
Abstract
Cerebellar ataxia with neuropathy and bilateral vestibular areflexia syndrome (CANVAS) is an hereditary autosomal recessive disease. Recent studies propose including chronic cough (CC) as a symptom of CANVAS. For 10 patients with CANVAS as genetically confirmed by biallelic expansion of the AAGG repeat motif (AAGGGexp) in intron 2 of replication factor C subunit 1 (RFC1), our aim was, as a multidisciplinary team, to describe clinical and functional characteristics and possible causes of CC following European Respiratory Society (ERS) recommendations, and to evaluate CC impact on quality of life (QoL) using self-administered questionnaires (Cough Severity Diary, Leicester Cough Questionnaire, Discrete Emotions Questionnaire, and EQ-5D-5L). In all 10 patients, the CC was a dry cough that developed several years prior to the neurological symptoms (mean 14.2 years); 7 patients had symptoms compatible with gastroesophageal reflux (GER), 5 with pathological GER diagnosed by 24-h esophageal pH testing, and 6 patients had impaired esophageal motility diagnosed by high-resolution esophageal manometry, most frequently ineffective peristalsis. Although further studies are required for confirmation, we conclude that CC may be a characteristic prodrome of CANVAS and may be related to GER and esophageal disorders. Furthermore, CC affects patients’ QoL, especially in the psychosocial sphere.
Similar content being viewed by others


Introduction
Cerebellar ataxia with neuropathy and bilateral vestibular areflexia syndrome (CANVAS) is a rare neurological disorder of autosomal recessive inheritance. In 2019, for the first time, the underlying genetic basis of this syndrome was described as biallelic expansion of the AAGG repeat motif (AAGGGexp) in intron 2 of replication factor C subunit 1 (RFC1) [1]. It has recently been reported that, exceptionally, CANVAS may also be due to AAGGGexp expansion and a truncating variant in compound heterozygosity in the RFC1 gene [2,3,4].
CANVAS is clinically characterized by combined adult-onset progressive ataxia, sensory neuropathy, and bilateral vestibular areflexia [5,6,7]. Also reported is a high prevalence (30–97%) of chronic cough (CC) [1, 8,9,10,11], which appears to precede the onset of neurological symptoms by decades (12–30 years) [12,13,14]. In fact, recent studies suggest that CC is a CANVAS-associated symptom that should guide CANVAS diagnosis if associated with at least 2 components of the main triad (cerebellar ataxia, neuronopathy, and vestibular areflexia) [10, 15], and also that CC should even be included as a symptom of CANVAS itself [13]. It has been recommended that patients with CANVAS be followed up by a multidisciplinary team that includes not only a neurologist, but also a pulmonologist and a gastroenterologist [14]. However, to our knowledge, no pathological studies on respiratory tissue in CANVAS cases.
As is the case for other neurological diseases such as Holmes-Adie syndrome [16] and type 1B sensory neuropathy [17], the mechanism underlying CC in CANVAS is currently unknown. CC is hypothesized to possibly be caused by impaired sensory innervation of upper respiratory tract or esophageal C fibres, resulting in their hypersensitivity [10, 13, 18]. The complex neurological mechanism behind CC involves a reflex arc made up of a peripheral and a central circuit.
The peripheral circuit is made up of afferent nerves, which activate or inhibit the cough mechanism through polymodal receptors, and efferent nerves, which activate the muscles involved in coughing. Subtypes of the afferent sensory nerves, part of the vagus nerve (10th cranial nerve), are the C fibres and A-delta fibres. C fibres are unmyelinated, have their cell bodies in the jugular ganglion, and are responsible for activating and inhibiting the cough reflex, while A-delta fibres are myelinated, have their cell bodies in the nodose ganglion, and are mostly responsible for activating the cough reflex [10, 19,20,21]. While peripheral terminations are believed to reside predominantly in the major airways (larynx, trachea, and large bronchi), terminations in the lung parenchyma cannot be ruled out, as several parenchymal lung diseases present with chronic cough [22]. Noxious stimuli, e.g., gastric fluid and cigarette smoke, are detected via receptors and ion channels (e.g., TRPV1 and P2X3) located in airway vagal afferent nerve endings [23]. Most C fibres are activated by irritant stimuli of inflammatory origin, while A-delta fibres are typically activated by mechanical and acidic stimuli [24]. As for the central circuit, this is made up of different regions such as the sensory cortical areas and the cingulate, insular, and orbitofrontal cortex [22]. Cough hypersensitivity, i.e., a coughing response to stimuli that do not usually produce cough, may be due to both peripheral and central mechanisms.
In the case of CANVAS, it is thought that AAGGGexp in intron 2 of RFC1 may cause CC by damaging vulnerable tissues like the C and A-delta fibres [21]. This nerve fibre damage may provoke an early change in esophageal motility that may lead to gastroesophageal reflux (GER) and consequently may cause CC—a hypothesis that may be supported by several studies that document GER in patients with CANVAS [10, 13, 14, 25].
Bearing in mind the possible link between CC and CANVAS, to our knowledge no protocolized study applying European Respiratory Society (ERS) recommendations has been conducted by a multidisciplinary team that includes pulmonologists specializing in CC that has evaluated possible alterations and causes associated with CC and the impact on quality of life (QoL) in patients with CANVAS. Regarding a possible relationship between CT and CANVAS, Guilleminault et al. [26], in a recent study of the prevalence of repeat expansions of RFC1 in patients with refractory CT, found that 16.2% (n = 11) and 8.8% (n = 6) of their patients had a biallelic mutation and a monoallelic mutation in RFC1, respectively.
Our aim was, as a multidisciplinary team composed of neurologists, pulmonologists, gastroenterologists, and geneticists, to identify clinical and functional characteristics of CC and its impact on QoL in patients with CANVAS.
Materials and methods
Study design and population
Our cross-sectional descriptive study included 10 male and female patients with CANVAS and experiencing CC, defined as a cough lasting > 8 weeks. The patients were referred to a specialist CC clinic from the neuromuscular disease unit of a Spanish tertiary hospital where they were being followed up for CANVAS, defined as the presence of the classical triad of cerebellar ataxia, neuronopathy, and vestibular areflexia, genetically confirmed by the biallelic expansion of AAGGG in RFC1. Exclusion criteria were age < 30 years and > 90 years, tobacco use, and angiotensin-converting enzyme inhibitor (ACEI) use, except when smoking was given up or ACEI use was withdrawn, respectively, and provided CC persisted.
Methodology
Sociodemographic, clinical, and functional variables were collected for the 10 patients included in our CC study, which applied the ERS [23] protocol: chest X-ray and/or chest computed tomography (CT), spirometry with bronchodilator test (BDT), fraction of exhaled nitric oxide (FENO), prick test, total blood immunoglobulin E (IgE) count, absolute peripheral eosinophil count, 24-h esophageal pH test (24-h pH), and high-resolution esophageal manometry (HREM). CC impact was assessed using the following instruments: Cough Severity Diary (CSD) [27], Leicester Cough Questionnaire (LCQ) [28, 29], Discrete Emotions Questionnaire (DEQ) [30], and European Quality of Life-5 Dimensions-5 Levels (EQ-5D-5L) [31,32,33].
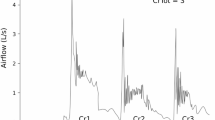
Spirometry with BDT was performed using the Datospir-600 device (Sibelmed SA, Barcelona, Spain) by an experienced technician and following American Thoracic Society/ERS (ATS/ERS) recommendations [34]. FENO was measured, applying ATS/ERS recommendations [35] and reference values from the literature [36], using electrochemical equipment (N-6008® SIR chemiluminescence sensor, Madrid, Spain) with precision ± 1%, a reading range of 0–500 parts per billion (ppb), and automatic results analysis. The prick test, based on the most prevalent standardized allergen extracts for our setting [37], was considered positive when the resulting papule was > 3 mm. Total blood IgE, determined using the enzyme-linked immunosorbent assay (ELISA) (UNICAP, Pharmacia, Uppsala, Sweden), was considered elevated for values > 160 IU/mL. 24-h pH was measured with a Digitrapper™ Recorder (Medtronic, Minneapolis, USA), using a 1-electrode probe placed 5 cm from the upper margin of the lower esophageal sphincter (LES) or a pH-impedance testing probe (pH-Z); the data were analysed using Reflux Software™ version 6.1 (Medtronic, Minneapolis, USA), and results were interpreted following Lyon Consensus recommendations [38]. Data for HREM, performed with the ManoScan™ system (Medtronic, Minneapolis, USA), were analysed using ManoView™ ESO version 3.3 software (Medtronic, Minneapolis, USA), and the findings were interpreted according to the Chicago Classification version 4.0 [39].
Genetic study of biallelic AAGGG expansion in replication factor C subunit 1 (RFC1)
The patients’ DNA samples were analysed using 2 genetic techniques: (1) amplification by standard polymerase chain reaction (PCR) with primers flanking the intron 2 fragment of the RFC1 gene (flanking-PCR)—a technique that only allows alleles of normal size to be amplified (i.e., not those containing large expansions, irrespective of their composition); and (2) amplification by triplet repeat primed PCR in 3 independent reactions: RP-PCR1 to detect the (AAAAG)11 and (AAAAG)exp alleles; RP-PCR2 to detect the (AAAGG)exp allele; and RP-PCR3 to detect the pathological (AAGGG)exp allele. The reference sequence used was NM_002913.4.
Chronic cough-related quality of life in patients with CANVAS
CC-related QoL was investigated via responses to 3 hard-copy self-administered questionnaires, as follows:
-
1.
CSD [27], designed to quantify cough severity in the previous 24 h, consists of 7 questions assessing frequency, intensity, and disruption, responded to on a Likert scale (0 = best possible score, 10 = worst possible score). The total score is obtained by summing and averaging the scores for the 3 domains, resulting in maximum and minimum possible scores of 10 and 0, respectively.
-
2.
LCQ [28, 29], designed to assess the impact of coughing in the physical, psychological, and social domains in the previous 2 weeks, consists of 19 questions, responded to on a Likert scale (1 = worst possible score, 7 = best possible score). The total score is obtained by summing the scores for the 3 domains, resulting in maximum and minimum possible scores of 3 and 21, respectively.
-
3.
DEQ [30], created to determine the impact of coughing on 32 emotions classified in 8 different emotional states (anger, disgust, fear, anxiety, sadness, desire, relaxation, and happiness). Each item is scored separately on a Likert scale (1 = worst possible score, 7 = best possible score).
In addition to these cough-specific questionnaires, health-related QoL was assessed using the EQ-5D-5L, which consists of 2 parts. For the first part, containing 5 health status questions with 5 responses reflecting different levels of severity, a specific reference value is subtracted depending on the target population (in our case, the Spanish population) [32]. Scores range from < 0 to 1, where 0 is equivalent to death, negative values reflect a status perceived to be worse than death, and 1 reflects full health [33]. The second part consists of a visual analogue scale (VAS), where 0 and 100 reflect the worst and best imaginable health states, respectively [31].
Ethical and legal aspects
The study complied with the principles of the Declaration of Helsinki (18th World Medical Assembly, 1964) and was approved by the Hospital Santa Creu i Sant Pau Clinical Research Ethics Committee (Barcelona). Patients provided their informed written consent prior to participation in the study and all study data were anonymized. The clinicaltrials.gov identifier is NCT04703595.
Results
Patient clinical and functional characteristics
The CC study was performed in 10 patients with CANVAS (5 men and 5 women) who met all the inclusion criteria and none of the exclusion criteria. Mean age was 64.8 ± 8.6 years and mean body mass index (BMI) was 24.4 ± 3.2 kg/m2. The most frequent comorbidities were clinical GER (70%, n = 7), rhinitis (50%, n = 5), depression (50%, n = 5), and nocturnal sleep apnea (confirmed and undergoing study due to clinical suspicion in 40% (n = 4) and 30% (n = 3), respectively).
All patients reported dry-type CC (100%), with a mean duration of 30.4 ± 8.7 years, a mean onset of 34.4 ± 9.9 years previously, and a mean of 14.2 ± 7.9 years before the onset of neurological symptoms consistent with CANVAS. Coughing tended to worsen with strong odours (60%, n = 6), speech (60%, n = 6), eating (50%, n = 5), and stress (50%, n = 5). Dyspnea (50%, n = 5) and urinary incontinence (40%, n = 4) were also frequently associated with coughing attacks.
In most patients (70%, n = 7), CC had been studied prior to the CANVAS diagnosis by pulmonologists (40%, n = 4), otorhinolaryngologists (30%, n = 3), or gastroenterologists (30%, n = 3). However, no cause was identified for 4 of the patients, and treatment failed for 3 patients for whom a possible cause was identified. Follow-up was lost in 71.4% (n = 5) of those CC cases.
Possible causes of chronic cough
Table 1 reports the full CC study results for the 10 patients with CANVAS. A single patient (#10) presented significant radiological and spirometry abnormalities, leading to a diagnosis of pleuro-parenchymal fibroelastosis. Notable at the lung function level was that 2 patients (#2 and #3) with spirometry in the normal range had a positive BDT. Only patient #3 showed partial improvement in response to the BDT, and this same patient also had associated peripheral eosinophilia and a positive prick test for dust mites and pollens, all compatible with a diagnosis of asthma.
Over half the patients (#2, #3, #4, #5, #7, and #9) showed some degree of esophageal motility impairment, ranging from ≥ 50% of ineffective sequences (patient #7) to failed sequences (patient #4). The most frequent alteration was ineffective esophageal motility without contraction reserve (patients #2, #3, and #9). In patients #2, #4, and #8, 24-h pH testing indicated pathological GER, although none of these patients indicated that the GER was related to coughing symptoms during testing.
Chronic cough impact on quality of life
Table 2 reports results for CC impact on QoL in the 10 patients with CANVAS. The mean total CSD score was 3.3 ± 1.9, and the impact was greater for the frequency (3.47 ± 2.2) and intensity (2.85 ± 1.9) domains than for the disruption domain. The mean total LCQ score was 13.1 ± 0.2, with a greater impact in the psychological domain (3.6 ± 1.1), followed by the social domain (4.4 ± 1.5) and the physical domain (5.1 ± 1.3). The DEQ domains most affected by CC were anxiety (3.2 ± 1.6) and anger (2.9 ± 1.8). As for the EQ-5D-5L, the mean health-related score was 0.8 ± 0.1 and the mean VAS score was 62 ± 12.5.
Discussion
The main characteristics of CC in our patients with genetically confirmed CANVAS were that the cough was dry, appeared several years before the neurological symptoms of CANVAS, especially affected psychosocial QoL, and was mainly associated with pathological GER and esophageal motility abnormalities.
The fact that the CC was dry is a finding consistent with previous studies reporting dry spasmodic cough in a high percentage (50–60%) of patients with CANVAS [8, 12, 14, 39]. It has also been documented that coughing worsens in response to stimuli that do not normally produce cough, such as speech and stress [12, 13]. This worsening of the cough in response to stimuli that should not provoke cough may be compatible with cough hypersensitivity syndrome, a hypothesized cause of CC in patients with CANVAS that results from impaired nervous regulation of the cough reflex arc caused by innocuous irritants [10, 13, 18].
The questionnaires pointed to a negative impact of CC on the QoL of our patients with CANVAS, corroborating previous studies reporting an association between CC and impaired QoL [41,42,43,44,45,46,47]; note, however, that to date, the specific impact on patients with CANVAS has not been documented. The fact that the psychosocial domain was most affected by CC (4.4 ± 1.5 and 5.1 ± 1.3 for the LCQ psychological and social domains, respectively) corroborates a prospective study by French et al. [41] performed on 39 patients with CC of any etiology. Anxiety and anger were the most prevalent emotions (3.2 ± 1.6 and 2.9 ± 1.8 for DEQ anxiety and anger, respectively), corroborating a study by Ueda et al. [44] of 21 patients with refractory or unexplained CC. The fact that health-related QoL in our patients was also diminished by CC (EQ-5D-5L 0.8 ± 0.1) largely corroborates the cross-sectional studies by Won et al. [45], based on analysis of the Korean National Health and Nutrition Examination Survey 2010–2016 database, and by Kubo et al. [46], based on surveys of 1136 patients, half with CC and the other half without CC.
Regarding the complementary tests, notable were the findings of compatibility with asthma (20%) and GER (50%), corroborating results for other series of patients [10, 11, 13, 14]. However, treatment did not completely resolve coughing in our patients, while pathological GER episodes detected by 24-h pH testing were not related to cough but to episodes of heartburn. The fact that the CC remained unresolved despite suitable study and targeted treatment would suggest that refractory CC is a characteristic and persistent pneumological symptom in patients with CANVAS. For this reason, it is important to study CC in all patients with CANVAS, since targeted treatment may reduce intensity and frequency, and may even throw light on future targeted treatments for refractory CC.
As a possible cause of CC, another pulmonary disease, namely, pleuro-parenchymal fibroelastosis, was detected by radiology in a single patient (10% of the included patients) and required specific respiratory monitoring. This finding would suggest that patients with CANVAS require a multidisciplinary approach that includes a protocolized CC study based on assessment by a CC specialist from within the pulmonology discipline.
The fact that CC developed, on average, 14.2 ± 7.9 years before the onset of any CANVAS symptom in our patients highlights the importance of early diagnosis of this progressive and disabling neurological disease, suggesting that CANVAS, as an hereditary autosomal recessive disease, would benefit from early genetic counselling. CC should also be properly included as a symptom of CANVAS [13], rather than only be taken into account when associated with 2 of the triad of symptoms (cerebellar ataxia, neuronopathy, and vestibular areflexia) [10, 15].
A study strength is, as far as we are aware, that this is the first multidisciplinary study of patients with CANVAS that has involved neurologists, geneticists, and gastroenterologists, as well as pulmonologists and CC specialists. An additional strength is that the study applied current ERS recommendations. The main limitation is the small sample of just 10 patients, explained by both the low prevalence of CANVAS and the lack of neurological tests to determine CC pathophysiology in patients with CANVAS and to study the cough reflex arc. Precise data on CANVAS prevalence are unavailable, although prevalence is estimated to be < 1/1,000,000 in the general population [48].
Conclusion
Although further studies are required for confirmation, CC onset up to decades before the development of neurological symptoms points to CC as a key early diagnostic clue for CANVAS. The importance of a multidisciplinary CC study of patients with genetically confirmed CANVAS is underlined by the fact that these patients present with a dry cough several years before the emergence of neurological symptoms, and that, in most patients, this cough, which especially affects psychosocial QoL, appears to be related to pathological GER and impaired esophageal motility. A multidisciplinary team of specialists is also necessary to confirm or rule out possible alternative causes of CC (such as asthma, GER, or pulmonary fibrosis) and to develop and provide targeted treatment for CC.
References
Cortese A, Simone R, Sullivan R, Vandrovcova J, Tariq H, Yau WY, Humphrey J, Jaunmuktane Z, Sivakumar P, Polke J, Ilyas M, Tribollet E, Tomaselli PJ, Devigili G, Callegari I, Versino M, Salpietro V, Efthymiou S, Kaski D, Wood NW, Andrade NS, Buglo E, Rebelo A, Rossor AM, Bronstein A, Fratta P, Marques WJ, Züchner S, Reilly MM, Houlden H (2019) Biallelic expansion of an intronic repeat in RFC1 is a common cause of late-onset ataxia. Nat Genet 51(4):649–658
Benkirane M, Da Cunha D, Marelli C, Larrieu L, Renaud M, Varilh J, Pointaux M, Baux D, Ardouin O, Vangoethem C, Taulan M, Daumas Duport B, Bergougnoux A, Corbillé AG, Cossée M, Juntas Morales R, Tuffery-Giraud S, Koenig M, Isidor B, Vincent MC (2022) RFC1 nonsense and frameshift variants cause CANVAS: clues for an unsolved pathophysiology. Brain 145(11):3770–3775
Ronco R, Perini C, Currò R, Dominik N, Facchini S, Gennari A, Simone R, Stuart S, Nagy S, Vegezzi E, Quartesan I, El-Saddig A, Lavin T, Tucci A, Szymura A, Novis De Farias LE, Gary A, Delfeld M, Kandikatla P, Niu N, Tawde S, Shaw J, Polke J, Reilly MM, Wood NW, Crespan E, Gomez C, Chen JYH, Schmahmann JD, Gosal D, Houlden H, Das S, Cortese A (2023) Truncating variants in RFC1 in cerebellar ataxia, neuropathy, and vestibular areflexia syndrome. Neurology 100(5):e543–e554
Arteche-López A, Avila-Fernandez A, Damian A, Soengas-Gonda E, de la Fuente RP, Gómez PR, Merlo JG, Burgos LH, Fernández CC, Rosales JML, Martínez JFG, Quesada-Espinosa JF, Corton M, Guerrero-Molina MP (2023) New cerebellar ataxia, neuropathy, vestibular areflexia syndrome cases are caused by the presence of a nonsense variant in compound heterozygosity with the pathogenic repeat expansion in the RFC1 gene. Clin Genet 103(2):236–241
Szmulewicz DJ, Waterston JA, Halmagyi GM, Mossman S, Chancellor AM, McLean CA, Storey E (2011) Sensory neuropathy as part of the cerebellar ataxia neuropathy vestibular areflexia syndrome. Neurology 76(22):1903–1910
Szmulewicz DJ, Roberts L, McLean CA, MacDougall HG, Halmagyi GM, Storey E (2016) Proposed diagnostic criteria for cerebellar ataxia with neuropathy and vestibular areflexia syndrome (CANVAS). Neurol Clin Pract 6(1):61–68
Cortese A, Curro’ R, Vegezzi E, Yau WY, Houlden H, Reilly MM (2022) Cerebellar ataxia, neuropathy and vestibular areflexia syndrome (CANVAS): genetic and clinical aspects. Pract Neurol 22(1):14–18
Huin V, Coarelli G, Guemy C, Boluda S, Debs R, Mochel F, Stojkovic T, Grabli D, Maisonobe T, Gaymard B, Lenglet T, Tard C, Davion JB, Sablonnière B, Monin ML, Ewenczyk C, Viala K, Charles P, Le Ber I, Reilly MM, Houlden H, Cortese A, Seilhean D, Brice A, Durr A (2022) Motor neuron pathology in CANVAS due to RFC1 expansions. Brain 145(6):2121–2132
Cortese A, Tozza S, Yau WY, Rossi S, Beecroft SJ, Jaunmuktane Z, Dyer Z, Ravenscroft G, Lamont PJ, Mossman S, Chancellor A, Maisonobe T, Pereon Y, Cauquil C, Colnaghi S, Mallucci G, Curro R, Tomaselli PJ, Thomas-Black G, Sullivan R, Efthymiou S, Rossor AM, Laurá M, Pipis M, Horga A, Polke J, Kaski D, Horvath R, Chinnery PF, Marques W, Tassorelli C, Devigili G, Leonardis L, Wood NW, Bronstein A, Giunti P, Züchner S, Stojkovic T, Laing N, Roxburgh RH, Houlden H, Reilly MM (2020) Cerebellar ataxia, neuropathy, vestibular areflexia syndrome due to RFC1 repeat expansion. Brain 143(2):480–490
Dupré M, Hermann R, Froment Tilikete C (2021) Update on cerebellar ataxia with neuropathy and bilateral vestibular areflexia syndrome (CANVAS). Cerebellum 20(5):687–700
Currò R, Salvalaggio A, Tozza S, Gemelli C, Dominik N, Galassi Deforie V, Magrinelli F, Castellani F, Vegezzi E, Businaro P, Callegari I, Pichiecchio A, Cosentino G, Alfonsi E, Marchioni E, Colnaghi S, Gana S, Valente EM, Tassorelli C, Efthymiou S, Facchini S, Carr A, Laura M, Rossor AM, Manji H, Lunn MP, Pegoraro E, Santoro L, Grandis M, Bellone E, Beauchamp NJ, Hadjivassiliou M, Kaski D, Bronstein AM, Houlden H, Reilly MM, Mandich P, Schenone A, Manganelli F, Briani C, Cortese A (2021) RFC1 expansions are a common cause of idiopathic sensory neuropathy. Brain 144(5):1542–1550
Magy L, Chazelas P, Richard L, Deschamps N, Frachet S, Vallat JM, Magdelaine C, Favreau F, Bessaguet F, Lia AS, Duchesne M (2022) Early diagnosis in cerebellar ataxia, neuropathy, vestibular areflexia syndrome (CANVAS) by focusing on major clinical clues: beyond ataxia and vestibular impairment. Biomedicines 10(8):2046
Infante J, García A, Serrano-Cárdenas KM, González-Aguado R, Gazulla J, de Lucas EM, Berciano J (2018) Cerebellar ataxia, neuropathy, vestibular areflexia syndrome (CANVAS) with chronic cough and preserved muscle stretch reflexes: evidence for selective sparing of afferent Ia fibres. J Neurol 265(6):1454–1462
Cortese A, Reilly MM, Houlden H (2020) RFC1 CANVAS/spectrum disorder. In: Adam MP, Everman DB, Mirzaa GM, Pagon RA, Wallace SE, Bean LJH, Gripp KW, Amemiya A, editors. GeneReviews® [Internet]. University of Washington, Seattle; 1993–2023
Çakar A, Şahin E, Tezel S, Candayan A, Samancı B, Battaloğlu E, Başak AN, Bilgiç B, Hanağası H, Durmuş H, Parman Y (2022) Cerebellar ataxia, neuropathy and vestibular areflexia syndrome (canvas): an important cause of late-onset ataxia with unique clinical features. Acta Neurol Belg 122(4):939–945
Kimber J, Mitchell D, Mathias CJ (1998) Chronic cough in the Holmes-Adie syndrome: association in five cases with autonomic dysfunction. J Neurol Neurosurg Psychiatry 65(4):583–586
Spring PJ, Kok C, Nicholson GA, Ing AJ, Spies JM, Bassett ML, Cameron J, Kerlin P, Bowler S, Tuck R, Pollard JD (2005) Autosomal dominant hereditary sensory neuropathy with chronic cough and gastro-oesophageal reflux: clinical features in two families linked to chromosome 3p22-p24. Brain 128(Pt 12):2797–2810
Szmulewicz DJ, McLean CA, MacDougall HG, Roberts L, Storey E, Halmagyi GM (2014) CANVAS an update: clinical presentation, investigation and management. J Vestib Res 24(5–6):465–474
Pacheco A, de Diego A, Domingo C, Lamas A, Gutierrez R, Naberan K, Garrigues V, López Vime R (2015) Chronic cough. Arch Bronconeumol 51(11):579–589
Mazzone SB, Undem BJ (2016) Vagal afferent innervation of the airways in health and disease. Physiol Rev 96(3):975–1024
Canning BJ, Mazzone SB, Meeker SN, Mori N, Reynolds SM, Undem BJ (2004) Identification of the tracheal and laryngeal afferent neurones mediating cough in anaesthetized guinea-pigs. J Physiol 557(Pt 2):543–558
Chung KF, McGarvey L, Song WJ, Chang AB, Lai K, Canning BJ, Birring SS, Smith JA, Mazzone SB (2022) Cough hypersensitivity and chronic cough. Nat Rev Dis Prim 8(1):45
Morice AH, Millqvist E, Bieksiene K, Birring SS, Dicpinigaitis P, Domingo Ribas C, Hilton Boon M, Kantar A, Lai K, McGarvey L, Rigau D, Satia I, Smith J, Song WJ, Tonia T, van den Berg JWK, van Manen MJG, Zacharasiewicz A (2020) ERS guidelines on the diagnosis and treatment of chronic cough in adults and children. Eur Respir J 55(1):1901136
McAlexander MA, Myers AC, Undem BJ (1999) Adaptation of guinea-pig vagal airway afferent neurones to mechanical stimulation. J Physiol 521(Pt 1):239–247
Sánchez-Tejerina D, Alvarez PF, Laínez E, Martinez VG, Santa-Cruz DI, Verdaguer L, Gratacòs M, Seoane JL, Raguer N, Hernández-Vara J, Llauradó A, Sotoca J, Salvado M, Arumi EG, Tizzano EF, Juntas R (2023) RFC1 repeat expansions and cerebellar ataxia, neuropathy and vestibular areflexia syndrome: experience and perspectives from a neuromuscular disorders unit. J Neurol Sci 446:120565
Guilleminault L, Chazelas P, Melloni B, Magdelaine C, Villeneuve T, Brouquières D, Lia AS, Magy L (2023) Repeat expansions of RFC1 in refractory chronic cough: a missing piece of the puzzle? Chest 163(4):911–915
Vernon M, Kline Leidy N, Nacson A, Nelsen L (2010) Measuring cough severity: development and pilot testing of a new seven-item cough severity patient-reported outcome measure. Ther Adv Respir Dis 4(4):199–208
Birring SS, Prudon B, Carr AJ, Singh SJ, Morgan MD, Pavord ID (2003) Development of a symptom specific health status measure for patients with chronic cough: Leicester Cough Questionnaire (LCQ). Thorax 58(4):339–343
Muñoz G, Buxó M, de Gracia J, Olveira C, Martinez-Garcia MA, Giron R, Polverino E, Alvarez A, Birring SS, Vendrell M (2016) Validation of a Spanish version of the Leicester Cough Questionnaire in non-cystic fibrosis bronchiectasis. Chron Respir Dis 13(2):128–136
Harmon-Jones C, Bastian B, Harmon-Jones E (2016) The discrete emotions questionnaire: a new tool for measuring state self-reported emotions. PLoS ONE 11(8):e0159915
Herdman M, Gudex C, Lloyd A, Janssen M, Kind P, Parkin D, Bonsel G, Badia X (2011) Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res 20(10):1727–1736
Ramos-Goñi JM, Pinto Prades JL, Oppe M, Cabasés Hita JM, Rivero-Arias O (2010) Estimación del conjunto de valores para los estados de salud del EQ-5D-5L basados en las preferencias de la población española. Plan de Calidad para el Sistema Nacional de Salud del Ministerio de Sanidad, Política Social e Igualdad. Servicio de Evaluación del Servicio Canario de la Salud; 2014. Informes de Evaluación de Tecnologías Sanitarias: SESCS Nº 2010/05
EuroQol Research Foundation (2019) EQ-5D-5L UserGuide. https://euroqol.org/publications/user-guides. Accessed 11 Aug 2022
Miller MR, Crapo R, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, Enright P, van der Grinten CP, Gustafsson P, Jensen R, Johnson DC, MacIntyre N, McKay R, Navajas D, Pedersen OF, Pellegrino R, Viegi G, Wanger J (2005) ATS/ERS Task Force. General considerations for lung function testing. Eur Respir J 1:153–161
American Thoracic Society, European Respiratory Society (2005) ATS/ERS recommendations for standardized procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide, 2005. Am J Respir Crit Care Med 171:912–930
Fortuna AM, Feixas T, Casan P (2007) Measurement of fraction of exhaled nitric oxide with the portable NIOX-MINO monitor in healthy adults. Arch Bronconeumol 43(3):176–179
(1988) Report on skin test standardization. The Committee on Skin Test Standardization of The Netherlands Society of Allergology. Clin Allergy 18(3):305–310
Gyawali CP, Kahrilas PJ, Savarino E, Zerbib F, Mion F, Smout AJPM, Vaezi M, Sifrim D, Fox MR, Vela MF, Tutuian R, Tack J, Bredenoord AJ, Pandolfino J, Roman S (2018) Modern diagnosis of GERD: the Lyon Consensus. Gut 67(7):1351–1362
Yadlapati R, Kahrilas PJ, Fox MR, Bredenoord AJ, Prakash Gyawali C, Roman S, Babaei A, Mittal RK, Rommel N, Savarino E, Sifrim D, Smout A, Vaezi MF, Zerbib F, Akiyama J, Bhatia S, Bor S, Carlson DA, Chen JW, Cisternas D, Cock C, Coss-Adame E, de Bortoli N, Defilippi C, Fass R, Ghoshal UC, Gonlachanvit S, Hani A, Hebbard GS, Wook Jung K, Katz P, Katzka DA, Khan A, Kohn GP, Lazarescu A, Lengliner J, Mittal SK, Omari T, Park MI, Penagini R, Pohl D, Richter JE, Serra J, Sweis R, Tack J, Tatum RP, Tutuian R, Vela MF, Wong RK, Wu JC, Xiao Y, Pandolfino JE (2021) Esophageal motility disorders on high-resolution manometry: Chicago classification version 4.0©. Neurogastroenterol Motil 33(1):e14058.
Dominik N, Galassi Deforie V, Cortese A, Houlden H (2021) CANVAS: a late onset ataxia due to biallelic intronic AAGGG expansions. J Neurol 268(3):1119–1126
French CL, Irwin RS, Curley FJ, Krikorian CJ (1998) Impact of chronic cough on quality of life. Arch Intern Med 158(15):1657–1661
Emilsson ÖI (2022) The burden and impact of chronic cough in severe disease. Curr Opin Support Palliat Care 16(4):183–187
Won HK, Song WJ (2021) Impact and disease burden of chronic cough. Asia Pac Allergy 11(2):e22
Ueda N, Yakushiji A, Schelfhout J, Tokita S, Kubo T (2022) Impact of refractory and unexplained chronic cough on disease burden: a qualitative study. BMC Pulm Med 22(1):372
Won HK, Lee JH, An J, Sohn KH, Kang MG, Kang SY, Morice AH, Cho SH, Song WJ (2020) Impact of chronic cough on health-related quality of life in the Korean adult general population: the Korean National Health and Nutrition Examination Survey 2010–2016. Allergy Asthma Immunol Res 12:964–979
Kubo T, Tobe K, Okuyama K, Kikuchi M, Chen Y, Schelfhout J, Abe M, Tokita S (2021) Disease burden and quality of life of patients with chronic cough in Japan: a population-based cross-sectional survey. BMJ Open Respir Res 8:e000764
Chamberlain SA, Garrod R, Douiri A, Masefield S, Powell P, Bücher C, Pandyan A, Morice AH, Birring SS (2015) The impact of chronic cough: a cross-sectional European survey. Lung 193(3):401–408
Orphanet (2023) The portal for rare diseases and orphan drugs: cerebellar ataxia with neuropathy and bilateral vestibular areflexia syndrome. https://www.orpha.net/consor/cgi-bin/OC_Exp.php?lng=EN&Expert=504476. Accessed 7 Sept 2023
Funding
Open Access Funding provided by Universitat Autonoma de Barcelona. This research was supported by a grant from the Spanish Society of Pulmonology and Thoracic Surgery (SEPAR) and the Catalan Society of Pulmonology (SOCAP). LGQ and PG were supported in this research by Instituto de Salud Carlos III and co-funded by EDRF/FEDER, ‘Una manera de hacer Europa’ under grant ACCI ER21P1AC705 from CIBERER. ASC was supported by grant FPU20/06692 from the Spanish Ministry of Universities.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
EP has received conference travel and attendance expenses from Gebro Pharma, Chiesi, FAES Farma, Rovi, GlaxoSmithKline, AstraZeneca, and Sanofi, and funds/grants for research projects from state agencies, non-profit foundations, and Alpha Bioresearch. ECS reports non-financial support from ALK, AstraZeneca, Novartis, and Menarini, personal fees from Boehringer-Ingelheim and TEVA, and personal fees/non-financial support from Chiesi outside the submitted work. VP in the last three years received honoraria for speaking at sponsored meetings from Astrazeneca, Boehringer-Ingelheim, Chiesi, Gebro, GSK, Luminova-Medwell and Sanofi. Received help assistance to meeting travel from Astrazeneca and Chiesi. Act as a consultant for Astrazeneca, Chiesi, GSK and Menarini. LGQ has received conference travel and attendance expenses and fees for talks at meetings sponsored by PTC Therapeutics, and has received funds/grants for research projects from state agencies. PG, LQ, FB, MR and ASC declare that they have no conflicts of interest. AC has received fees in the last 3 years for talks at meetings sponsored by AstraZeneca, Zambón, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, MSD, Novartis, Orion Pharma, and Sanofi, conference travel and attendance expenses from Gebro, GlaxoSmithKline, and Novartis, and funds/grants for research projects from several state agencies, non-profit foundations, AstraZeneca, and GlaxoSmithKline.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Palones, E., Curto, E., Plaza, V. et al. Clinical and functional characteristics, possible causes, and impact of chronic cough in patients with cerebellar ataxia, neuropathy, and bilateral vestibular areflexia syndrome (CANVAS). J Neurol 271, 1204–1212 (2024). https://doi.org/10.1007/s00415-023-12001-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-023-12001-9