
Abstract
Objective
This study aimed to assess the efficacy and safety of mycophenolate mofetil (MMF) versus cyclophosphamide (CYC) in patients with active antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV).
Methods
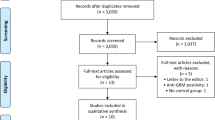
We performed a meta-analysis of four randomized clinical trials (RCTs; 300 patients) to examine the relative efficacy and safety of MMF compared to CYC in patients with active AAV.
Results
There was no significant difference in remission at 6 months between MMF and CYC (odds ratio [OR] 1.311, 95% confidence interval [CI] 0.570–3.017, P = 0.524). Additionally, the relapse rate did not differ between the MMF and CYC groups (OR 1.331, 95% CI 0.497–3.568, P = 0.570). There was no significant difference in serious adverse event (SAE; OR 1.232, 95% CI 0.754–2.014, P = 0.404) and infection rates (OR 0.958, 95% CI 0.561–1.634, P = 0.873) between the MMF and CYC groups. Some heterogeneity was found in the meta-analysis of remission and relapse rates (I2 = 57.4%, 63.4%), but no between-study heterogeneity was found during the meta-analysis of SAE and infection rate. Egger’s regression test showed no evidence of publication bias (Egger’s regression test P-values >0.1).
Conclusion
MMF was an equally effective alternative treatment to CYC and MMF was comparable to CYC in patients with active AAV in terms of safety, suggesting that MMF can be used as an alternative to CYC for remission induction in AAV.
Zusammenfassung
Ziel
Ziel der vorliegenden Studie war es, die Wirksamkeit und Sicherheit von Mycophenolatmofetil (MMF) vs. Cyclophosphamid (CYC) bei Patienten mit aktiver, mit antineutrophilen zytoplasmatischen Antikörpern (ANCA) assoziierter Vaskulitis (AAV) zu untersuchen.
Methoden
Es wurde eine Metaanalyse von 4 randomisierten klinischen Studien (300 Patienten) durchgeführt, um die relative Wirksamkeit und Sicherheit von MMF im Vergleich zu CYC bei Patienten mit aktiver AAV zu untersuchen.
Ergebnisse
Bei der Remission nach 6 Monaten gab es keinen signifikanten Unterschied zwischen MMF und CYC (Odds Ratio, OR: 1,311; 95%-Konfidenzintervall, 95%-KI: 0,570–3,017; p = 0,524). Darüber hinaus unterschied sich die Rezidivrate nicht zwischen der MMF- und der CYC-Gruppe (OR: 1,331; 95%-KI: 0,497–3,568; p = 0,570). Auch gab es keinen signifikanten Unterschied bei der Rate an schweren unerwünschten Ereignissen (SAE; OR: 1,232; 95%-KI: 0,754–2,014; p = 0,404) und Infektionen (OR: 0,958; 95%-KI: 0,561–1,634; p = 0,873) zwischen der MMF- und der CYC-Gruppe. Eine gewisse Heterogenität in der Metaanalyse der Remissions- und Rezidivraten war festzustellen (I2 = 57,4%; 63,4%), aber es bestand keine Heterogenität zwischen den Studien bei der Metaanalyse der Rate an SAE und Infektionen. Im Regressionstest nach Egger zeigte sich kein Anhalt für Publikations-Bias (p-Werte >0,1 im Regressionstest nach Egger).
Schlussfolgerung
Der Behandlungsansatz mit MMF erwies sich als Alternative zu CYC mit gleicher Wirksamkeit, und in Bezug auf die Sicherheit war MMF vergleichbar mit CYC bei Patienten mit aktiver AAV, was darauf hindeutet, dass MMF als Alternative zu CYC für die Induktion einer Remission bei AAV eingesetzt werden kann.



Similar content being viewed by others


References
Jennette JC (2013) Overview of the 2012 revised international Chapel Hill consensus conference nomenclature of vasculitides. Clin Exp Nephrol 17:603–606
Jayne D, Rasmussen N, Andrassy K et al (2003) A randomized trial of maintenance therapy for vasculitis associated with antineutrophil cytoplasmic autoantibodies. N Engl J Med 349:36–44
Jayne D (2008) Challenges in the management of microscopic polyangiitis: past, present and future. Curr Opin Rheumatol 20:3–9
Koukoulaki M, Iatrou C (2019) The role of mycophenolate in the treatment of antineutrophil cytoplasmic antibody-associated vasculitis. World J Nephrol 8:75–82
Faurschou M, Westman K, Rasmussen N, de Groot K, Flossmann O, Hoglund P, Jayne DR, European Vasculitis Study G (2012) Brief Report: long-term outcome of a randomized clinical trial comparing methotrexate to cyclophosphamide for remission induction in early systemic antineutrophil cytoplasmic antibody-associated vasculitis. Arthritis Rheum 64:3472–3477
Han F, Liu G, Zhang X, Li X, He Q, He X, Li Q, Wang S, Wang H, Chen J (2011) Effects of mycophenolate mofetil combined with corticosteroids for induction therapy of microscopic polyangiitis. Am J Nephrol 33:185–192
Jones RB, Hiemstra TF, Ballarin J et al (2019) Mycophenolate mofetil versus cyclophosphamide for remission induction in ANCA-associated vasculitis: a randomised, non-inferiority trial. Ann Rheum Dis 78:399–405
Tuin J, Stassen PM, Bogdan DI, Broekroelofs J, van Paassen P, Cohen Tervaert JW, Sanders JS, Stegeman CA (2019) Mycophenolate mofetil versus cyclophosphamide for the induction of remission in nonlife-threatening relapses of antineutrophil cytoplasmic antibody-associated vasculitis: randomized, controlled trial. Clin J Am Soc Nephrol 14:1021–1028
Hu W, Liu C, Xie H, Chen H, Liu Z, Li L (2008) Mycophenolate mofetil versus cyclophosphamide for inducing remission of ANCA vasculitis with moderate renal involvement. Nephrol Dial Transplant 23:1307–1312
Allison AC, Eugui EM (2000) Mycophenolate mofetil and its mechanisms of action. Immunopharmacology 47:85–118
Lee YH, Song GG (2015) Relative efficacy and safety of tacrolimus, mycophenolate mofetil, and cyclophosphamide as induction therapy for lupus nephritis: a Bayesian network meta-analysis of randomized controlled trials. Lupus 24:1520–1528
Lee YH (2018) Association between the neutrophil-to-lymphocyte ratio, and platelet-to-lymphocyte ratio and rheumatoid arthritis and their correlations with the disease activity: a meta-analysis. J Rheum Dis 25:169–178
Lee YH (2015) Meta-analysis of genetic association studies. Ann Lab Med 35:283–287
Lee YH, Song GG (2019) Causal association between rheumatoid arthritis with the increased risk of type 2 diabetes: a mendelian randomization analysis. J Rheum Dis 26:131–136
Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJM, Gavaghan DJ, McQuay HJ (1996) Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 17:1–12
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 151:264–269
Davey Smith G, Egger M (1997) Meta-analyses of randomised controlled trials. Lancet 350:1182
Higgins JP, Thompson SG (2002) Quantifying heterogeneity in a meta-analysis. Stat Med 21:1539–1558
Egger M, Davey Smith G, Schneider M, Minder C (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315:629–634
Hellmich B, Lamprecht P, Gross WL (2006) Advances in the therapy of Wegener’s granulomatosis. Curr Opin Rheumatol 18:25–32
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
G.G. Song and Y.H. Lee declare that they have no competing interests.
For this article no studies with human participants or animals were performed by any of the authors. All studies performed were in accordance with the ethical standards indicated in each case.
Additional information
Redaktion
U. Müller-Ladner, Bad Nauheim
U. Lange, Bad Nauheim
Rights and permissions
About this article

Cite this article
Song, G.G., Lee, Y.H. Comparative efficacy and safety of mycophenolate mofetil versus cyclophosphamide in patients with active antineutrophil cytoplasmic antibody-associated vasculitis: a meta-analysis of randomized trials. Z Rheumatol 80, 425–431 (2021). https://doi.org/10.1007/s00393-020-00803-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00393-020-00803-5