
Abstract
Introduction
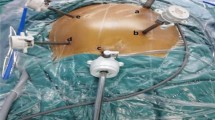
The concept of complete mesocolic excision (CME) with central vascular ligation (CVL) for treatment of right colon cancer evolved over last one decade. It decreases local recurrences and improves the survival rates. We describe our novel technique which involves first posterior sharp dissection between planes of parietal and visceral fascia of mesocolon followed by ligation of ileocolic, right colic and middle colic pedicles at their origin. We highlight the technical variations with various techniques and advantages over conventional medial to lateral approach in current study.
Aim
The outcomes were measured in terms of technical feasibility, short-term outcomes and pathological radicality of current laparoscopic technique (IRETA) for CME with CVL.
Materials and methods
Two hundred twelve patients (163 males) who underwent laparoscopic CME for right colon cancer over the period of January 2009 to December 2013 were analysed via prospectively maintained database.
Results
97.16 % of patients (n = 206) underwent laparoscopic CME while six patients required open conversion. Mean operative time was 142 ± 28.4 min with median hospital stay of 5 days (range 4–11). The median count of lymph node harvested were 24 (range 10–42). The complete mesocolic excision plane was achieved in 93.8 % patients. 84.4 % (n = 179) of our patients were having (T3, N+) disease on pathological examination. The overall morbidity (<30 days) was 9.9 %.
Conclusion
Laparoscopic initial retrocolic endoscopic tunnel approach (IRETA) for CME with CVL in right colonic cancers is safe, simpler and feasible laparoscopic approach with minimal complications. Creation of retro colic tunnel is key highlight of IRETA approach. This approach becomes especially useful in patients with late presentations where complete mesocolic excision remains essential to enhance oncological radicality as per evidence available.




Similar content being viewed by others


References
Heald RJ, Ryall RD (1986) Recurrence and survival after total mesorectal excision for rectal cancer. Lancet 1(8496):1479–1482
West NP, Kobayashi H, Takahashi K, Perrakis A, Weber K, Hohenberger W et al (2012) Understanding optimal colonic cancer surgery: comparison of Japanese D3 resection and European complete mesocolic excision with central vascular ligation. J Clin Oncol 30(15):1763–1769
Hohenberger W, Weber K, Matzel K, Papadopoulos T, Merkel S (2009) Standardized surgery for colonic cancer: complete mesocolic excision and central ligation—technical notes and outcome. Color Dis 11(4):354–364
Bae SU, Saklani AP, Lim DR, Kim DW, Hur H, Min BS et al (2014) Laparoscopic-assisted versus open complete mesocolic excision and central vascular ligation for right-sided colon cancer. Ann Surg Oncol 21(7):2288–2294
Veldkamp R, Kuhry E, Hop WC, Jeekel J, Kazemier G, Bonjer HJ et al (2005) COlon cancer Laparoscopic or Open Resection Study Group (COLOR). Laparoscopic surgery versus open surgery for colon cancer: short-term outcomes of a randomised trial. Lancet Oncol 6(7):477–484
Bertelsen CA, Bols B, Ingeholm P, Jansen JE, Neuenschwander AU, Vilandt J (2011) Can the quality of colonic surgery be improved by standardization of surgical technique with complete mesocolic excision? Color Dis 13(10):1123–1129
Quirke P, Steele R, Monson J, Grieve R, Khanna S, Couture J, MRC CR07/NCIC-CTG CO16 Trial Investigators; NCRI Colorectal Cancer Study Group et al (2009) Effect of the plane of surgery achieved on local recurrence in patients with operable rectal cancer: a prospective study using data from the MRC CR07 and NCIC-CTG CO16 randomised clinical trial. Lancet 373(9666):821–828
Galizia G, Lieto E, De Vita F, Ferraraccio F, Zamboli A, Mabilia A et al (2014) Is complete mesocolic excision with central vascular ligation safe and effective in the surgical treatment of right-sided colon cancers? A prospective study. Int J Color Dis 29(1):89–97
Kang J, Kim IK, Kang SI, Sohn SK, Lee KY (2014) Laparoscopic right hemicolectomy with complete mesocolic excision. Surg Endosc 28(9):2747–2751
Adamina M, Manwaring ML, Park KJ, Delaney CP (2012) Laparoscopic complete mesocolic excision for right colon cancer. Surg Endosc 26(10):2976–2980
Gouvas N, Pechlivanides G, Zervakis N, Kafousi M, Xynos E (2012) Complete mesocolic excision in colon cancer surgery: a comparison between open and laparoscopic approach. Color Dis 14(11):1357–1364
Cao QF, Lu AG, Ma JJ, Zheng MH (2010) The clinical analysis of laparoscopic-assisted radical right hemicolectomy: a report of 177 cases. J Surg Concepts Pr 15:361–365
Rotholtz NA, Bun ME, Tessio M, Lencinas SM, Laporte M, Aued ML et al (2009) Laparoscopic colectomy: medial versus lateral approach. Surg Laparosc Endosc Percutan Tech 19(1):43–47
Liang JT, Lai HS, Lee PH (2007) Laparoscopic medial-to-lateral approach for the curative resection of right-sided colon cancer. Ann Surg Oncol 14(6):1878–1879
Yan J, Ying MG, Zhou D, Chen X, Chen LC, Ye WF et al (2010) A prospective randomized control trial of the approach for laparoscopic right hemi-colectomy: medial-tolateral versus lateral-to-medial. Zhonghua Wei Chang Wai Ke Za Zhi 13(6):403–405
West NP, Morris EJ, Rotimi O, Cairns A, Finan PJ, Quirke P (2008) Pathology grading of colon cancer surgical resection and its association with survival: retrospective observational study. Lancet Oncol 9(9):857–865
Solomon MJ, Egan M, Roberts RA, Philips J, Russell P (1997) Incidence of free colorectal cancer cells on the peritoneal surface. Dis Colon Rectum 40(11):1294–1298
Parsons HM, Tuttle TM, Kuntz KM, Begun JW, McGovern PM, Virnig BA (2011) Association between lymph node evaluation for colon cancer and node positivity over the past 20 years. JAMA 306(10):1089–1097
Acknowledgments
The technique was presented by Palanivelu C et al. Initial retrocolic endoscopic tunnel approach: IRETA—for laparoscopic right colectomy in malignant disease presented at ELSA 2006 as an oral presentation (Endoscopic and Laparoscopic Surgeons of Asia Congress at Seoul, South Korea, October 18 to 21, 2006). The current study ‘Initial Retrocolic Endoscopic Tunnel Approach [IRETA] With Complete Mesocolic Excision [CME] For Right Colonic Cancers: Technique, Pathological Radicality and short term outcomes’ was presented as an oral presentation at (Indian association of surgical gastroenterology) IASG 2014 at Ahmedabad, October 2 to 5, 2014.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Subbiah, R., Bansal, S., Jain, M. et al. Initial retrocolic endoscopic tunnel approach (IRETA) for complete mesocolic excision (CME) with central vascular ligation (CVL) for right colonic cancers: technique and pathological radicality. Int J Colorectal Dis 31, 227–233 (2016). https://doi.org/10.1007/s00384-015-2415-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-015-2415-3