
Abstract
Introduction
Active surveillance, primary retroperitoneal lymph node dissection and adjuvant chemotherapy are treatment options for high-risk clinical stage (CS) I nonseminomatous germ cell testicular tumors (NSGCT). Since 1981, at Princess Margaret Hospital, Toronto, initial active surveillance with treatment delayed until relapse has been the preferred management option for all CS I NSGCT, regardless of baseline risk of relapse which has allowed us to better define and assess the natural history of high-risk tumors.
Materials and methods
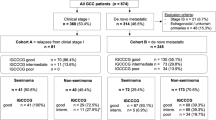
From 1981 to 2005, 371 patients with CS I NSGCT were placed on an active surveillance protocol. Recurrence patterns, predictors of relapse, disease specific (DS) and overall survival (OS) were measured. Outcomes were stratified into two cohorts by their time of diagnosis [initial, 157 patients (1981–1992); recent, 214 patients (1993–2005)].
Results
Median follow-up was 6.3 years. Median time to relapse was 7.1 months. Lympho-vascular invasion (P < 0.0001) and pure embryonal carcinoma (P = 0.02) were independent predictors of relapse. In the initial cohort, 66/157 (42.0%) were high-risk and 36/66 (54.5%) relapsed versus 17/91 (18.7%) low-risk (P < 0.0001). In the recent cohort, 59/214 (27.6%) patients were high-risk and 29/59 (49.2%) recurred, versus 22/155 (14.2%) low-risk (P < 0.0001). The 5-year DSS and OS were 99.2 and 98.2%, respectively.
Conclusions
Nonrisk adapted active surveillance is the preferred management strategy for all CS I NSGCT patients including those at high-risk, providing near 100% cure rate with reduced overall treatment burden. Approximately half of the high-risk patients will be spared unnecessary treatment with little or no increase risk.
Similar content being viewed by others


References
Albers P, Albrecht W, Algaba F et al (2005) Guidelines on testicular cancer. Eur Urol 48:885
Huyghe E, Matsuda T, Thonneau P (2003) Increasing incidence of testicular cancer worldwide: a review. J Urol 170:5
Choueiri TK, Stephenson AJ, Gilligan T et al (2007) Management of clinical stage I nonseminomatous germ cell testicular cancer. Urol Clin North Am 34:137
Stephenson AJ, Sheinfeld J (2005) Management of patients with low-stage nonseminomatous germ cell testicular cancer. Curr Treat Options Oncol 6:367
Colls BM, Harvey VJ, Skelton L et al (1999) Late results of surveillance of clinical stage I nonseminoma germ cell testicular tumours: 17 years’ experience in a national study in New Zealand. BJU Int 83:76
Segal R (2006) Surveillance programs for stage I nonseminomatous germ cell tumors of the testis. Urol Oncol 24:68
Pont J, Holtl W, Kosak D et al (1990) Risk-adapted treatment choice in stage I nonseminomatous testicular germ cell cancer by regarding vascular invasion in the primary tumor: a prospective trial. J Clin Oncol 8:16
Sogani PC, Perrotti M, Herr HW et al (1998) Clinical stage I testis cancer: long-term outcome of patients on surveillance. J Urol 159:855
Al Ghamdi AM, Jewett MA (2005) Stage I nonseminomatous germ cell tumors: the case for management by risk stratification. Can J Urol 12(Suppl 1):62
Albers P, Siener R, Kliesch S et al (2003) Risk factors for relapse in clinical stage I nonseminomatous testicular germ cell tumors: results of the German Testicular Cancer Study Group trial. J Clin Oncol 21:1505
Peckham MJ, Barrett A, Husband JE et al (1982) Orchidectomy alone in testicular stage I non-seminomatous germ-cell tumours. Lancet 2:678
Sturgeon JF, Jewett MA, Alison RE et al (1992) Surveillance after orchidectomy for patients with clinical stage I nonseminomatous testis tumors. J Clin Oncol 10:564
Nicolai N, Pizzocaro G (1995) A surveillance study of clinical stage I nonseminomatous germ cell tumors of the testis: 10-year follow-up. J Urol 154:1045
Roeleveld TA, Horenblas S, Meinhardt W et al (2001) Surveillance can be the standard of care for stage I nonseminomatous testicular tumors and even high risk patients. J Urol 166:2166
Pizzocaro G, Zanoni F, Salvioni R et al (1987) Difficulties of a surveillance study omitting retroperitoneal lymphadenectomy in clinical stage I nonseminomatous germ cell tumors of the testis. J Urol 138:1393
Nicolai N, Miceli R, Artusi R et al (2004) A simple model for predicting nodal metastasis in patients with clinical stage I nonseminomatous germ cell testicular tumors undergoing retroperitoneal lymph node dissection only. J Urol 171:172
Maroto P, Garcia del Muro X, Aparicio J et al (2005) Multicentre risk-adapted management for stage I non-seminomatous germ cell tumours. Ann Oncol 16:1915
Divrik RT, Akdogan B, Ozen H et al (2006) Outcomes of surveillance protocol of clinical stage I nonseminomatous germ cell tumors-is shift to risk adapted policy justified? J Urol 176:1424
Peckham MJ, Barrett A, Horwich A et al (1983) Orchiectomy alone for Stage I testicular non-seminoma. A progress report on the Royal Marsden Hospital study. Br J Urol 55:754
Albers P, Siener R, Hartmann M et al (1999) Risk factors for relapse in stage I non-seminomatous germ-cell tumors: preliminary results of the German Multicenter Trial. German Testicular Cancer Study Group. Int J Cancer 83:828
Read G, Stenning SP, Cullen MH et al (1992) Medical Research Council prospective study of surveillance for stage I testicular teratoma. Medical Research Council Testicular Tumors Working Party. J Clin Oncol 10:1762
Vergouwe Y, Steyerberg EW, Eijkemans MJ et al (2003) Predictors of occult metastasis in clinical stage I nonseminoma: a systematic review. J Clin Oncol 21:4092
Sharir S, Jewett MA, Sturgeon JF et al (1999) Progression detection of stage I nonseminomatous testis cancer on surveillance: implications for the followup protocol. J Urol 161:472
Lowe BA (1993) Surveillance versus nerve-sparing retroperitoneal lymphadenectomy in stage I nonseminomatous germ-cell tumors. Urol Clin North Am 20:75
Foster RS, Donohue JP (2000) Retroperitoneal lymph node dissection for the management of clinical stage I nonseminoma. J Urol 163:1788
Heidenreich A, Sesterhenn IA, Mostofi FK et al (1998) Prognostic risk factors that identify patients with clinical stage I nonseminomatous germ cell tumors at low risk and high risk for metastasis. Cancer 83:1002
Albers P (2007) Management of stage I testis cancer. Eur Urol 51:34
Price P, Hogan SJ, Bliss JM et al (1990) The growth rate of metastatic nonseminomatous germ cell testicular tumours measured by marker production doubling time. II. Prognostic significance in patients treated by chemotherapy. Eur J Cancer 26:453
Boyer MJ, Cox K, Tattersall MH et al (1997) Active surveillance after orchiectomy for nonseminomatous testicular germ cell tumors: late relapse may occur. Urology 50:588
Rustin GJ, Mead GM, Stenning SP et al (2007) Randomized trial of two or five computed tomography scans in the surveillance of patients with stage I nonseminomatous germ cell tumors of the testis: Medical Research Council Trial TE08, ISRCTN56475197—the National Cancer Research Institute Testis Cancer Clinical Studies Group. J Clin Oncol 25:1310
Schmoll HJ, Souchon R, Krege S et al (2004) European consensus on diagnosis and treatment of germ cell cancer: a report of the European Germ Cell Cancer Consensus Group (EGCCCG). Ann Oncol 15:1377
Stephenson AJ, Bosl GJ, Bajorin DF et al (2005) Retroperitoneal lymph node dissection in patients with low stage testicular cancer with embryonal carcinoma predominance and/or lymphovascular invasion. J Urol 174:557
Stephenson AJ, Bosl GJ, Motzer RJ et al (2005) Retroperitoneal lymph node dissection for nonseminomatous germ cell testicular cancer: impact of patient selection factors on outcome. J Clin Oncol 23:2781
Baniel J, Foster RS, Einhorn LH et al (1995) Late relapse of clinical stage I testicular cancer. J Urol 154:1370
Yoon GH, Stein JP, Skinner DG (2005) Retroperitoneal lymph node dissection in the treatment of low-stage nonseminomatous germ cell tumors of the testicle: an update. Urol Oncol 23:168
Jewett MA, Kong YS, Goldberg SD et al (1988) Retroperitoneal lymphadenectomy for testis tumor with nerve sparing for ejaculation. J Urol 139:1220
Donohue JP, Thornhill JA, Foster RS et al (1993) Primary retroperitoneal lymph node dissection in clinical stage A non-seminomatous germ cell testis cancer. Review of the Indiana University experience 1965–1989. Br J Urol 71:326
Donohue JP, Foster RS, Rowland RG et al (1990) Nerve-sparing retroperitoneal lymphadenectomy with preservation of ejaculation. J Urol 144:287
Foster RS, Roth BJ (1998) Clinical stage I nonseminoma: surgery versus surveillance. Semin Oncol 25:145
Hermans BP, Sweeney CJ, Foster RS et al (2000) Risk of systemic metastases in clinical stage I nonseminoma germ cell testis tumor managed by retroperitoneal lymph node dissection. J Urol 163:1721
Sternberg CN (1998) The management of stage I testis cancer. Urol Clin North Am 25:435
Amato RJ, Ro JY, Ayala AG et al (2004) Risk-adapted treatment for patients with clinical stage I nonseminomatous germ cell tumor of the testis. Urology 63:144
Link RE, Allaf ME, Pili R et al (2005) Modeling the cost of management options for stage I nonseminomatous germ cell tumors: a decision tree analysis. J Clin Oncol 23:5762
Travis LB, Fossa SD, Schonfeld SJ et al (2005) Second cancers among 40, 576 testicular cancer patients: focus on long-term survivors. J Natl Cancer Inst 97:1354
Travis LB, Andersson M, Gospodarowicz M et al (2000) Treatment-associated leukemia following testicular cancer. J Natl Cancer Inst 92:1165
Hao D, Seidel J, Brant R et al (1998) Compliance of clinical stage I nonseminomatous germ cell tumor patients with surveillance. J Urol 160:768
Conflict of interest statement
There is no actual or potential conflict of interest in relation to this article whatsoever.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kakiashvili, D.M., Zuniga, A. & Jewett, M.A.S. High risk NSGCT: case for surveillance. World J Urol 27, 441–447 (2009). https://doi.org/10.1007/s00345-009-0453-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-009-0453-6