
Abstract
Background
Patients with ischemic stroke and diabetes are classified as extreme risk for secondary prevention, with much attention and specific management. However, the up-to-date information regarding the burden of diabetes in acute ischemic stroke (AIS) patients is lacking in China, and evidence for an association between diabetes and in-hospital outcomes after AIS remains controversial.
Methods
This quality improvement study was conducted at 1,476 participating hospitals in the Chinese Stroke Center Alliance between 2015 and 2019. Prevalence of diabetes was evaluated in the overall study population and different subgroups. The association between diabetes and in-hospital outcomes in AIS patients was analyzed by using multivariable logistic regression analysis and propensity score-matched analysis.
Results
Of 838,229 patients with AIS, 286,252 (34.2%) had diabetes/possible diabetes. The prevalence of diabetes/possible diabetes was higher in women than in men (37.6% versus 32.1%). Patients with diabetes/possible diabetes had higher rates of adverse in-hospital outcomes than those without. Multivariable analysis revealed a significant association between diabetes/possible diabetes and adverse in-hospital outcomes (all-cause mortality: odds ratio [OR], 1.30 [95% confidence interval [CI], 1.23–1.38]; major adverse cardiovascular events (MACEs): OR, 1.08 [95% CI, 1.06–1.10]) in AIS patients. The excess risk of in-hospital outcomes still remained in AIS patients with diabetes/possible diabetes after propensity score-matching analysis (all-cause mortality: OR, 1.26 [95% CI, 1.17–1.35]; MACEs: OR, 1.07 [95% CI, 1.05–1.10]).
Conclusion
Diabetes was highly prevalent among AIS patients in China and associated with worse in-hospital outcomes. Greater efforts to increase targeted approach to secondary prevention treatments of diabetes in AIS patients are warranted.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Stroke is the leading cause of death in China, accounting for approximately one-third of worldwide stroke-related death [1, 2]. Diabetes is a common comorbidity in stroke patients and is associated with adverse outcomes after stroke, particularly recurrent stroke and mortality [3,4,5,6]. Patients with ischemic stroke and diabetes are classified as extreme risk for secondary prevention, with much attention and specific management according to algorithmic guidelines published by diabetes, endocrinology, and stroke associations [7]. However, in China the up-to-date information regarding the burden of diabetes in acute ischemic stroke (AIS) patients is lacking. The latest studies focusing on the prevalence of diabetes among Chinese AIS patients were conducted over 10 years ago [3, 5]. With the alarming increase in the prevalence of diabetes among the general population in China, it is necessary to re-evaluate the burden of diabetes among Chinese AIS patients.
Despite diabetes is an independent risk factor for the development of AIS, the evidence for an association between diabetes and in-hospital outcomes after AIS still remains controversial [4, 8,9,10,11]. Some studies have suggested that diabetes is an independently predictive factor for poor in-hospital outcomes after ischemic stroke [4, 8], but several studies have not [9,10,11]. The differences of results in previous studies on the relationship between diabetes and in-hospital outcomes of AIS patients could possibly be explained by inconsistent definition of diabetes or in-hospital outcomes, different confounding variables adjusted in multivariable analysis model, and different length of in-hospital stay of AIS inpatients [4, 8,9,10,11]. It is essential to perform further studies for clearly elucidating this issue among AIS patients.
The objective of this study therefore was to provide an updated estimation of the burden of diabetes among AIS patients in China and to evaluate the association between diabetes and in-hospital outcomes of AIS patients, using data from the Chinese Stroke Center Alliance (CSCA) program.
Materials and methods
Study design
The CSCA, launched in 2015, is a large, nationwide, multicenter, voluntary, multifaceted intervention, and continuous quality improvement initiative. Details of the design and methodology of the CSCA project have been published [12]. In brief, the study included 756 tertiary hospitals and 720 secondary hospitals from 31 provinces, autonomous regions, or municipalities in China. Data were collected by trained hospital personnel via the web-based patient data collection and management tool (Medicine Innovation Research Center, Beijing, China). The China National Clinical Research Center for Neurological Diseases served as the data analysis center. Institutional review board approval was granted for this program with a waiver for informed consent by the Ethics Committee of Beijing Tiantan Hospital. The CSCA study was performed according to the principles expressed in the Declaration of Helsinki.
Study population
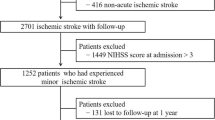
The CSCA consecutively enrolled patients aged over 18 years having a primary diagnosis of acute stroke or transient ischemic attack (TIA) confirmed by brain computed tomography or magnetic resonance imaging, including ischemic stroke, TIA, intracerebral hemorrhage, or subarachnoid hemorrhage within 7 days of symptom onset. A total of 1,006,798 inpatient with stroke or TIA were registered between August 2015 and July 2019 from 1,476 hospitals. More details can be found in previous report [13]. Of these, 838,229 AIS inpatients were included in the current study after excluding patients with TIA, hemorrhagic stroke, subarachnoid hemorrhage, or diagnosed as "undetermined". The flow chart of study population recruitment is presented in Supplementary Fig. S1.
Study variables
Definition of diabetes
Diabetes was defined as a self-reported history of diabetes, or use of hypoglycemic medications before hospitalization or at discharge, or glycated hemoglobin A1c (HbA1c) ≥ 6.5% (48 mmol/mol), or diabetes listed in the medical records as one of the discharge diagnoses.
Possible diabetes was defined as elevated level of fasting blood glucose (FBG, ≥ 7.0 mmol/L (126 mg/dL)) but without measurement of HbA1c, considering we were unable to distinguish this group of patients between undiagnosed diabetes and stress hyperglycemia only based on the results of FBG.
Definition of in‑hospital outcomes
The in-hospital outcomes investigated in this study referred to all-cause mortality and major adverse cardiovascular events (MACEs) during hospitalization. MACEs were defined as a combination of ischemic stroke, hemorrhagic stroke, TIA, and myocardial infarction (MI).
Statistical analysis
Consider that most inpatients with possible diabetes who may be undiagnosed or at high risk of developing diabetes also require the same in-hospital care as inpatients with diabetes [14, 15], we combined diabetes and possible diabetes for statistical analysis for the purposes of our study. We first assessed the prevalence of diabetes/possible diabetes among all AIS patients as well as in different subgroups by sex. The baseline characteristics, in-hospital treatments, and in-hospital outcomes were compared between patients with and without diabetes/possible diabetes. Continuous variables were described as mean (standard deviation [SD]) for normally distributed data. Categorical variables were presented as the number (percentage). Patients' characteristics, in-hospital treatments, and in-hospital outcomes were compared using absolute standardized difference (ASD), with an ASD ≥ 10% considered clinically significant [16]. We used logistic regression analyses to evaluate the association between diabetes/possible diabetes and in-hospital outcomes, after adjusting for potential confounders, including baseline characteristics, risk factors, medical history, in-hospital treatments, and stroke severity.
To account for missing values on National Institutes of Health Stroke Scale (NIHSS) score, multiple imputation with chained equations was performed by using 10 iterations to impute missing values of NIHSS score, and the risk of diabetes/possible diabetes was recalculated in model 3 adjusting the imputed NIHSS score. Meanwhile, sensitivity analysis excluding patients with stress hyperglycemia (FBG ≥ 7.0 mmol/L (126 mg/dL) but with HbA1c < 6.5% (48 mmol/mol)) was also performed, considering the elevated risk of adverse in-hospital outcomes among those patients.
Subgroup analyses, including age (< 75/ ≥ 75 years old), sex (men/women), hypertension (yes/no), and in-hospital NIHSS score (0–4/5–14/ ≥ 15), were conducted using multivariable logistic regression model. The odds ratios (ORs) between the analyzed subgroups were compared by a Z-test.
Furthermore, propensity score-matched analysis was conducted to confirm the association between diabetes/possible diabetes and in-hospital outcomes. We calculated propensity scores of having diabetes/possible diabetes by logistic regression analysis involving the following factors: age, sex, body mass index (BMI), hypertension, dyslipidemia, current smoking, drinking, history of stroke/TIA, history of MI, history of atrial fibrillation, history of heart failure, history of carotid stenosis, history of peripheral artery disease, history of liver/renal dysfunction, in-hospital NIHSS score, insurance and hospital location. Patients with and without diabetes/possible diabetes were then paired at 1:1 according to the propensity scores using nearest-neighbor matching without replacement, with a caliper size of 0.02. The ASDs of variables were compared before and after propensity score matching (Supplementary Fig. S2), with ASD < 10% for the variables being considered successful balancing between groups. The baseline characteristics and in-hospital treatments between groups were re-compared after propensity score matching.
Statistical analyses were performed using SAS 9.4 (SAS Institute, Cary, NC, USA). Two-tailed P values of < 0.05 were considered statistically significant. Descriptive tables were produced by an SAS macro (%ggBaseline) that can automatically generate baseline tables [17].
Results
Diabetes prevalence in AIS patients
Among 838,229 patients with AIS who were included in this study, 524,351 (62.6%) were men and 313,878 (37.4%) were women, with an average age of 66.2 (± 12.0) years. Of these patients, a total of 286,252 (34.2%) had diabetes/possible diabetes (Table 1), including 33.4% diabetes and 0.7% possible diabetes. Female patients had a higher prevalence of diabetes/possible diabetes than male patients (37.6% versus 32.1%). Diabetes/possible diabetes was most common among patients aged 55–64 years (men: 34.6%; women: 41.6%). The prevalence of diabetes/possible diabetes increased with BMI. Patients with a history of stroke/TIA had a higher proportion of diabetes/possible diabetes than those without history of stroke/TIA (38.2% versus 32.3%).
Characteristics of AIS patients with/without diabetes
The demographics and clinical characteristics of included patients are summarized in Table 2. Compared with AIS patients without diabetes, patients with diabetes/possible diabetes were more likely to have an increased BMI (24.5 ± 5.0 versus 23.7 ± 4.0, ASD = 17.7) and a higher proportion of hypertension (91.0% versus 85.7%, ASD = 16.6), dyslipidemia (18.8% versus 11.7%, ASD = 19.8), and a history of stroke/TIA (35.1% versus 29.5%, ASD = 12.0). The severity of stroke (expressed as NIHSS score) showed similar results in AIS patients with and without diabetes/possible diabetes.
In‑hospital treatments of AIS patients with/without diabetes
The in-hospital treatments were compared between AIS patients with and without diabetes/possible diabetes (Table 3). There were no significant differences between two groups among in-hospital treatments, including IV-rtPA administration ≤ 4.5 h, antiplatelet therapy, anticoagulant therapy, and statins. Longer length of hospital stay was observed in patients with diabetes/possible diabetes than those without diabetes in this study (12.1 ± 7.1 versus 11.4 ± 6.6, ASD = 10.2).
Association between diabetes and in‑hospital outcomes
We compared the in-hospital outcomes between AIS patients with and without diabetes/possible diabetes (Supplementary Table S1). Higher rates of in-hospital outcomes were observed in AIS patients with diabetes/possible diabetes than those without diabetes, including all-cause mortality (0.8% versus 0.5%) and MACEs (7.7% versus 6.1%). In univariate logistic regression analysis, we observed significantly higher risk of in-hospital all-cause mortality and MACEs in AIS patients with diabetes/possible diabetes (Table 4, Supplementary Table S2). After adjusting for patients' demographic characteristics, medical history, in-hospital treatments, and other confounding factors, diabetes/possible diabetes was associated with excess risk of in-hospital all-cause mortality (odds ratio [OR], 1.38 [95% CI 1.30–1.46]) and MACEs (OR, 1.09 [95% CI 1.07–1.12]). After further adjusting in-hospital NIHSS score, the higher risk of in-hospital all-cause mortality (OR, 1.33 [95% CI 1.24–1.42]) and MACEs (OR, 1.08 [95% CI 1.06–1.10]) were still statistically significant in patients with diabetes/possible diabetes. Moreover, after multiple imputation with chained equations being used to impute missing value of NIHSS score, the significant association between diabetes/possible diabetes and in-hospital outcomes (all-cause mortality: OR, 1.30 [95% CI 1.23–1.38]; MACE: OR, 1.08 [95% CI 1.06–1.10]) still remained in AIS patients after multivariable adjustment (Table 4).
Sensitivity analysis was also performed to evaluate the association between diabetes/possible diabetes and in-hospital outcomes (Supplementary Table S3, Supplementary Table S4). After excluding patients with possible stress hyperglycemia (n = 33,706) in patients without diabetes, diabetes/possible diabetes was still significant associated with higher risk of in-hospital outcomes, including all-cause mortality (OR, 1.48 [95% CI 1.39–1.58]) and MACEs (OR, 1.09 [95% CI 1.07–1.11]) (Supplementary Table S3). Even excluding in-hospital TIA from MACEs, the higher risk of MACEs still remained in patients with diabetes/possible diabetes than those without diabetes (Supplementary Table S4).
In further subgroup analyses using multivariable logistic regression, higher risks of in-hospital all-cause mortality and MACEs were observed in patients with diabetes/possible diabetes in all subgroups (Fig. 1a,b).

Subgroup analysis for the association between diabetes/possible diabetes and in-hospital outcomes in AIS patients. a Association between diabetes/possible diabetes and in-hospital all-cause mortality. b Association between diabetes/possible diabetes and in-hospital MACEs. OR odds ratio, CI confidence interval, MACEs major adverse cardiovascular events, NIHSS national institutes of health stroke scale
Propensity score-matching analysis
In propensity score matching, 221,431 AIS patients with diabetes/possible diabetes were matched with 221,431 patients without diabetes. After matching, the ASD were all less than 10.0% for the variables included in the calculation of propensity score, suggesting that AIS patients with and without diabetes/possible diabetes were well matched (Supplementary Fig. S2). The baseline characteristics and in-hospital treatments between groups were re-compared (Supplementary Table S5). The rates of in-hospital outcomes still remained higher in patients with diabetes/possible diabetes than those without diabetes (all-cause mortality: 0.8% versus 0.6%; MACEs: 7.4% versus 6.9%) (Supplementary Table S1), and patients with diabetes/possible diabetes had higher risks of in-hospital all-cause mortality (OR, 1.26 [95% CI 1.17–1.35]) and MACEs (OR, 1.07 [95% CI 1.05–1.10]) than those without diabetes (Supplementary Table S6). After excluding in-hospital TIA from MACEs, the higher risk of MACEs still remained in diabetic/possible diabetic patients than in non-diabetic patients (Supplementary Table S4).
Discussion
To the best of our knowledge, the present study is the largest contemporary registry study to provide an updated estimation of the burden of diabetes among AIS patients in China and evaluate the association between diabetes and in-hospital outcomes after AIS. Our findings are of great significance in pointing out the future direction for improving secondary prevention strategies of AIS in China.
High diabetes prevalence among AIS patients in China
In this study, we found that diabetes/possible diabetes was highly prevalent in AIS patients across China, with 1 in 3 AIS patients had diabetes/possible diabetes.
The prevalence of diabetes in our study is higher than that in previous reports [5, 18,19,20], which may reflect the increasing prevalence of diabetes among AIS patients in China. The China National Stroke Registry reported that 21.6% of AIS patients across China had diabetes from 2007–2008, and 20.7% of them from 2012–2013 [18]. Date from the China National Stroke Screening Survey from 2013 to 2015 showed that 21.5% of ischemic stroke patients had diabetes across China [19]. Moreover, in view of the alarming growth in the prevalence of diabetes among the general population in China [21, 22], the proportion of diabetes among Chinese AIS patients will be continuously increasing.
Furthermore, according to the Survey on Abnormal Glucose Regulation in Patients With Acute Stroke Across China (ACROSS-China) from 2008 to 2009, 23% of patients with AIS were diagnosed with diabetes by medical history, and notably 22.8% of these patients were newly diagnosed with diabetes by oral glucose tolerance test (OGTT) [3]. In this setting, the actual prevalence of diabetes in AIS patients may be even higher than the reported proportion of our study, as some patients with diabetes may not have been identified because in the routine clinical practice OGTT is not widely applied to detect diabetes among inpatients. The finding from ACROSS-China also showed that the proportion of impaired glucose regulation in AIS patients was 23.9%, indicating that about a quarter of AIS patients in China are in pre-diabetes [3]. These findings suggest that neurologists in China have to manage a large proportion of AIS patients with pre-diabetes/diabetes in their clinical practice. Therefore, the screening for diabetes should be included in the routine examination at admission as the first key step in neurologists' management strategies. Clinical guidelines have suggested that it was reasonable for all patients with stroke to have an assessment of diabetes at admission [14, 23]. It is time to attach importance to the professional training of neurologists toward diabetes education and care and strengthen multi-disciplinary cooperation between internists, endocrinologists, and neurologists in clinical practice.
Adverse impact of diabetes on in-hospital outcomes of AIS patients
Our study provided evidence of an association between diabetes and adverse in-hospital outcomes in AIS patients. We found that AIS patients with diabetes/possible diabetes had higher risks of in-hospital all-cause mortality and MACEs, especially stroke recurrence, than did without diabetes, in both multivariable logistic regression analysis and propensity-score matching analysis.
Consistent with previous studies [4, 5, 24], we observed higher crude rates of adverse in-hospital outcomes in AIS patients with diabetes/possible diabetes than those without diabetes. Notably, the rate of in-hospital adverse outcomes was lower in our study than that in previous studies conducted among Chinese AIS patients [5, 25]. These findings might indicate that the advancements in the management of ischemic stroke patients during the past two decades have improved the prognosis of patients with ischemic stroke but have not eliminated the risk gap between diabetic and non-diabetic patients. Similar to those in previous studies [4, 5], AIS patients with diabetes in the present study were more likely to be overweight, had a higher proportion of history of stroke/TIA and more comorbidities, including hypertension and dyslipidemia, than those without diabetes. In our study, in-hospital treatments for AIS were comparable between patients with and without diabetes. After adjusting for confounding variables, the excess risk of adverse in-hospital outcomes still remained in AIS patients with diabetes/possible diabetes, which was in line with previous findings [4, 8]. Therefore, all AIS patients with diabetes/possible diabetes should raise much attention in clinical practice. In particular, female AIS patients should be kept under special close supervision in light of their high prevalence of diabetes and high risk of poor prognosis [26]. However, there has been some studies regarding the association between diabetes and in-hospital outcomes after AIS showed that the adverse in-hospital outcomes after ischemic stroke were not increased in patients with diabetes [9,10,11]. Many factors could contribute to these differences, including type II error result from smaller samples of study, different treatment patterns between countries, ethnicity difference, population health, and other social determinants.
Moreover, patients with diabetes/possible diabetes were more likely to have a slightly longer hospital stay. These observations fit with previous studies that showed that diabetes resulted in longer length of stay which possibly meant the complex complications, severe clinical conditions, and difficulties in controlling the blood glucose during hospitalization [8, 24]. Also, some studies with longer follow-up periods in Chinese population have found significant associations between diabetes and poor clinical prognosis among AIS patients [5, 27]. Those findings highlight that early identification and treatment of diabetes is more than timely and much needed for improving the prognosis of AIS patients. Previous studies showed that the presence of a prior TIA was associated with a favorable outcome in ischemic stroke patients, suggesting a neuroprotective effect of TIA possibly by inducing a phenomenon of ischemic tolerance allowing better recovery from a subsequent ischemic stroke [28, 29]. However, some studies failed to confirm this [30]. The discrepancy of results may result from the difference in the type of stroke, inconsistent definition of study endpoint, and bias in the record of previous TIA. Future prospective studies with carefully design are need to explore the phenomenon of ischemic tolerance in AIS patients.
Nowadays, clinical guidelines have classified stroke patients with diabetes as a high-risk group, and management strategies for them have been specially issued by the national and international guidelines [7, 14, 31,32,33]. With much attention being paid to those patients, the heavy burden and excess risk of diabetes in AIS patients are expected to decrease in the near future.
Limitations
Several limitations need to be addressed. First, the data on OGTT were unavailable in our study, which might influence the evaluation of proportion of AIS patients with diabetes. However, OGTT was not routinely applied in the current clinical workup. Further studies that consider OGTT are warranted. Second, as this was a quality improvement study based on medical records, the information about physical activity, diabetes types and emerging cerebrovascular risk factors (e.g., sleep-related breathing disorders, drug abuse, oral contraceptive use and inflammatory markers) were not available, which future studies should take into consideration. Third, this study did not collect information on the specific time of FBG measurement during hospitalization, some patients with only elevated FBG could not be definitively diagnosed with diabetes. Nevertheless, the use of only FBG test indicated that neurologists do not pay enough attention to the diagnosis of diabetes in AIS patients. Fourth, the potential bias in diagnostic criteria between participating hospitals may underestimate the endpoints. However, we still found the adverse effects of diabetes on in-hospital outcomes for AIS patients. Finally, the CSCA is based on voluntary enrollment of hospitals and does not have an elaborately designed sampling mechanism. However, the large sample size improves the robustness and generalizability of this study.
Conclusions
Our results showed that diabetes was highly prevalent among AIS patients in China and independently associated with worse in-hospital outcomes, based on a nationwide representative registry study. These findings highlight the importance and necessity of early identification and timely management of diabetes in AIS patients, informing future priorities for improving secondary prevention of AIS patients in clinical practice in China.
Data availability
The datasets analyzed during the current study are not publicly available due to intellectual property rights, but are available from the corresponding author on reasonable request.
Abbreviations
- AIS:
-
Acute ischemic stroke
- ASD:
-
Absolute standardized difference
- BMI:
-
Body mass index
- CI:
-
Confidence interval
- DBP:
-
Diastolic blood pressure
- HbA1c:
-
Glycated hemoglobin A1c
- IQR:
-
Interquartile range
- IV rtPA:
-
Intravenous tissue plasminogen activator
- MACEs:
-
Major adverse cardiovascular events
- MI:
-
Myocardial infarction
- NIHSS:
-
National Institutes of Health Stroke Scale
- OGTT:
-
Oral glucose tolerance test
- OR:
-
Odds ratio
- SBP:
-
Systolic blood pressure
- SD:
-
Standard deviation
- TIA:
-
Transient ischemic attack
References
Zhou M, Wang H, Zeng X, Yin P, Zhu J, Chen W, Li X, Wang L, Wang L, Liu Y, Liu J, Zhang M, Qi J, Yu S, Afshin A, Gakidou E, Glenn S, Krish VS, Miller-Petrie MK, Mountjoy-Venning WC, Mullany EC, Redford SB, Liu H, Naghavi M, Hay SI, Wang L, Murray CJL, Liang X (2019) Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet 394:1145–1158
Global Burden of Disease Collaborative Network (2018) Global Burden of Disease Study 2017 (GBD 2017) Results. http://ghdx.healthdata.org/gbd-results-tool. Accessed 25 December 2021
Jia Q, Zheng H, Zhao X, Wang C, Liu G, Wang Y, Liu L, Li H, Zhong L, Wang Y, Investigators for the Survey on Abnormal Glucose Regulation in Patients With Acute Stroke Across China (2012) Abnormal glucose regulation in patients with acute stroke across China: prevalence and baseline patient characteristics. Stroke 43:650–657
Szlachetka WA, Pana TA, Tiamkao S, Clark AB, Kongbunkiat K, Sawanyawisuth K, Bettencourt-Silva JH, Kasemap N, Mamas MA, Myint PK (2020) Impact of diabetes on complications, long term mortality and recurrence in 608,890 hospitalised patients with stroke. Glob Heart 15:2
Jia Q, Zhao X, Wang C, Wang Y, Yan Y, Li H, Zhong L, Liu L, Zheng H, Zhou Y, Wang Y (2011) Diabetes and poor outcomes within 6 months after acute ischemic stroke: the China National Stroke Registry. Stroke 42:2758–2762
Luitse MJ, Biessels GJ, Rutten GE, Kappelle LJ (2012) Diabetes, hyperglycaemia, and acute ischaemic stroke. Lancet Neurol 11:261–271
Garber AJ, Handelsman Y, Grunberger G, Einhorn D, Abrahamson MJ, Barzilay JI, Blonde L, Bush MA, DeFronzo RA, Garber JR, Garvey WT, Hirsch IB, Jellinger PS, McGill JB, Mechanick JI, Perreault L, Rosenblit PD, Samson S, Umpierrez GE (2020) Consensus statement by the american association of clinical endocrinologists and american college of endocrinology on the comprehensive type 2 diabetes management algorithm - 2020 executive summary. Endocr Pract 26:107–139
Reeves MJ, Vaidya RS, Fonarow GC, Liang L, Smith EE, Matulonis R, Olson DM, Schwamm LH (2010) Quality of care and outcomes in patients with diabetes hospitalized with ischemic stroke: findings from Get With the Guidelines-Stroke. Stroke 41:e409-417
Cruz-Herranz A, Fuentes B, Martínez-Sánchez P, Ruiz-Ares G, Lara-Lara M, Sanz-Cuesta B, Díez-Tejedor E (2015) Is diabetes an independent risk factor for in-hospital complications after a stroke? J Diabetes 7:657–663
Snarska KK, Bachórzewska-Gajewska H, Kapica-Topczewska K, Drozdowski W, Chorąży M, Kułakowska A, Małyszko J (2017) Hyperglycemia and diabetes have different impacts on outcome of ischemic and hemorrhagic stroke. Archives of medical science : AMS 13:100–108
Lekoubou A, Clovis N, Dzudie A, Kengne AP (2017) Diagnosed diabetes mellitus and in-hospital stroke mortality in a major sub-Saharan African urban medical unit. Prim Care Diabetes 11:57–62
Wang Y, Li Z, Wang Y, Zhao X, Liu L, Yang X, Wang C, Gu H, Zhang F, Wang C, Xian Y, Wang DZ, Dong Q, Xu A, Zhao J (2018) Chinese Stroke Center Alliance: a national effort to improve healthcare quality for acute stroke and transient ischaemic attack: rationale, design and preliminary findings. Stroke Vasc Neurol 3:256–262
Gu HQ, Yang X, Wang CJ, Zhao XQ, Wang YL, Liu LP, Meng X, Jiang Y, Li H, Liu C, Wangqin R, Fonarow GC, Schwamm LH, Xian Y, Li ZX, Wang YJ (2021) Clinical Characteristics, Management, and In-Hospital Outcomes in Patients With Stroke or Transient Ischemic Attack in China. JAMA Network Open 4:e2120745
Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, Biller J, Brown M, Demaerschalk BM, Hoh B, Jauch EC, Kidwell CS, Leslie-Mazwi TM, Ovbiagele B, Scott PA, Sheth KN, Southerland AM, Summers DV, Tirschwell DL (2019) Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the american heart association/american stroke association. Stroke 50:e344–e418
Ali Abdelhamid Y, Kar P, Finnis ME, Phillips LK, Plummer MP, Shaw JE, Horowitz M, Deane AM (2016) Stress hyperglycaemia in critically ill patients and the subsequent risk of diabetes: a systematic review and meta-analysis. Crit Care 20:301
Austin PC (2009) Using the standardized difference to compare the prevalence of a binary variable between two groups in observational research. Commun Statist Simul Comput 38:1228–1234
Gu HQ, Li DJ, Liu C, Rao ZZ (2018) %ggBaseline: a SAS macro for analyzing and reporting baseline characteristics automatically in medical research. Ann Transl Med 6:326
Li Z, Wang C, Zhao X, Liu L, Wang C, Li H, Shen H, Liang L, Bettger J, Yang Q, Wang D, Wang A, Pan Y, Jiang Y, Yang X, Zhang C, Fonarow GC, Schwamm LH, Hu B, Peterson ED, Xian Y, Wang Y, Wang Y (2016) Substantial Progress Yet Significant Opportunity for Improvement in Stroke Care in China. Stroke 47:2843–2849
Guo J, Guan TJ, Wang LD, Chao BH (2021) The epidemiological characteristics and adherence to hypoglycemic agents of ischemic stroke patients with diabetes. Chin J Prev Med 55:952–957
Wang YJ, Li ZX, Gu HQ, Zhai Y, Jiang Y, Zhao XQ, Wang YL, Yang X, Wang CJ, Meng X, Li H, Liu LP, Jing J, Wu J, Xu AD, Dong Q, Wang D, Zhao JZ, China Stroke Statistics Writing Committee (2020) China Stroke Statistics 2019: A Report From the National Center for Healthcare Quality Management in Neurological Diseases, China National Clinical Research Center for Neurological Diseases, the Chinese Stroke Association, National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention and Institute for Global Neuroscience and Stroke Collaborations. Stroke Vasc Neurol 5:211–239
Ma RCW (2018) Epidemiology of diabetes and diabetic complications in China. Diabetologia 61:1249–1260
Chan JCN, Zhang Y, Ning G (2014) Diabetes in China: a societal solution for a personal challenge. Lancet Diabetes Endocrinol 2:969–979
Stroke prevention and treatment engineering committee of the national health and family planning commission (2015) Chinese guidelines for blood glucose management of stroke patients. Beijing, China
Tanaka R, Ueno Y, Miyamoto N, Yamashiro K, Tanaka Y, Shimura H, Hattori N, Urabe T (2013) Impact of diabetes and prediabetes on the short-term prognosis in patients with acute ischemic stroke. J Neurol Sci 332:45–50
Zhang XD, Chen YR, Ge L, Ge ZM, Zhang YH (2007) Features of stroke in Chinese diabetes patients: a hospital-based study. J Int Med Res 35:540–546
Arboix A, Milian M, Oliveres M, Garcia-Eroles L, Massons J (2006) Impact of female gender on prognosis in type 2 diabetic patients with ischemic stroke. Eur Neurol 56:6–1227
Jing J, Pan Y, Zhao X, Zheng H, Jia Q, Li H, Guan L, Liu L, Wang C, Meng X, He Y, Wang Y, Wang Y (2016) Prognosis of ischemic stroke with newly diagnosed diabetes mellitus according to hemoglobin A1c criteria in chinese population. Stroke 47:2038–2044
Arboix A, Cabeza N, Garcia-Eroles L, Massons J, Oliveres M, Targa C, Balcells M (2004) Relevance of transient ischemic attack to early neurological recovery after nonlacunar ischemic stroke. Cerebrovasc Dis 18:304–311
Kim JG, Choi H, Sohn SY, Kim DH, Lee SJ (2016) Transient ischemic attacks preceding acute lacunar infarction. Eur Neurol 76:278–283
Ghozy S, Kacimi SEO, Elfil M, Sobeeh MG, Reda A, Kallmes KM, Rabinstein AA, Holmes DR Jr, Brinjikji W, Kadirvel R, Kallmes DF (2021) Transient ischemic attacks preceding ischemic stroke and the possible preconditioning of the human brain: a systematic review and meta-analysis. Front Neurol 12:755167
Chinese Society of Neurology, Chinese Stroke Society (2018) Chinese guidelines for diagnosis and treatment of acute ischemic stroke. Chin J Neurol 51:666–682
Wang Y, Han S, Qin H, Zheng H, Jiang B, Cao Y, Gao Y, Guan L, Jia Q, Jiang Y, Jiao Y, Li S, Li Y, Li Z, Liu W, Ru X, Sun D, Sun H, Wang P, Wang T, Zong L, Guo L, Xie X, Xu Y, Xu Y, Yang X, Yang Y, Zhou M, Wang W, CSASCGW Committee (2020) Chinese Stroke Association guidelines for clinical management of cerebrovascular disorders: executive summary and 2019 update of the management of high-risk population. Stroke Vasc Neurol 5:270–278
Fuentes B, Ntaios G, Putaala J, Thomas B, Turc G, Diez-Tejedor E, Organisation ES (2018) European stroke organisation (ESO) guidelines on glycaemia management in acute stroke. Eur Stroke J 3:5–21
Acknowledgements
We thank all the participating centers for their contributions to the CSCA program (the Chinese Stroke Center Alliance).
Funding
This study was supported by grants from the National Natural Science Foundation of China (No. 81825007), Beijing Outstanding Young Scientist Program (No. BJJWZYJH01201910025030), Youth Beijing Scholar Program (No.010), Beijing Talent Project-Class A: Innovation and Development (No. 2018A12), "National Ten-Thousand Talent Plan"-Leadership of Scientific and Technological Innovation, and National Key R&D Program of China (No. 2017YFC1307900, 2017YFC1307905).
Author information
Authors and Affiliations
Contributions
GH: conceptualization; methodology; writing-original draft; writing—review and editing. HG: data curation; software; writing—review and editing. YJ: software; data curation. XY: data curation; project administration. CW: data curation; project administration. YJ: data curation; supervision. ZL: supervision. YW: supervision. YW: conceptualization; funding acquisition; supervision; writing—review and editing.
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflict of interest.
Ethical approval
This study was approved by the Ethics Committee of Beijing Tiantan Hospital. All procedures performed in this study involving human participants were in accordance with the 1964 Helsinki Declaration and its later amendments.
Consent to participate and consent to publication
Each participating hospital received institutional review board approval to enroll participants without individual patient consent under the Common Rule or a waiver of authorization and exemption.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visithttp://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hu, G., Gu, H., Jiang, Y. et al. Prevalence and In-hospital outcomes of diabetes among acute ischemic stroke patients in china: results from the Chinese Stroke Center Alliance. J Neurol 269, 4772–4782 (2022). https://doi.org/10.1007/s00415-022-11112-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-022-11112-z