinese general population. PloS One. 8(9):e74126. https://doi.org/10.1371/journal.pone.0074126
Xin M, Feng J, Hao Y, You J, Wang X, Yin X, Shang P, Ma D (2020) Cyclic adenosine monophosphate in acute ischemic stroke: some to update, more to explore. J Neurol Sci. 413:116775. https://doi.org/10.1016/j.jns.2020.116775
Yamashita T, Sawamoto K, Suzuki S, Suzuki N, Adachi K, Kawase T, Mihara M, Ohsugi Y, Abe K, Okano H (2005) Blockade of interleukin-6 signaling aggravates ischemic cerebral damage in mice: possible involvement of Stat3 activation in the protection of neurons. J Neurochem. 94(2):459–468. https://doi.org/10.1111/j.1471-4159.2005.03227.x
Yamazaki Y, Zhao N, Caulfield TR, Liu C-C, Bu G (2019) Apolipoprotein E and Alzheimer disease: pathobiology and targeting strategies. Nat Rev Neurol 15(9):501–518. https://doi.org/10.1038/s41582-019-0228-7
Yan J, Jm G, Pa M (2016) Interleukin 6 promoter 174 G/C polymorphisms in acute ischemic stroke: G allele is protective but not associated with IL-6 levels or stroke outcome. J Neuroimmunol. 293:22–27. https://doi.org/10.1016/j.jneuroim.2016.02.001
Yang Q, Li J, Lu F, Wen A, Xiang J, Zhang L, Huang Z, Wang J (2008) Upregulated expression of toll-like receptor 4 in monocytes correlates with severity of acute cerebral infarction. J Cereb Blood Flow Metabol. 28(9):1588–1596. https://doi.org/10.1038/jcbfm.2008.50
Yang Y, Candelario-Jalil E, Thompson JF, Cuadrado E, Estrada EY, Rosell A, Montaner J, Rosenberg GA (2010) Increased intranuclear matrix metalloproteinase activity in neurons interferes with oxidative DNA repair in focal cerebral ischemia. J Neurochem. 112(1):134–149. https://doi.org/10.1111/j.1471-4159.2009.06433.x
Yang Y, Rosenberg GA (2015) Matrix metalloproteinases as therapeutic targets for stroke. Brain Res. 1623:30–38. https://doi.org/10.1016/j.brainres.2015.04.024
Yao L, Kan EM, Lu J, Hao A, Dheen ST, Kaur C, Ling E-A (2013) Toll-like receptor 4 mediates microglial activation and production of inflammatory mediators in neonatal rat brain following hypoxia: role of TLR4 in hypoxic microglia. J Neuroinflamm. 10(1):785. https://doi.org/10.1186/1742-2094-10-23
Ye Z, Zhang H, Sun L, Cai H, Hao Y, Xu Z, Zhang Z, Liu X (2018) GWAS-supported CRP Gene polymorphisms and functional outcome of large artery atherosclerotic stroke in Han Chinese. Neuromol Med. 20(2):225–232. https://doi.org/10.1007/s12017-018-8485-y
Yi X, Liao D, Wu L, Chen H, Li J, Wang C (2016) CYP genetic variants, CYP metabolite levels, and symptomatic carotid stenosis in ischemic stroke patients. J Atheroscler Thromb. 23(5):621–631. https://doi.org/10.5551/jat.32714
Yi X, Lin J, Li J, Zhou Q, Han Z (2017) Epoxyeicosatrienoic acids are mediated by EPHX2 variants and may be a predictor of early neurological deterioration in acute minor ischemic stroke. J Atheroscler Thromb. 24(12):1258–1266. https://doi.org/10.5551/jat.41145
Yi X, Lin J, Wang C, Zhou Q (2017) CYP genetic variants, CYP metabolite levels, and neurologic deterioration in acute ischemic stroke in chinese population. J Stroke Cerebrovasc Dis. 26(5):969–978. https://doi.org/10.1016/j.jstrokecerebrovasdis.2016.11.004
Yi X, Ming B, Wang C, Chen H, Ma C (2017) Variants in COX-2, PTGIS, and TBXAS1 are associated with carotid artery or intracranial arterial stenosis and neurologic deterioration in ischemic stroke patients. J Stroke Cerebrovasc Dis 26(5):1128–1135. https://doi.org/10.1016/j.jstrokecerebrovasdis.2016.12.032
Yi X, Wang C, Zhou Q, Lin J (2017) Interaction among COX-2, P2Y1 and GPIIIa gene variants is associated with aspirin resistance and early neurological deterioration in Chinese stroke patients. BMC Neurol. https://doi.org/10.1186/s12883-016-0788-8
Yi X, Wu L, Liao D, Wang C, Zhang B (2016) Interactions Among CYP2C8, EPHX2, and CYP4A11 Variants and CYP Plasma Metabolite Levels in Ischemic Stroke. J Atheroscler Thromb. 23(11):1286–1293. https://doi.org/10.5551/jat.35279
Yi X, Zhou Q, Sui G, Ren G, Tan L, Li J, Lin J, Bao S (2021) Interactions among variants in P53 apoptotic pathway genes are associated with neurologic deterioration and functional outcome after acute ischemic stroke. Brain Behav. 11(5):e01492. https://doi.org/10.1002/brb3.1492
Yi X-Y, Liao D-X, Wang C, Cheng W, Fu X-Q, Zhang B (2016) Cytochrome P450 genetic variants and their metabolite levels associated with plaque stability in patients with ischemic stroke. J Atheroscler Thromb. 23(3):330–338. https://doi.org/10.5551/jat.31120
Yin G-T, Ma Y-T, Zheng Y-Y, Yang Y-N, Li X-M, Fu Z-Y, Zhang J-Z, Dai C-F, Liu F, Chen B-D, Gai M-T, Xie X (2015) Polymorphisms of interleukin-10 genes on the risk of ischemic stroke in a meta-analysis. Int J Clin Experim Med. 8(2):1888–1895
Yuan S, Chan HS, Vogel H, Filipek S, Stevens RC, Palczewski K (2016) The molecular mechanism of P2Y1 receptor activation. Angewandte Chemie. 128(35):10487–91. https://doi.org/10.1002/anie.201605147
Zhang E, Yin D, Sun M, Kong R, Liu X, You L, Han L, Xia R, Wang K, Yang J, De W, Shu Y, Wang Z (2014) P53-regulated long non-coding RNA TUG1 affects cell proliferation in human non-small cell lung cancer, partly through epigenetically regulating HOXB7 expression. Cell Death Dis. 5(5):e1243. https://doi.org/10.1038/cddis.2014.201
Zhang F, Gu W, Hurles ME, Lupski JR (2009) Copy number variation in human health, disease, and evolution. Annu Rev Genomics Hum Genet 10(2009):451–481. https://doi.org/10.1146/annurev.genom.9.081307.164217
Zhang L et al (2007) Discovery of common human genetic variants of GTP cyclohydrolase 1 (GCH1) governing nitric oxide, autonomic activity, and cardiovascular risk. J Clin Investig. 117(9):2658–2671. https://doi.org/10.1172/JCI31093
Zhang L, Chopp M, Meier DH, Winter S, Wang L, Szalad A, Lu M, Wei M, Cui Y, Zhang ZG (2013) Sonic Hedgehog signaling pathway mediates cerebrolysin-improved neurological function after stroke. Stroke. 44(7):1965–1972. https://doi.org/10.1161/STROKEAHA.111.000831
Zhang Y, Liu S, Yue W, Shi Z, Guan Y, Li M, Ji Y, Li X (2017) Association of apolipoprotein E genotype with outcome in hospitalized ischemic stroke patients. Medicine. 96(50):e8964. https://doi.org/10.1097/MD.0000000000008964
Zhang Y, Meyer MA (2010) Clinical analysis on alteration of thyroid hormones in the serum of patients with acute ischemic stroke. Stroke Res Treatment. https://doi.org/10.4061/2010/290678
Zhang Z, Xu G, Liu D, Fan X, Zhu W, Liu X (2012) Angiotensin-converting enzyme insertion/deletion polymorphism contributes to ischemic stroke risk: a meta-analysis of 50 case-control studies. PLoS One. 7(10):e46495. https://doi.org/10.1371/journal.pone.0046495
Zhao J, Bai Y, Jin L, Weng Y, Wang Y, Wu H, Li X, Huang Y, Wang S (2017) A functional variant in the 3’-UTR of VEGF predicts the 90-day outcome of ischemic stroke in Chinese patients. PloS One. 12(2):e0172709. https://doi.org/10.1371/journal.pone.0172709
Zhao J, Wu H, Zheng L, Weng Y, Mo Y (2013) Brain-derived neurotrophic factor G196A polymorphism predicts 90-day outcome of ischemic stroke in Chinese: a novel finding. Brain Res. 1537:312–318. https://doi.org/10.1016/j.brainres.2013.08.061
Zhao L, Fang J, Zhou M, Zhou J, Yu L, Chen N, He L (2019) Interaction between COX-1 and COX-2 increases susceptibility to ischemic stroke in a Chinese population. BMC Neurol. 19(1):291. https://doi.org/10.1186/s12883-019-1505-1
Zhou J, Ma M-M, Fang J-H, Zhao L, Zhou M-K, Guo J, He L (2019) Differences in brain-derived neurotrophic factor gene polymorphisms between acute ischemic stroke patients and healthy controls in the Han population of southwest China. Neural Regener Res. 14(8):1404–1411. https://doi.org/10.4103/1673-5374.253525
Zhou Y, Han W, Gong D, Man C, Fan Y (2016) Hs-CRP in stroke: a meta-analysis. Clinica Chimica Acta Int J Clin Chem. 453:21–27. https://doi.org/10.1016/j.cca.2015.11.027
Zhou Y, Yao Y, Sheng L, Zhang J, Zhang JH, Shao A (2020) Osteopontin as a candidate of therapeutic application for the acute brain injury. J Cell Mol Med. 24(16):8918–8929. https://doi.org/10.1111/jcmm.15641
Zhou YL, Wu WP, Cheng J, Liang LL, Cen JM, Chen C, Liu X, Xiong XD (2020) CircFOXO3 rs12196996, a polymorphism at the gene flanking intron, is associated with circFOXO3 levels and the risk of coronary artery disease. Aging (Albany NY). 12(13):13076
Zhu H, Jian Z, Zhong Y, Ye Y, Zhang Y, Hu X, Pu B, Gu L, Xiong X (2021) Janus kinase inhibition ameliorates ischemic stroke injury and neuroinflammation through reducing NLRP3 inflammasome activation via JAK2/STAT3 pathway inhibition. Front Immunol. https://doi.org/10.3389/fimmu.2021.714943
Zhu R, Zhao Y, Tian D, Guo N, Zhang C, Liu X (2021) GWAS-linked hot loci predict short-term functional outcome and recurrence of ischemic stroke in Chinese population. Am J Translat Res 13(5):4521–4534
Zuo L et al (2020) Circulating circular RNAs as biomarkers for the diagnosis and prediction of outcomes in acute ischemic stroke. Stroke. 51(1):319–323. https://doi.org/10.1161/STROKEAHA.119.027348
(2012) C-reactive protein, fibrinogen, and cardiovascular disease prediction. N Engl J Med 367(14):1310–1320. https://doi.org/10.1056/NEJMoa1107477
(2012) Genome-wide association study identifies a variant in HDAC9 associated with large vessel ischemic stroke. Nat Genet 44(3):328–333. https://doi.org/10.1038/ng.1081
(2018) Global, regional, and country-specific lifetime risks of stroke, 1990 and 2016. N Engl J Med 379(25):2429–2437. https://doi.org/10.1056/NEJMoa1804492
(2012) Interleukin-6 receptor pathways in coronary heart disease: a collaborative meta-analysis of 82 studies. The Lancet. 379(9822):1205–1213. https://doi.org/10.1016/S0140-6736(11)61931-4
Funding
No funding was received to assist with the preparation of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors have no relevant financial or non-financial interests to disclose.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Carnwath, T.P., Demel, S.L. & Prestigiacomo, C.J. Genetics of ischemic stroke functional outcome. J Neurol 271, 2345–2369 (2024). https://doi.org/10.1007/s00415-024-12263-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-024-12263-x