
Abstract
Purpose
Some gut bacteria can produce enzymes (collagenases) that can break down collagen in the intestinal wall. This could be a part of the pathophysiology of anastomotic leakage (AL). This systematic review aimed to investigate if such bacteria were present more frequently in AL patients versus non-AL patients following colorectal surgery.
Methods
This systematic review was reported according to the PRISMA and AMSTAR guidelines. Before the literature search, a study protocol was registered at PROSPERO (CRD42022363454). We searched PubMed, EMBASE, Google Scholar, and Cochrane CENTRAL on April 9th, 2023, for randomized and observational human studies of AL following colorectal surgery with information on gastrointestinal bacteria. The primary outcome was bacteria with the potential to produce collagenase. The risk of bias was assessed with the Newcastle–Ottawa Scale, as all studies were observational.
Results
We included 15 studies, with a total of 52,945 patients, of which 1,747 had AL, and bacteriological information from feces, mucosa, the resected specimen, or drain fluid was presented. In 10 of the 15 studies, one or more collagenase-producing bacteria were identified in the patients with AL. Neither the bacteria nor the collagenase production were quantified in any of the studies. The studies varied greatly in terms of sample material, analytical method, and time of collection. Studies using DNA sequencing methods did not report findings of collagenase-producing bacteria.
Conclusion
Collagenase-producing bacteria are more common in patients with AL following colorectal surgery than in patients without AL, but the significance is unclear. From the current studies, it is not possible to determine the pathogenicity of the individual gut bacteria.
Similar content being viewed by others


Introduction
Surgical resections of parts of the colon and rectum are common procedures for removing benign conditions (e.g., inflammatory bowel or diverticular diseases), precancerous lesions, or malignant tumors. In most patients, it is possible to re-establish gut continuity with an anastomosis, and the surgical wound in the intestine usually heals within 7–10 days. However, a major complication is anastomotic leakage (AL), which occurs in 2–15% of the patients, with the occurrence rate depending on the specific location of the anastomosis [1,2,3,4,5,6]. Anastomoses in the right side of the colon have the lowest risk of AL (2–5%), and anastomoses to the rectum have the greatest risk of AL (10–15%). Among other risk factors for AL are male gender, increasing age, American Society of Anesthesiologists (ASA) classification > II, renal disease, smoking, obesity, poor nutrition, neoadjuvant chemoradiotherapy, blood loss/transfusion during surgery, and duration of surgery [3, 7,8,9]. AL is associated with considerably increased morbidity, reduced quality of life, prolonged hospital stay (including stays in the intensive care unit) [10], increased costs [11], increased risk of recurrence of cancer, and increased risk of death [12].
Collagen is one of the key components of the extracellular matrix (ECM), and the formation and deposits of collagen fibers are essential for the normal strength of the intestinal wall [13]. However, the surgery disrupts the ECM, causing reduced tensile strength of the collagen fibers in the submucosal layer around the suture material [14].
Healing of the surgical wound is a complex process that can roughly be divided into four partly overlapping temporal phases: Hemostasis, inflammation, proliferation (cellular infiltration, angiogenesis, and re-epithelialization), and maturation/remodeling [15]. Collagen plays a pivotal role in regulating these phases [16]. Disruption of any of the wound healing phases will fixate the healing process in a chronic, non-healing state. Persistent inflammation can lead to chronic wounds by elevating matrix metalloproteinases (MMP) levels and other enzymes. This increases the destruction of ECM components and improper activation of soluble mediators of the wound healing process. Not only is the ECM modified by MMPs and other endogenous enzymes originating from the cells within the wound, but the ECM can also be affected by exogenous enzymes from the bacteria in the gut.
One major group of these is the collagenases, a group of enzymes belonging to the metalloproteinase family, which can play a significant role in the degradation of extracellular collagen fibers. The collagenase enzyme consists of three chains of repeating amino acids that together form a triple helix structure. It has two primary units: the collagen-binding and catalytic domains [17]. The remodeling process of collagen within the intestinal wall is influenced by collagenases originating from either cells that are part of the wound healing process or bacteria that use these as part of their mechanism to invade the human organism [18, 19]. These collagenase-producing bacteria are classified by The Nomenclature Committee of the International Union of Biochemistry and Molecular Biology (NC-IUBMB) under the EC 3.4.24.3 group. Still, more than 50 other bacteria have been reported to have collagenolytic activity (presented in Online Resource 1). The most clinically relevant bacteria are Enterococcus faecalis [18, 20], Clostridioides difficile [21], Klebsiella pneumoniae [22], Pseudomonas aeruginosa [19, 23, 24], Proteus mirabilis [24, 25], and Bacteroides spp. [24, 26, 27].
The idea that there might be a causal relationship between gut bacteria and AL was supported by a recent study [28], where feces from patients with AL after colorectal surgery were transferred to mice undergoing colorectal surgery. The mice showed poorer colonic healing, including reduced levels of ECM components in the wound and increased collagen degradation activity.
The aim of this systematic review was to investigate if bacteria capable of producing collagenase were present more frequently among AL patients vs. non-AL patients following colorectal surgery.
Methods
This systematic review follows the PRISMA (Preferred Reporting Items or Systematic Reviews and Meta-Analysis 2020) [29] and AMSTAR (Assessing the Methodological Quality of Systematic Reviews) guidelines [30]. The PRISMA checklist is available in Online Resource 2.
The protocol was registered at PROSPERO (International Prospective Register of Systematic Reviews) before the literature search (registration number CRD42022363454). Originally, the intention was to present both animal and human studies on the topic. Therefore, our study is registered and approved with PROSPERO as an “Animal research study” with additional information on how to handle human studies. Later in the review process, it was decided only to include human studies. Changing the type of PROSPERO registration from “Animal research study” to “Health research study” was not possible.
Eligibility criteria
The literature search followed the principles of PICO (Patients, Intervention, Comparator, Outcome). The participants were patients with previous colorectal resection and anastomosis, where the studies presented data of bacteria/gut microbiome in either feces, mucosa, the resected specimen, or drain fluid. AL was the exposure (intervention), and similar patients without AL were the comparator.
The primary outcome was identifying bacteria with the potential to produce collagenase; the secondary outcome was reports of other bacteria found.
We included all randomized and observational studies written in English or Danish. There was no restriction on publication year.
Information sources and search strategy
The literature search was conducted on November 30, 2022, and updated on April 8, 2023. We searched PubMed (from 1946 to present), EMBASE (OVID interface, from 1974 to present), Google Scholar (from 2004 to present), and Cochrane Central Register of Controlled Trials (CENTRAL) (from 1992 to present).
The principle of the literature search was a bloc search strategy. Three blocks should cover the topics of AL, colorectal surgery, and bacterial collagenase. The search string for PubMed was: (“anastomotic leak”[MeSH Terms] OR “anastomotic leak*”[All Fields] OR “insufficient anastomosis”[All Fields] OR “anastomotic insufficiency”[All Fields] OR “anastomotic dehiscence”[All Fields] OR “leak*”[All Fields]) AND (“colorectal surgery”[MeSH Terms] OR “colon”[All Fields] OR “colonic”[All Fields] OR “colorectal”[All Fields] OR “rectal”[All Fields] OR “ileorectal”[All Fields] OR “ileoanal”[All Fields] OR “colorectal surgery”[All Fields] OR “colorectal resection”[All Fields] OR “colorectal anastomosis”[All Fields] OR “colon surgery”[All Fields] OR “colon resection”[All Fields] OR “colon anastomosis”[All Fields] OR “colonic surgery”[All Fields] OR “colonic resection”[All Fields] OR “colonic anastomosis”[All Fields] OR “rectal surgery”[All Fields] OR “rectal resection”[All Fields] OR “rectal anastomosis”[All Fields] OR “ileorectal anastomosis”[All Fields] OR “ileoanal anastomosis”[All Fields]) AND (“microbial collagenase”[MeSH Terms] OR “collagenase”[All Fields] OR “collagenoly*”[All Fields] OR “bacterial collagenase”[All Fields] OR “microbial collagenase”[All Fields] OR (“enterococcus”[MeSH Terms] OR “enterococcus”[All Fields]) OR “Pseudomonas aeruginosa”[All Fields] OR “Proteus mirabilis”[All Fields] OR “Bacteroides fragilis”[All Fields] OR “16S”[All Fields] OR “culture”[All Fields] OR “sequenc*”[All Fields]). The search strategies for EMBASE, Google Scholar, and Cochrane CENTRAL are included as Online Resource 3, along with an overview of the bloc search strategy.
In addition to these searches, we performed a snowball search of the reference lists of the included studies, to identify additional studies that could meet the inclusion criteria. To retrieve missing data, we contacted the authors by e-mail.
Study selection
The search results were imported into the online review management solution Covidence [31], automatically removing duplicates. One of the authors verified that no papers were removed by mistake. Two authors screened all the abstracts, and any disagreements were solved by conference with a third author. We excluded case reports, conference abstracts, animal studies, and studies that had not been peer-reviewed.
Data collection
We extracted data from the included studies to a spreadsheet prepared in advance. Author information, year of study, study design, sample material (feces, drain fluid, perioperative sample, and mucosal swab/tissue), method (culture, next-generation sequencing (NGS), quantitative polymerase chain reaction (qPCR), or Clostridioides difficile immunochemical assay (CDI)), patient demography (number of patients, gender, antibiotic usage, bowel preparation, indication for surgery, type of surgery, anastomotic technique, diverting ileostomy, and usage of drain), and outcome (AL-rate, information on any bacteria able to produce collagenase, and other bacteria) were extracted from the studies. Relevant statistical measures were also noted.
Risk of bias
Two authors independently assessed the risk of bias for the studies according to study type. We used Cochrane Risk of Bias tools for randomized trials (Rob 2) [32]. For observational or case–control studies, we used the Newcastle–Ottawa scale (NOS) [33]. However, we made the following minor modifications: For cohort and case–control studies, each study can be graded with up to nine stars combined from three categories (Selection, Comparability, and Outcome). As the “Non-exposed cohort” in the cohort studies obviously had to come from the same group of patients as the “Exposed,” this point in the “Selection” section was left out. Similarly, the “Selection of controls” point was left out in the “Selection” section of the case–control studies because all studies used hospital controls. Therefore, cohort and case–control studies could be assigned a maximum of eight stars. The higher the number of stars, the lower the risk of bias.
The outcome of our study is a description of the bacteria found in the case of AL. Under the “Comparability” category, we awarded each study one star in 1a if the study distinguished colonic from rectal AL and if bacterial information was presented separately for each group. Likewise, in 1b, a star was only awarded if the study presented other relevant risk factors for AL (for instance gender, age, smoker status, or ASA classification) along with specified bacterial information. Any doubts about the grading were solved by conference with the senior author.
Data synthesis and statistics
We planned to do a descriptive presentation of the studies as we anticipated finding heterogeneous studies in a limited number. As both primary and secondary outcomes were reports of the association between the bacteria found in feces/mucosa/specimen/drain fluid in patients with anastomotic leakage, we did not plan to conduct a meta-analysis.
Results
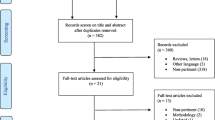
We found a total of 1,676 papers in the search. There were 216 from PubMed, 702 from EMBASE, 748 from Google Scholar, and ten from Cochrane CENTRAL. Out of these, 214 papers were marked as duplicates by Covidence, and this was manually verified. We screened 1,462 abstracts for inclusion, and 1,403 did not meet the inclusion criteria. For the remaining 59 studies, it was possible to retrieve all records for full-text assessment, and of 59 articles, we excluded 44 due to various reasons (12 conference abstracts, nine had no relevant data, seven were animal studies, six had wrong outcome, four were case reports, three were not colorectal surgery, one duplicate, one not peer-reviewed, and one was written in another language than Danish or English). We included 15 studies in this systematic review [34,35,36,37,38,39,40,41,42,43,44,45,46,47,48]. Figure 1 presents the PRISMA 2020 flow diagram for study selection.

PRISMA flow diagram for study screening and selection. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Study characteristics
Most studies (80%) were published from 2019 onwards [34, 35, 37, 39, 41,42,43,44,45,46,47,48]. The majority of the studies were case–control studies [35, 36, 38,39,40,41, 43,44,45,46,47,48], and three were descriptive studies [34, 37, 42].
The number of patients varied greatly from as few as 19 patients [34] to more than 46,000 patients [35]. The total number of patients in all studies was 52,945, of which 1,747 had AL. All studies except one [35] had a majority of male patients. However, one study did not report the sex of the patients [42]. The rate of AL was reported in 14 out of 15 studies [35,36,37,38,39,40,41,42,43,44,45,46,47,48]. The use of antibiotics was reported in nine studies [35,36,37,38, 40, 43, 45, 46, 48], and information about bowel preparation was presented in eight studies [35,36,37,38, 40, 43,44,45]. Less than half of the studies reported the type (hand-sewn or stapled) of anastomosis constructed [36,37,38, 40, 46,47,48]. The formation of a diverting ileostomy at the primary operation was noted in eight studies [37, 38, 40, 42, 43, 46,47,48], along with the placement of a drain [36, 40,41,42,43, 46,47,48]. These parameters had a lot of missing values but are still presented as they are important factors in assessing the quality of the surgery and the anastomosis. The indication for surgery was presented in all studies [34,35,36,37,38,39,40,41,42,43,44,45,46,47,48]. There were 11 studies on colorectal cancer patients [36,37,38,39, 41,42,43,44,45,46,47], and four studies were a mixture of benign and malignant colorectal diseases [34, 35, 40, 48]. One study reported only patients with occult AL [47], a small leak from the anastomosis without any clinical findings. The study characteristics are presented in Table 1.
Sample material and study methods
The majority of studies reported drain fluid as the sample material [34, 36, 38, 40, 46, 47]. Fecal samples were reported in four studies [35, 37, 39, 44], perioperative intraabdominal sampling in two studies [34, 42], mucosal tissue in three studies [41, 43, 48], and one study reported rectal mucosal swabs as sample material [45].
The composition of bacteria in the gut, feces, or abdomen was primarily characterized by cultures [34, 36, 38, 42, 47]. DNA sequencing methods were used in five studies [39, 41, 44, 45, 48], although one study did not specifically report exactly which part of the bacterial DNA had been sequenced [44]. Other study methods were qPCR in three studies [40, 43, 46] and enzyme immunoassay for Clostridioides difficile infection (CDI) in two studies [35, 37]. One study used visual identification and counting with Gram staining of bacteria as the study method [47]. An overview of sample material, time of collection, and study methods is presented in Table 2.
Case–control group comparison
Twelve studies were case–control studies [35, 36, 38,39,40,41, 43,44,45,46,47,48], in which cases of AL were compared with controls without AL. One study found that the risk of AL had an increased OR of 2.34 among patients with CDI [35]. A similar finding was that the risk was increased almost fourfold among patients with increased levels of Bifidobacterium spp. in mucosal tissue adjacent to the anastomosis [43]. DNA sequencing of preoperative fecal samples showed that two specific bacteria (Acinetobacter lwoffii and Acinetobacter johnsonii) were found exclusively among AL patients, whereas non-AL patients had Barnesiella intestinihominis (absent among AL patients) [44]. Infectious complications (including AL) were reduced with diminished levels of Proteobacteria [45] from rectal swabs, and there was increased alpha diversity in postoperatively collected fecal samples from AL patients [39]. Another study found increased levels of the families Lachnospiraceae and Bacteroidaceae in mucosal tissue among AL patients, and they presented a prediction model for AL based on this in combination with the alpha diversity of the samples [48].
Cultures from drain samples showed that almost all AL patients had positive cultures on postoperative day (POD) 5 [36], whereas nearly all non-AL patients had a negative culture [38]. One study showed no difference in positive cultures among AL and non-AL patients on POD1-3 [46], and another found that the absence of E. faecalis in drain fluid on POD3 had a high negative predictive value for AL [40]. The identified bacteria in all studies and the type of surgery, are presented in Table 3.
Collagenase-producing bacteria
Bacteria with the ability to produce collagenase were reported in 10 out of 15 studies [34,35,36,37,38, 40, 42, 43, 46, 47]. One study found collagenase-producing bacteria in 14 of 19 (73.7%) bacterial cultures, but it is not specified which bacteria were found [34]. Enterococcus faecalis was most frequently reported [34, 40, 43, 46, 47]. On the genus level, there were reports of Pseudomonas spp. [38, 42], Klebsiella spp. [38, 42], and Proteus spp. [36] in samples from AL patients. On the species level, both Pseudomonas aeruginosa [47] and Klebsiella pneumoniae were found [36] in samples from AL patients. Two studies had CDI as the primary outcome [35, 37]. One study did not find Enterococcus spp. among the AL patients, although some of the control patients without AL had Enterococcus spp. in the drain fluid [36]. None of the studies presented information of the actual presence of collagenase in the bacterial samples.
Risk of bias
The Newcastle Ottawa scale was used for all studies, as no randomized trials were included. The median score for all studies was six stars (range 3–7). For the cohort studies, the score was five stars (range 4–6), whereas the case–control studies had a median score of six stars (range 3–7). Very few stars were assigned in the “Comparability” category, as most studies present a mixture of both colonic and rectal resections without segregating the bacterial findings. Only five studies were given a star in Comparability point 1a [36,37,38, 46, 48], and just one study in Comparability point 1b [35]. Details of the bias assessment are presented in Table 4.
Discussion
This systematic review provides an overview of the bacteria associated with AL after colorectal surgery. The main finding in our study is that 10 out of 15 studies identify one or several bacteria among AL patients that have the potential to produce collagenase(s), although no studies had analyzed the collagenolytic activity of the samples. The studies varied greatly with regard to sample material, study method, and time of sample collection.
The most commonly found bacteria in AL was Enterococcus faecalis, from studies using culture or qPCR as study method. This is a common bacteria in the intestinal tract, as it (together with Enterococcus faecium) constitutes up to 1% of the adult gut microbiota [50]. Under normal circumstances, it is not a cause of infection, but in case of dysbiosis in the gut (for instance after bowel preparation, antibiotics, and surgical stress), it can begin to express virulence factors that make it a cause of infection. Two studies reported that Clostridioides difficile (transferred from the genus Clostridium in 2016) infection implied an increased risk of AL with an odds ratio of 2.39 [35] and a relative risk of 13.7 [37]. C. difficile is also a common gut bacteria; it is most common among infants and decreases with age [51]. Infections with C. difficile usually occur during hospital admissions and antibiotic treatment. C. difficile can cause sepsis and produce toxins capable of causing gastrointestinal symptoms varying from mild diarrhea to pseudomembranous enterocolitis and toxic megacolon. Patients who received neoadjuvant chemoradiotherapy have an increased risk of developing CDI [52] and severe dysbiosis of the gut microbiota [53].
Pseudomonas spp. (including Pseudomonas aeruginosa) were found in several studies. There are conflicting reports in the literature as to whether P. aeruginosa is an ordinary member of the normal gut microbiota or not; some argue that this is the case [54, 55], whereas others state otherwise [56, 57]. Treatment of P. aeruginosa is usually challenging because the bacteria is resistant to several types of antibiotics [58]. Klebsiella pneumoniae is also part of the normal gut microbiota and is a common cause of nosocomial infection. Klebsiella pneumoniae and Pseudomonas aeruginosa have approximately 99% similar DNA sequences, which makes them susceptible to being mistaken for one or another when interpreting results from microbiome studies [59]. Another genus of bacteria in the gut is Bacteroides, and several species can produce collagenase [60]. There are more than 20 known species, most of which can be isolated from human feces. In the studies in this review, Bacteroides spp. were overrepresented among AL patients.
Most of the studies used either culture, qPCR, or C. difficile immunoassay to identify the bacteria, and all of these studies detected one or more collagenase-producing bacteria. All the qPCR studies targeted E. faecalis and Escherichia coli [40, 43, 46], and one study also targeted the Bifidobacterium genus and Fusobacterium nucleatum [43]. All these species are known to be able to produce collagenase.
The five studies that used DNA sequencing methods did find bacterial differences between the AL and non-AL groups. Still, none of the reported bacteria are known to be capable of producing collagenase. This could be due to underreporting of the results, as microbiome studies generate vast amounts of output data, and a complete presentation of the data on the species level rarely seems appropriate. One significant advantage of microbiome analyses is that the anaerobic bacteria are not eliminated by the sampling method, as might be the case using the conventional culture because sampling these bacteria alive requires special attention and equipment [61].
In the majority of the studies, bacteria with the capability to produce collagenase were found among AL patients, and to a lesser degree among patients without AL. According to the literature, all of these bacterial species are known as common members of the intestinal microbiota. This implies that it is not unusual for both patients with or without AL to have these bacteria in the intestine before surgery. However, it is noteworthy that once AL occurs, bacteria with the capability to produce collagenase are a frequent finding in the surroundings of the anastomosis. It is impossible to know whether this is the cause of AL, but it does show some degree of association between this selected group of bacteria and AL. The production of collagenase in a bacterial sample could be quantified by means of zymography [62], or transcriptomic analysis to assess gene activity. Other potential pathways for bacteria to contribute to the development of AL could be that their presence induces a cascade of reactions in the intestine after surgery. Animal models have shown that E. faecalis can activate two alternative pathways that lead to collagen degradation. One is through activation of human recombinant MMP9 [18], the other through activation of tissue plasminogen to active plasmin that can cleave collagen and also active MMPs [63]. The functional pathways of the bacteria are outside the scope of this review.
The review has identified some challenges/limitations originating from the current literature. It contains a limited number of studies with a relatively small number of patients in each study, although one study had more than 46,000 patients [35]. All studies have different ways of identifying and reporting bacterial findings, making them very hard to compare equally. Several studies did not report basic confounders for AL, such as smoker status, body mass index, ASA classification, renal disease, neoadjuvant chemoradiotherapy, or blood loss during surgery. Only a minor part of the studies had reports of bowel preparation, preoperative antibiotics, anastomotic technique, and the use of a diverting ileostomy; factors that might also be important to the overall quality of the surgery.
All studies are based on retrospective data, and there might be a degree of reporting bias regarding which results are included in the papers. Only a selection of the bacterial findings may be described in the papers. This could be due to various reasons, for instance, that the complete findings would take up too much space in the papers, or the authors decided that some of the information was irrelevant. In addition, there might be a degree of underreporting of complications in either the patient charts or database data.
The strengths of this review are that it follows PRISMA guidelines and was registered at PROSPERO before the literature search. This increases the transparency in the review process and reduce selection bias. The review is, to our knowledge, the first that aims at describing the microbiology in the surroundings of an AL, based on all available clinical studies. Even though narrative reviews on the association between bacteria in the gut and AL have been published [64,65,66,67,68,69], this is the first systematic review using multiple literature sources, and the first to focus on bacteria with collagenase-producing capability.
The amount of gut microbiome studies increases yearly, as both analytical capacity and availability increase, and costs are constantly reduced. To increase the quality of microbiome studies, the STORMS (Strengthening The Organization and Reporting of Microbiome Studies) checklist was formulated in 2021 [70]. None of the microbiome studies presented in this review used the STORMS checklist. However, three studies [41, 44, 48] were published before the STORMS checklist.
In conclusion, we found that collagenase-producing bacteria were more common in patients with AL following colorectal surgery than in patients without AL, but the significance is unclear. Future studies could focus on the pathogenicity of bacteria found in AL after colorectal surgery.
Data availability
All data generated or analyzed in the study are included in this article. Further inquiries can be directed to the corresponding author.
References
Kube R, Mroczkowski P, Granowski D et al (2010) Anastomotic leakage after colon cancer surgery: a predictor of significant morbidity and hospital mortality, and diminished tumour-free survival. Eur J Surg Oncol 36(2):120–124. https://doi.org/10.1016/j.ejso.2009.08.011
Krarup P-M, Jorgensen LN, Andreasen AH et al (2012) A nationwide study on anastomotic leakage after colonic cancer surgery. Colorectal Dis 14(10):e661–e667. https://doi.org/10.1111/j.1463-1318.2012.03079.x
Pommergaard HC, Gessler B, Burcharth J et al (2014) Preoperative risk factors for anastomotic leakage after resection for colorectal cancer: a systematic review and meta-analysis. Colorectal Dis 16(9):662–671. https://doi.org/10.1111/CODI.12618
Peeters KCMJ, Tollenaar RAEM, Marijnen CAM et al (2005) Risk factors for anastomotic failure after total mesorectal excision of rectal cancer. Br J Surg 92(2):211–216. https://doi.org/10.1002/BJS.4806
Koneru S, Reece MM, Goonawardhana D et al (2023) Right hemicolectomy anastomotic leak study: a review of right hemicolectomy in the binational clinical outcomes registry (BCOR). ANZ J Surg 93(6):1646–1651. https://doi.org/10.1111/ans.18337
Pellino G, Frasson M, García-Granero A et al (2018) Predictors of complications and mortality following left colectomy with primary stapled anastomosis for cancer: results of a multicentric study with 1111 patients. Color Dis 20(11):986–995. https://doi.org/10.1111/codi.14309
McDermott FD, Heeney A, Kelly ME et al (2015) Systematic review of preoperative, intraoperative and postoperative risk factors for colorectal anastomotic leaks. Br J Surg 102(5):462–479. https://doi.org/10.1002/BJS.9697
Sciuto A, Merola G, De Palma GD et al (2018) Predictive factors for anastomotic leakage after laparoscopic colorectal surgery. World J Gastroenterol 24(21):2247–2260. https://doi.org/10.3748/wjg.v24.i21.2247
Hoek VT, Buettner S, Sparreboom CL et al (2022) A preoperative prediction model for anastomotic leakage after rectal cancer resection based on 13.175 patients. Eur J Surg Oncol 48(12):2495–501. https://doi.org/10.1016/j.ejso.2022.06.016
Arron MNN, Custers JAE, van Goor H et al (2023) The association between anastomotic leakage and health-related quality of life after colorectal cancer surgery. Colorectal Dis 25(7):1381–1391. https://doi.org/10.1111/codi.16543
Weber MC, Berlet M, Stoess C et al (2023) A nationwide population-based study on the clinical and economic burden of anastomotic leakage in colorectal surgery. Langenbeck’s Arch Surg 408(1):55. https://doi.org/10.1007/S00423-023-02809-4
Krarup P-M, Nordholm-Carstensen A, Jorgensen LN et al (2014) Anastomotic leak increases distant recurrence and long-term mortality after curative resection for colonic cancer. Ann Surg 259(5):930–938. https://doi.org/10.1097/SLA.0b013e3182a6f2fc
Syk I, Ågren MS, Adawi D et al (2001) Inhibition of matrix metalloproteinases enhances breaking strength of colonic anastomoses in an experimental model. Br J Surg 88(2):228–234. https://doi.org/10.1046/J.1365-2168.2001.01649.X
Stumpf M, Klinge U, Wilms A et al (2005) Changes of the extracellular matrix as a risk factor for anastomotic leakage after large bowel surgery. Surgery 137(2):229–234. https://doi.org/10.1016/j.surg.2004.07.011
Lam A, Fleischer B, Alverdy J (2020) The biology of anastomotic healing-the unknown overwhelms the known. J Gastrointest Surg 24(9):2160–2166. https://doi.org/10.1007/s11605-020-04680-w
Mathew-Steiner SS, Roy S, Sen CK (2021) Collagen in wound healing. Bioengineering 8(5):63. https://doi.org/10.3390/bioengineering8050063
Duarte AS, Correia A, Esteves AC (2016) Bacterial collagenases - a review. Crit Rev Microbiol 42(1):106–126. https://doi.org/10.3109/1040841X.2014.904270
Shogan BD, Belogortseva N, Luong PM et al (2015) Collagen degradation and MMP9 activation by Enterococcus faecalis contribute to intestinal anastomotic leak. Sci Transl Med 7(286):286ra68. https://doi.org/10.1126/scitranslmed.3010658
Olivas AD, Shogan BD, Valuckaite V et al (2012) Intestinal tissues induce an SNP mutation in Pseudomonas aeruginosa that enhances its virulence: possible role in anastomotic leak. PLoS One 7(8):e44326. https://doi.org/10.1371/journal.pone.0044326
Jackson RJ, Lien Dao M, Lim DV (1995) Modified FALGPA assay for cell-associated collagenolytic activity. J Microbiol Methods 21(2):209–215. https://doi.org/10.1016/0167-7012(94)00050-H
Steffen EK, Hentges DJ (1981) Hydrolytic enzymes of anaerobic bacteria isolated from human infections. J Clin Microbiol 14(2):153–156. https://doi.org/10.1128/jcm.14.2.153-156.1981
Suphatharaprateep W, Cheirsilp B, Jongjareonrak A (2011) Production and properties of two collagenases from bacteria and their application for collagen extraction. N Biotechnol 28(6):649–655. https://doi.org/10.1016/j.nbt.2011.04.003
Diener B, Carrick L, Berk RS (1973) In vivo studies with collagenase from Pseudomonas aeruginosa. Infect Immun 7(2):212–217. https://doi.org/10.1128/iai.7.2.212-217.1973
McGregor JA, Lawellin D, Franco-Buff A et al (1986) Protease production by microorganisms associated with reproductive tract infection. Am J Obstet Gynecol 154(1):109–114. https://doi.org/10.1016/0002-9378(86)90404-7
Guyton KL, Levine ZC, Lowry AC et al (2019) Identification of collagenolytic bacteria in human samples: screening methods and clinical implications for resolving and preventing anastomotic leaks and wound complications. Dis Colon Rectum 62(8):972–979. https://doi.org/10.1097/DCR.0000000000001417
Jin KC, Barua PK, Zambon J et al (1989) Proteolytic activity in black-pigmented bacteroides species. J Endod 15(10):463–467. https://doi.org/10.1016/S0099-2399(89)80025-1
Robertson PB, Lantz M, Marucha PT et al (1982) Collagenolytic activity associated with Bacteroides species and Actinobacillus actinomycetemcomitans. J Periodontal Res 17(3):275–283. https://doi.org/10.1111/J.1600-0765.1982.TB01154.X
Hajjar R, Gonzalez E, Fragoso G et al (2023) Gut microbiota influence anastomotic healing in colorectal cancer surgery through modulation of mucosal proinflammatory cytokines. Gut 72(6):1143–1154. https://doi.org/10.1136/gutjnl-2022-328389
Page MJ, McKenzie JE, Bossuyt PM et al (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg 88(March 2021):105906. https://doi.org/10.1016/j.ijsu.2021.105906
Shea BJ, Reeves BC, Wells G et al (2017) AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 358:j4008. https://doi.org/10.1136/bmj.j4008
Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia. Available at http://www.covidence.org
Sterne JAC, Savović J, Page MJ et al (2019) RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 366:l4898. https://doi.org/10.1136/bmj.l4898
Wells G, Shea B, O’Connell D et al (2000) The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa Hospital Research Institute, Ottawa, ON Available at https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp
Anderson DI, Keskey R, Ackerman MT et al (2021) Enterococcus faecalis is associated with anastomotic leak in patients undergoing colorectal surgery. Surg Infect (Larchmt) 22(10):1047–1051. https://doi.org/10.1089/sur.2021.147
Baker SE, Monlezun DJ, Ambroze WL et al (2022) Anastomotic leak is increased with clostridium difficile infection after colectomy: machine learning-augmented propensity score modified analysis of 46 735 patients. Am Surg 88(1):74–82. https://doi.org/10.1177/0003134820973720
Bilgin IA, Hatipoglu E, Aghayeva A et al (2017) Predicting value of serum procalcitonin, C-reactive protein, drain fluid culture, drain fluid interleukin-6, and tumor necrosis factor-α levels in anastomotic leakage after rectal resection. Surg Infect (Larchmt) 18(3):350–356. https://doi.org/10.1089/sur.2016.222
Calu V, Toma E-A, Enciu O et al (2019) Clostridium difficile infection and colorectal surgery: is there any risk? Medicina (Kaunas) 55(10):683. https://doi.org/10.3390/medicina55100683
Fouda E, El Nakeeb A, Magdy A et al (2011) Early detection of anastomotic leakage after elective low anterior resection. J Gastrointest Surg 15(1):137–144. https://doi.org/10.1007/s11605-010-1364-y
Jin X, Liu Y, Yan W et al (2022) Gut microbiota from nCAL patients promotes colon anastomotic healing by inducing collagen synthesis in epithelial cells. J Gastroenterol Hepatol 37(9):1756–1767. https://doi.org/10.1111/jgh.15946
Komen N, Slieker J, Willemsen P et al (2014) Polymerase chain reaction for Enterococcus faecalis in drain fluid: the first screening test for symptomatic colorectal anastomotic leakage. The Appeal-study: analysis of parameters predictive for evident anastomotic leakage. Int J Colorectal Dis 29(1):15–21. https://doi.org/10.1007/s00384-013-1776-8
Li Y-D, He K-X, Zhu W-F (2019) Correlation between invasive microbiota in margin-surrounding mucosa and anastomotic healing in patients with colorectal cancer. World J Gastrointest Oncol 11(9):717–728. https://doi.org/10.4251/wjgo.v11.i9.717
Lohsiriwat V, Assawasirisin C (2020) Anastomotic leakage following 4,357 colorectal cancer surgery: incidence, presentation, pathogens, treatment and outcome. J Med Assoc Thail 103(5):6–11
Mima K, Sakamoto Y, Kosumi K et al (2020) Mucosal cancer-associated microbes and anastomotic leakage after resection of colorectal carcinoma. Surg Oncol 32:63–68. https://doi.org/10.1016/j.suronc.2019.11.005
Palmisano S, Campisciano G, Iacuzzo C et al (2020) Role of preoperative gut microbiota on colorectal anastomotic leakage: preliminary results. Updates Surg 72(4):1013–1022. https://doi.org/10.1007/s13304-020-00720-x
Reuvers JRD, Budding AE, van Egmond M et al (2023) Gut proteobacteria levels and colorectal surgical infections: SELECT trial. Br J Surg 110(2):129–132. https://doi.org/10.1093/bjs/znac288
Sparreboom CL, Komen N, Rizopoulos D et al (2020) A multicentre cohort study of serum and peritoneal biomarkers to predict anastomotic leakage after rectal cancer resection. Colorectal Dis 22(1):36–45. https://doi.org/10.1111/codi.14789
Tominaga T, Nonaka T, Oyama S et al (2022) Utility of drain fluid culture and gram stain in early intervention for occult anastomotic leakage in colorectal cancer. Anticancer Res 42(6):3091–8. https://doi.org/10.21873/anticanres.15797
van Praagh JB, de Goffau MC, Bakker IS et al (2019) Mucus microbiome of anastomotic tissue during surgery has predictive value for colorectal anastomotic leakage. Ann Surg 269(5):911–916. https://doi.org/10.1097/SLA.0000000000002651
Bakker IS, Morks AN, ten Cate Hoedemaker HO et al (2017) Randomized clinical trial of biodegradeable intraluminal sheath to prevent anastomotic leak after stapled colorectal anastomosis. Br J Surg 104(8):1010–1019. https://doi.org/10.1002/BJS.10534
Dubin K, Pamer EG (2014) Enterococci and their interactions with the intestinal microbiome. Microbiol Spectr 5(6). https://doi.org/10.1128/microbiolspec.BAD-0014-2016
Sehgal K, Khanna S (2021) Gut microbiome and Clostridioides difficile infection: a closer look at the microscopic interface. Therap Adv Gastroenterol 14:1756284821994736. https://doi.org/10.1177/1756284821994736
Puerta-Alcalde P, Garcia-Vidal C, Soriano A (2023) Prevention and treatment of C. difficile in cancer patients. Curr Opin Infect Dis 36:1–8. https://doi.org/10.1097/QCO.0000000000000954
Moraitis I, Guiu J, Rubert J (2023) Gut microbiota controlling radiation-induced enteritis and intestinal regeneration. Trends Endocrinol Metab 34(8):489–501. https://doi.org/10.1016/j.tem.2023.05.006
Griffith SJ, Nathan C, Selander RK et al (1989) The epidemiology of Pseudomonas aeruginosa in oncology patients in a general hospital. J Infect Dis 160(6):1030–1036. https://doi.org/10.1093/infdis/160.6.1030
Fusco A, Savio V, Stelitano D et al (2021) The intestinal biofilm of Pseudomonas aeruginosa and Staphylococcus aureus is inhibited by antimicrobial peptides HBD-2 and HBD-3. Appl Sci 11(14):6595. https://doi.org/10.3390/app11146595
Rubio-Gómez JM, Santiago CM, Udaondo Z et al (2020) Full transcriptomic response of Pseudomonas aeruginosa to an inulin-derived fructooligosaccharide. Front Microbiol 11(February):202. https://doi.org/10.3389/fmicb.2020.00202
Wheatley RM, Caballero JD, van der Schalk TE et al (2022) Gut to lung translocation and antibiotic mediated selection shape the dynamics of Pseudomonas aeruginosa in an ICU patient. Nat Commun 13(1):6523. https://doi.org/10.1038/s41467-022-34101-2
Breidenstein EBM, de la Fuente-Núñez C, Hancock REW (2011) Pseudomonas aeruginosa: all roads lead to resistance. Trends Microbiol 19(8):419–426. https://doi.org/10.1016/j.tim.2011.04.005
Conlan S, Kong HH, Segre JA (2012) Species-level analysis of DNA sequence data from the NIH Human Microbiome Project. Plos One 7(10):e47075. https://doi.org/10.1371/journal.pone.0047075
Harrington DJ (1996) Bacterial collagenases and collagen-degrading enzymes and their potential role in human disease. Infect Immun 64(6):1885–1891. https://doi.org/10.1128/iai.64.6.1885-1891.1996
Guilhot E, Khelaifia S, La Scola B et al (2018) Methods for culturing anaerobes from human specimen. Future Microbiol 13(3):369–381. https://doi.org/10.2217/fmb-2017-0170
Prasad S, Roy I (2017) A sensitive, rapid, and specific technique for the detection of collagenase using zymography. Methods Mol Biol 1626:115–121. https://doi.org/10.1007/978-1-4939-7111-4_10
Jacobson RA, Wienholts K, Williamson AJ et al (2020) Enterococcus faecalis exploits the human fibrinolytic system to drive excess collagenolysis: implications in gut healing and identification of druggable targets. Am J Physiol Gastrointest Liver Physiol 318(1):G1-9. https://doi.org/10.1152/ajpgi.00236.2019
Agnes A, Puccioni C, D’Ugo D et al (2021) The gut microbiota and colorectal surgery outcomes: facts or hype? A narrative review BMC Surg 21(1):83. https://doi.org/10.1186/s12893-021-01087-5
Lauka L, Reitano E, Carra MC et al (2019) Role of the intestinal microbiome in colorectal cancer surgery outcomes. World J Surg Oncol 17(1):204. https://doi.org/10.1186/s12957-019-1754-x
Bartolini I, Risaliti M, Ringressi MN et al (2020) Role of gut microbiota-immunity axis in patients undergoing surgery for colorectal cancer: focus on short and long-term outcomes. World J Gastroenterol 26(20):2498–2513. https://doi.org/10.3748/wjg.v26.i20.2498
Lederer A-K, Pisarski P, Kousoulas L et al (2017) Postoperative changes of the microbiome: are surgical complications related to the gut flora? A systematic review BMC Surg 17(1):125. https://doi.org/10.1186/s12893-017-0325-8
Bachmann R, Leonard D, Delzenne N et al (2017) Novel insight into the role of microbiota in colorectal surgery. Gut 66(4):738–749. https://doi.org/10.1136/gutjnl-2016-312569
Hajjar R, Santos MM, Dagbert F et al (2019) Current evidence on the relation between gut microbiota and intestinal anastomotic leak in colorectal surgery. Am J Surg 218(5):1000–1007. https://doi.org/10.1016/j.amjsurg.2019.07.001
Mirzayi C, Renson A, Genomic Standards Consortium et al (2021) Reporting guidelines for human microbiome research: the STORMS checklist. Nat Med 27(11):1885–92. https://doi.org/10.1038/s41591-021-01552-x
Acknowledgements
This review was conducted as a part of a PhD, supported by the Department of Surgery, Holbæk Hospital; House of Research, Holbæk Hospital; The Research Foundation of Region Zealand; The Vissing Foundation, Dagmar Marshalls Foundation, and The Danish Cancer Society.
Funding
This review was conducted as a part of a PhD, supported by the Department of Surgery, Holbæk Hospital; House of Research, Holbæk Hospital; The Research Foundation of Region Zealand; The Vissing Foundation, Dagmar Marshalls Foundation, and The Danish Cancer Society.
Author information
Authors and Affiliations
Contributions
A.B.J. had the idea for the article, performed the literature search, study selection, data extraction, data analysis, quality assessment, and drafted the article. I.J. performed the study selection, data extraction, analysis, and quality assessment. L.F.H. and B.B. had the idea for the article and supervised all steps in the process. All authors critically reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
An ethics statement is not applicable as this study was based exclusively on published literature.
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Jørgensen, A.B., Jonsson, I., Friis-Hansen, L. et al. Collagenase-producing bacteria are common in anastomotic leakage after colorectal surgery: a systematic review. Int J Colorectal Dis 38, 275 (2023). https://doi.org/10.1007/s00384-023-04562-y
Accepted:
Published:
DOI: https://doi.org/10.1007/s00384-023-04562-y