
Abstract
In patients with heart failure, it is unknown whether the extracellular water (ECW)/intracellular water (ICW) ratio is associated with muscle strength, and thus, it is not well understood whether poor muscle quality contributes to muscular weakness. This study examined the relationship among hand grip strength, skeletal muscle mass index (SMI), and upper limb ECW/ICW ratio in patients with heart failure. This study followed a cross-sectional design. Demographic data, medical information, and hand grip strength were collected. The SMI and ECW/ICW ratio were measured using bio-impedance analysis (BIA). Hierarchical multiple regression analysis was conducted to identify factors associated with hand grip strength. 51 patients with heart failure were analyzed for this study (mean age 84.58 ± 7.18). Hierarchical multiple regression analysis identified SMI as well as upper limb ECW/ICW ratio as factors associated with hand grip strength, independent of age, sex, body mass index, and Life Space Assessment scores. Standardized partial regression coefficients representing the magnitude of involvement of each independent variable were 0.33 and − 0.16. The coefficient of determination adjusted for degrees of freedom (R2), representing the contribution rate of the regression equation, was 0.830. We revealed that loss of hand grip strength in patients with heart failure is associated with not only with a decrease in skeletal muscle mass, but also with a decline in muscle quality, characterized by an increased upper limb ECW/ICW ratio. BIA is a simple and useful method to measure the ECW/ICW ratio, and in turn, the muscle quality, in patients with heart failure.
Similar content being viewed by others


Introduction
Currently, the world’s heart failure prevalence is on the verge of 30 million [1]. According to the 2013–2016 National Health and Nutrition Examination Survey, the number of patients with heart failure in the United States rose to over 6.2 million and is expected to reach 8 million by 2030 [1]. Patients with heart failure tend to have a high incidence of sarcopenia [2], which is characterized by a decrease in skeletal muscle mass and an increase in muscular weakness. Heart failure patients with sarcopenia experience worsened physical functions, increased mortality, and increased rehospitalization rates [3,4,5]. In 2019, the European Working Group of Sarcopenia in Older People 2 (EWGSOP2) reported the importance of assessing both muscle mass and muscle quality as a new diagnostic standard for sarcopenia [6]. Hand grip strength is used to diagnose sarcopenia and can be used as a representative assessment of muscular strength in patients with heart failure [7]. Previously, a prospective observational study examined 148 male patients with heart failure and reported an association between low hand grip strength and decreased life expectancy [8]. In addition, another high-quality study reported low grip strength as an independent predictor of increased mortality and hospitalization in patients with heart failure [9]. These studies highlight the importance of prevention and improvement of muscular weakness in patients with heart failure.
Both the loss of muscle mass and the loss of muscle quality contribute to muscular weakness [10, 11]. The most common method for assessing muscle mass is the measurement of skeletal muscle mass index (SMI) by way of bio-impedance analysis (BIA) [11, 12]. In patients with heart failure, low SMI is associated with low grip strength [11], suggesting contribution of loss of muscle mass to overall muscular weakness. Recently, the segmental extracellular water (ECW)/intracellular water (ICW) ratio, which can be measured via BIA, has attracted attention as an index of muscle quality [13]. Skeletal muscles retain large amounts of water, which accounts for approximately 75% of muscle mass [14]. Muscle cell membranes divide the water content of skeletal muscles into ICW and ECW [15]. ICW reflects muscle cell mass, whereas ECW represents the sum of interstitial fluid and blood plasma in the extracellular space [16]. Therefore, an increase in the ECW/ICW ratio indicates a relative increase in non-contractile tissue [17]. Thus, the BIA method has the advantage of measuring both muscle mass and muscle quality simultaneously. This method has been utilized in previous studies to provide evidence of a relationship between increased ECW/ICW ratio and decreased strength. For example, a study reported that the thigh ECW/ICW ratio is negatively associated with knee extension strength in the elderly [17]. In addition, high thigh ECW/ICW ratio has been associated with decreased knee extensor strength in patients with knee osteoarthritis [18]. In patients with heart failure, however, it is unknown whether the ECW/ICW ratio is associated with muscle strength, and thus, it is not well understood whether poor muscle quality contributes to muscular weakness.
The purpose of this study was to assess the relationship among grip strength, SMI, and upper limb ECW/ICW ratio in patients with heart failure. If low hand grip strength is related not only to low SMI but also to increased upper limb ECW/ICW ratio, patients with heart failure will need to improve muscle quality as well as muscle mass progress their overall muscular strength.
Materials and methods
Study design
This study followed a cross-sectional design. The protocol was explained in detail to all participants in order to gather informed consent. This study was conducted in accordance with the strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement and followed ethical principles of the Declaration of Helsinki. It was approved by the ethics committees of Kure Kyosai Hospital (approval number: 2021–3).
Setting and patients
Study participants included patients admitted to the hospital with heart failure between January 2020 and July 2021. Heart failure was defined following the Framingham criteria [19]. Additional inclusion criteria included age (65 years or older) and ability to walk independently prior to admission. Patients were excluded if they suffered complications during hospitalization, had pacemakers inserted or had severe dementia, which was defined as a Revised Hasegawa’s Dementia Scale (HDS-R) score of 9 or below. The measurements were performed by the rehabilitation staff of the cooperating hospital. The sample size was calculated using G*Power version 3.1.9. A sample size analysis was performed with the 55 cases with the alpha value at 0.05, the statistical power at 0.8, and the effect size f2 greater than or equal to 0.15.
Demographic information
Patient demographic information included age, sex, body mass index (BMI), presence of family members in the same home, HDS-R score, Life Space Assessment (LSA) score, and degree of sarcopenia. HDS-R scores were categorized as follows: normal (21–30), suspected dementia (15–20), mild to moderate dementia (10–14), and severe dementia (less than or equal to 9) [20]. Life space was evaluated using the LSA developed by Baker et al. [21], in which a maximum of 120 points is assigned based on the existence or absence of activity, as well as the frequency and degree of independence in each life space level during the month prior to assessment. Accordingly, higher scores indicate a wider life space and/or greater independence. The degree of sarcopenia was determined based on the diagnostic criteria of the Asian Working Group for Sarcopenia [22].
Medical information
Medical information gathered from each patient included class of heart failure (based on the New York Heart Association classification system), presence or absence of medical history (including heart failure, coronary artery disease, valvar disease, hypertension, diabetes mellitus, dyslipidemia, atrial fibrillation, chronic renal failure, and stroke), pharmacotherapy (dobamin, dobutamine, noradrenaline, phosphodiesterase III inhibitors, diuretics, and beta blockers), Geriatric Nutritional Risk Index, brain natriuretic peptides, estimated glomerular filtration rate, and hemoglobin as blood data. Left ventricular ejection fraction was utilized as echocardiographic data.
SMI and ECW/ICW ratio
The BIA (S10, InBody, Tokyo, Japan) was used to measure SMI and ECW/ICW ratios. SMI and ECW/ICW ratios were measured on five body parts (left and right arms, trunk, and left and right legs) by thirty impedance measurements using six different frequencies (1, 5, 50, 250, 500, and 1000 kHz). Measurements were taken in the supine position with elbows extended and relaxed along the trunk. Touch-type electrodes were attached to each patient’s middle fingers and thumbs of both hands and between the heel and the ankle of each foot. Skeletal muscle mass was measured, and SMI (appendicular skeletal muscle mass/height2, kg/m2) was calculated as the sum of the lean soft tissues of the two upper and two lower limbs. The ECW/ICW ratios were measured in the right and left upper limbs.
Hand grip strength
Hand grip strength was measured using a grip strength meter (KK-5101; Takei Scientific Instruments, Tokyo, Japan) in the standing position with abduction of the upper limb to about 20 degrees from the body. Two measurements were taken on each side, and the maximum value (rounded to the nearest 0.1 kg) was used as the representative value [23].
Statistical analysis
All statistical analyses were performed using SPSS version 28 for Windows (IBM SPSS Japan, Tokyo, Japan). The upper limb ECW/ICW ratio as well as other variables was assessed for normality using the Shapiro–Wilk test. Associations of the upper limb ECW/ICW ratio with other variables were assessed using Pearson's correlation coefficient or Spearman's correlation coefficient. A hierarchical multiple regression analysis was conducted to identify factors associated with hand grip strength. The independent variables included demographic and medical information, SMI, and upper limb ECW/ICW ratio. Age, sex, BMI, and LSA were forced in as block 1. The other independent variables were entered in block 2 using a stepwise method. Factors related to hand grip strength were extracted separately from confounding factors (age, sex, BMI, and LSA). To account for multicollinearity, the threshold of the correlation coefficient between independent factors was set to 0.8, selecting those with a high correlation with the dependent variable [24]. The significance level was set at 5%.
Results
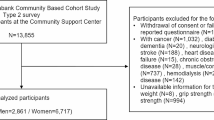
68 patients with heart failure initially met the inclusion criteria for this study. Of these, 9 had pacemakers inserted, 6 developed complications during hospitalization, and 2 had severe dementia. Thus, these 17 patients were excluded from the analyses. In total, 51 patients were analyzed (mean age 84.58 ± 7.18) (Table1).
In the correlation analyses, the upper limb ECW/ICW ratio was negative correlated with coronary artery disease (r = − 0.31, P < 0.05) and hand grip strength (r = − 0.27, P < 0.01). The upper limb ECW/ICW ratio was positively correlated with brain natriuretic peptide (r = 0.27, P < 0.05). The other variables were not significantly correlated with the upper limb ECW/ICW ratio (Table 2).
The final independent variables included: age, sex, BMI, presence of family members living in the same home as the subject, HDS-R score, LSA score, degree of sarcopenia, classification of heart failure (per guidelines of the New York Heart Association), presence or absence of medical history, geriatric nutritional risk index, number of brain natriuretic peptides, estimated glomerular filtration rate, hemoglobin level, left ventricular ejection fraction, SMI, and upper limb ECW/ICW ratio.
The results of the hierarchical multiple regression analysis are shown in Table 3. The significant associated factors extracted for hand grip strength included SMI and upper limb ECW/ICW ratio, independent of age, sex, BMI, and LSA scores. Standardized partial regression coefficients representing the magnitude of involvement of each independent variable were 0.33, − 0.16. The coefficient of determination adjusted for degrees of freedom (R2), representing the contribution rate of the regression equation, was 0.830.
Discussion
The purpose of this study was to assess the relationship among hand grip strength, SMI, and upper limb ECW/ICW ratio in patients with heart failure. Increased upper limb ECW/ICW ratio was significantly associated with decreased hand grip strength. In addition, hierarchical multiple regression analysis revealed that both SMI and upper limb ECW/ICW ratios were significantly associated with hand grip strength, independent of age, sex, BMI, and LSA score. Our results suggest that not only a decrease in skeletal muscle mass, but also low muscle quality (characterized by an increased ECW/ICW ratio) contribute to loss of hand grip strength in patients with heart failure. Therefore, improvement of both muscle quality and muscle mass is indicated to improve muscle strength in patients with heart failure.
An inverse relationship was discovered between an increase in the upper limb ECW/ICW ratio and a decrease in hand grip strength. Previous studies reported that both thigh and lower leg ECW/ICW ratios increase with aging, and thigh ECW/ICW ratio is negatively correlated with knee extensor strength and walking speed in the elderly subjects [15, 17]. Thigh ECW/ICW ratio has been significantly associated with knee extensor strength independent of age, sex, BMI, and skeletal muscle mass in elderly subjects [17]. Furthermore, Hiroka et al. reported that the ECW/ICW ratio was negatively related to hand grip strength in community-dwelling elderly [10]. Thus, it is recognized that the relative expansion of ECW to ICW in the muscle is a biomarker of low muscle quality [17]. Furthermore, an increase in the ECW/ICW ratio in patients with heart failure also contributes to muscle weakness, because it impacts muscle quality. This is significant because previous research has shown that hand grip strength is positively related to body weight and physical function [25]. Additionally, poor hand grip strength is associated with increased instances of malnutrition, cardiovascular disease, hip fractures, stroke, myocardial infarction, and mortality [26, 27]. Considering our findings and the existing literature on hand grip strength [25, 26, 28, 29], the upper limb ECW/ICW ratio may be an indicator of health conditions in elderly patients with heart failure.
The upper limb ECW/ICW ratio was positively correlated with brain natriuretic peptide, which is a marker of cardiac stress. This result suggests that the ECW/ICW ratio tends to increase in patients who have high cardiac stress. The detailed mechanisms why higher ECW/ICW ratio was associated with higher brain natriuretic peptide are unknown, but we propose the following possibility. BNP has various effects, and one of these is reduction of the cardiac stress by excreting excess sodium from the blood into the urine [30]. Thus, it is suggested that heart failure patients with high BNP may have higher sodium content. Elevated sodium content will increase osmotic pressure and elevate the ECW/ICW ratio through the movement of water from intracellular to extracellular. In fact, hyponatremia with increased body fluid volume (i.e., increased sodium content with further increased body fluid volume) is observed in patients with heart failure [31]. The main cause of heart failure is coronary artery disease [32]. The results of this study showed that heart failure patients with coronary artery disease had a lower ECW/ICW ratio. This result suggests that ECW/ICW ratio is likely to be increased in patients with heart failure due to causes other than coronary artery diseases. This possibility should be examined in detail in future studies.
The EWGSPO2 has reported the importance of assessing muscle mass and muscle quality in diagnosing sarcopenia [6]. The relative increase in non-contractile tissue leads to a decrease in muscle quality [33]. ECW and fat are the major non-contractile tissues of the muscle. Water mass can be measured using nuclear magnetic resonance imaging (NMRI) [29]. Previous studies using the NMRI have indicated that muscle water mass is significantly higher in older subjects than in younger subjects [34]. The intramuscular fat fraction is also one of the indexes of muscle quality and can be measured by echo intensity [35]. However, evaluation methods using NMRI and echo intensity have limitations, as they are challenging to implement and require advanced techniques. The measurement of BIA, which was used in this study, is a simple and easy way to measure ECW/ICW ratio simultaneously with muscle mass. Therefore, BIA is a simple and useful tool for the measurement of ECW/ICW ratio to assess muscle quality across various subjects, including patients with heart failure.
There are some limitations to this study. For example, we were unable to measure the ECW/ICW ratio of individual muscles. Instead, we utilized measurements of upper limb ECW/ICW ratios. Although this method is simple, muscles other than the finger flexors that produce hand grip strength were also targeted for measurement. Additionally, only hand grip strength was examined as an index of muscular strength. In the future, similar studies targeted for lower limb muscle strength, which is greatly related to motor function, should also be conducted.
In conclusion, we revealed that loss of hand grip strength in patients with heart failure is associated with not only a decrease in skeletal muscle mass, but also a decrease in muscle quality, characterized by an increased upper limb ECW/ICW ratio. Measurement of the ECW/ICW ratio using BIA is a simple and useful index of muscle quality in patients with heart failure.
References
Benjamin EJ, Muntner P, Alonso A, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Das SR, Delling FN, Djousse L, Elkind MSV, Ferguson JF, Fornage M, Jordan LC, Khan SS, Kissela BM, Knutson KL, Kwan TW, Lackland DT, Lewis TT, Lichtman JH, Longenecker CT, Loop MS, Lutsey PL, Martin SS, Matsushita K, Moran AE, Mussolino ME, O’Flaherty M, Pandey A, Perak AM, Rosamond WD, Roth GA, Sampson UKA, Satou GM, Schroeder EB, Shah SH, Spartano NL, Stokes A, Tirschwell DL, Tsao CW, Turakhia MP, VanWagner LB, Wilkins JT, Wong SS, Virani SS, American Heart Association Council on E, Prevention Statistics C, Stroke Statistics S (2019) Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation 139(10):e56–e528
Zhang Y, Zhang J, Ni W, Yuan X, Zhang H, Li P, Xu J, Zhao Z (2021) Sarcopenia in heart failure: a systematic review and meta-analysis. ESC Heart Fail 8(2):1007–1017
Long L, Mordi IR, Bridges C, Sagar VA, Davies EJ, Coats AJ, Dalal H, Rees K, Singh SJ, Taylor RS (2019) Exercise-based cardiac rehabilitation for adults with heart failure. Cochrane Database Syst Rev 1:CD003331
Konishi M, Kagiyama N, Kamiya K, Saito H, Saito K, Ogasahara Y, Maekawa E, Misumi T, Kitai T, Iwata K, Jujo K, Wada H, Kasai T, Nagamatsu H, Ozawa T, Izawa K, Yamamoto S, Aizawa N, Makino A, Oka K, Momomura SI, Matsue Y (2021) Impact of sarcopenia on prognosis in patients with heart failure with reduced and preserved ejection fraction. Eur J Prev Cardiol 28(9):1022–1029
Sato Y, Shiraishi H, Nakanishi N, Zen K, Nakamura T, Yamano T, Shirayama T, Matoba S (2020) Clinical significance of rectus femoris diameter in heart failure patients. Heart Vessels 35(5):672–680
Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyere O, Cederholm T, Cooper C, Landi F, Rolland Y, Sayer AA, Schneider SM, Sieber CC, Topinkova E, Vandewoude M, Visser M, Zamboni M, Writing Group for the European Working Group on Sarcopenia in Older P, the Extended Group for E (2019) Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing 48(4):601
Puthoff ML, Saskowski D (2013) Reliability and responsiveness of gait speed, five times sit to stand, and hand grip strength for patients in cardiac rehabilitation. Cardiopulm Phys Ther J 24(1):31–37
Izawa KP, Watanabe S, Osada N, Kasahara Y, Yokoyama H, Hiraki K, Morio Y, Yoshioka S, Oka K, Omiya K (2009) Handgrip strength as a predictor of prognosis in Japanese patients with congestive heart failure. Eur J Cardiovasc Prev Rehabil 16(1):21–27
Pavasini R, Serenelli M, Celis-Morales CA, Gray SR, Izawa KP, Watanabe S, Colin-Ramirez E, Castillo-Martinez L, Izumiya Y, Hanatani S, Onoue Y, Tsujita K, Macdonald PS, Jha SR, Roger VL, Manemann SM, Sanchis J, Ruiz V, Bugani G, Tonet E, Ferrari R, Volpato S, Campo G (2019) Grip strength predicts cardiac adverse events in patients with cardiac disorders: an individual patient pooled meta-analysis. Heart 105(11):834–841
Hioka A, Akazawa N, Okawa N, Nagahiro S (2021) Increased total body extracellular-to-intracellular water ratio in community-dwelling elderly women is associated with decreased handgrip strength and gait speed. Nutrition 86:111175
Fulster S, Tacke M, Sandek A, Ebner N, Tschope C, Doehner W, Anker SD, von Haehling S (2013) Muscle wasting in patients with chronic heart failure: results from the studies investigating co-morbidities aggravating heart failure (SICA-HF). Eur Heart J 34(7):512–519
Harada H, Kai H, Niiyama H, Nishiyama Y, Katoh A, Yoshida N, Fukumoto Y, Ikeda H (2017) Effectiveness of cardiac rehabilitation for prevention and treatment of sarcopenia in patients with cardiovascular disease—a retrospective cross-sectional analysis. J Nutr Health Aging 21(4):449–456
Yamada Y, Matsuda K, Bjorkman MP, Kimura M (2014) Application of segmental bioelectrical impedance spectroscopy to the assessment of skeletal muscle cell mass in elderly men. Geriatr Gerontol Int 14(Suppl 1):129–134
Mingrone G, Bertuzzi A, Capristo E, Greco AV, Manco M, Pietrobelli A, Salinari S, Heymsfield SB (2001) Unreliable use of standard muscle hydration value in obesity. Am J Physiol Endocrinol Metab 280(2):E365-371
Yamada Y, Ikenaga M, Takeda N, Morimura K, Miyoshi N, Kiyonaga A, Kimura M, Higaki Y, Tanaka H, Nakagawa H (2014) Estimation of thigh muscle cross-sectional area by single- and multifrequency segmental bioelectrical impedance analysis in the elderly. J Appl Physiol (1985) 116(2):176–182
Taniguchi M, Yamada Y, Fukumoto Y, Sawano S, Minami S, Ikezoe T, Watanabe Y, Kimura M, Ichihashi N (2017) Increase in echo intensity and extracellular-to-intracellular water ratio is independently associated with muscle weakness in elderly women. Eur J Appl Physiol 117(10):2001–2007
Yamada Y, Yoshida T, Yokoyama K, Watanabe Y, Miyake M, Yamagata E, Yamada M, Kimura M (2017) The extracellular to intracellular water ratio in upper legs is negatively associated with skeletal muscle strength and gait speed in older people. J Gerontol A Biol Sci Med Sci 72(3):293–298
Taniguchi M, Fukumoto Y, Yagi M, Yamagata M, Kobayashi M, Yamada Y, Kimura M, Ichihashi N (2021) Enhanced echo intensity and a higher extracellular water-to-intracellular water ratio are helpful clinical signs for detecting muscle degeneration in patients with knee osteoarthritis. Clin Rheumatol 40(10):4207–4215
Ho KK, Anderson KM, Kannel WB, Grossman W, Levy D (1993) Survival after the onset of congestive heart failure in Framingham Heart Study subjects. Circulation 88(1):107–115
Imai YHK (1994) The Revised Hasegawa’s Dementia Scale (HDS-R)-Evaluation of its usefulness as a screening test for dementia. Hong Kong J Psychiatry 4:20–24
Baker PS, Bodner EV, Allman RM (2003) Measuring life-space mobility in community-dwelling older adults. J Am Geriatr Soc 51(11):1610–1614
Chen LK, Woo J, Assantachai P, Auyeung TW, Chou MY, Iijima K, Jang HC, Kang L, Kim M, Kim S, Kojima T, Kuzuya M, Lee JSW, Lee SY, Lee WJ, Lee Y, Liang CK, Lim JY, Lim WS, Peng LN, Sugimoto K, Tanaka T, Won CW, Yamada M, Zhang T, Akishita M, Arai H (2020) Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J Am Med Dir Assoc 21(3):300–30.e2
Huang C, Niu K, Kobayashi Y, Guan L, Momma H, Cui Y, Chujo M, Otomo A, Guo H, Tadaura H, Nagatomi R (2013) An inverted J-shaped association of serum uric acid with muscle strength among Japanese adult men: a cross-sectional study. BMC Musculoskelet Disord 14:258
Umehara T, Katayama N, Tsunematsu M, Kakehashi M (2020) Factors affecting hospital readmission heart failure patients in Japan: a multicenter retrospective cohort study. Heart Vessels 35(3):367–375
Sayer AA, Kirkwood TB (2015) Grip strength and mortality: a biomarker of ageing? Lancet 386(9990):226–227
Denk K, Lennon S, Gordon S, Jaarsma RL (2018) The association between decreased hand grip strength and hip fracture in older people: A systematic review. Exp Gerontol 111:1–9
Zhang XS, Liu YH, Zhang Y, Xu Q, Yu XM, Yang XY, Liu Z, Li HZ, Li F, Xue CY (2017) Handgrip strength as a predictor of nutritional status in chinese elderly inpatients at hospital admission. Biomed Environ Sci 30(11):802–810
Nacul LC, Mudie K, Kingdon CC, Clark TG, Lacerda EM (2018) Hand grip strength as a clinical biomarker for ME/CFS and disease severity. Front Neurol 9:992
Forrest KYZ, Williams AM, Leeds MJ, Robare JF, Bechard TJ (2018) Patterns and Correlates of Grip Strength in Older Americans. Curr Aging Sci 11(1):63–70
Burke MA, Cotts WG (2007) Interpretation of B-type natriuretic peptide in cardiac disease and other comorbid conditions. Heart Fail Rev 12(1):23–36
Klein L, O’Connor CM, Leimberger JD, Gattis-Stough W, Piña IL, Felker GM, Adams KF Jr, Califf RM, Gheorghiade M (2005) Lower serum sodium is associated with increased short-term mortality in hospitalized patients with worsening heart failure: results from the Outcomes of a Prospective Trial of Intravenous Milrinone for Exacerbations of Chronic Heart Failure (OPTIME-CHF) study. Circulation 111(19):2454–2460
Lala A, Desai AS (2014) The role of coronary artery disease in heart failure. Heart Fail Clin 10(2):353–365
Kent-Braun JA, Ng AV, Young K (2000) Skeletal muscle contractile and noncontractile components in young and older women and men. J Appl Physiol (1985) 88(2):662–668
Azzabou N, Hogrel JY, Carlier PG (2015) NMR based biomarkers to study age-related changes in the human quadriceps. Exp Gerontol 70:54–60
Nakano I, Hori H, Fukushima A, Yokota T, Kinugawa S, Takada S, Yamanashi K, Obata Y, Kitaura Y, Kakutani N, Abe T, Anzai T (2020) Enhanced echo intensity of skeletal muscle is associated with exercise intolerance in patients with heart failure. J Card Fail 26(8):685–693
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Umehara, T., Kaneguchi, A., Kawakami, W. et al. Association of muscle mass and quality with hand grip strength in elderly patients with heart failure. Heart Vessels 37, 1380–1386 (2022). https://doi.org/10.1007/s00380-022-02046-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00380-022-02046-7