
Abstract
To assess the impact of the COVID-19 pandemic on the training of rheumatology trainees. We conducted an observational cross-sectional study using an online survey-based questionnaire sent to rheumatology trainees in India. Rheumatology trainees from India, including DM/DNB residents and fellows, were included. A total of 78 trainees from 24 institutes in 12 states participated in the study. An overwhelming majority of residents (84%) felt COVID-19 Pandemic Negatively impacted their residency and their Physical (65%), Mental (74%) and Social well-being (80%); 79% of trainees felt burnt out. Majority of trainees felt the pandemic negatively impacted their training with clinical teaching (91%), Clinical examination skills (74%), current (80%) and future (70%) research opportunities suffering during the pandemic. Most had significant reduction in the overall footfall (72%) of patients in rheumatology including OPD (77%) and indoor (67%) admissions along with academics (35%), procedures (66%) and exposure to musculoskeletal ultrasound (71%). Almost 60% and 40% of trainees had OPDs, and indoor admissions stopped during COVID-19 pandemic of these 20% had OPDs, and Admissions closed for more than 6 months. 85% of participants had one or the other psychological symptoms with almost half experiencing anxiety (44%), low mood (47%) or lack of sleep (41%). We found The COVID-19 Pandemic has significantly affected the physical, social and mental well-being of Rheumatology trainees. Academic and clinical training reduced, current and future Research became difficult, disruptions in OPDs and Admissions, recurrent COVID postings and reduction in patient footfall, procedures and MSK-US have been detrimental to trainees.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The COVID-19 (coronavirus disease 2019) pandemic has proven to be relentlessly challenging, leading to an unprecedented public health crisis impacting healthcare systems, healthcare workers, and communities substantively. The situation has been starker in developing countries with understaffed and overburdened healthcare. COVID-19 has been the great disrupter of our times, with almost all aspects of healthcare being severely affected, from medical education to clinical practice and research. The sudden transition from conventional in-person teaching to virtual training was not smooth, a number of social, economic, cultural, and mental factors interfered with full utilization and acclimatization of the virtual education platform initially. Stress from the multiple covid duties, self-isolations, and quarantines further added to the woes of trainees. A study revealed significantly higher rates of stress and burnout in COVID-19 exposed physician trainees compared to non-exposed trainees [1]. The stress was specially higher in female and unmarried trainees [2]. Planned interventions were severely disrupted in the pandemic, impacting intervention-based branches dearly.
COVID 19 Global Rheumatology Alliance trainee survey of 302 rheumatology trainees across different institutes depicted that sudden and unexpected changes in health services during the COVID-19 pandemic had significantly impacted the clinical training, research opportunities and health and well-being of rheumatology trainees [3]. The current study aims to gauge the magnitude of the effect the pandemic had on Rheumatology training (including the impact on clinical, academic and research activity) in India, their physical, mental and social wellbeing during the pandemic and the perceived changes in Rheumatology training and care during the pandemic from the trainee’s view.
Methods
Survey design and dissemination
Using an online survey platform (Google form), we conducted an observational cross-sectional study across India. A questionnaire was designed and distributed to all the current trainees and fellows pursuing their course (DM, DNB and Fellowship) in rheumatology. Candidates who had cleared their final examination before 2020 were excluded from the study population. The listed authors designed the questionnaire collaboratively regarding the impact of COVID-19 on rheumatology trainees in India. The survey questionnaire incorporated questions on impact on rheumatology training and research, patient care and trainee wellness. In addition, seven questions were asked to evaluate telemedicine status, vaccination coverage and covid exposure history among trainees. The questionnaire was generated by a web-based platform (Google Form) and distributed to all the participants a link on social media platforms (e.g., WhatsApp, Telegram and Email) after proper consent and the responses were received over 6 months.
Eligibility criteria
Participant selection was made on adult and paediatric rheumatology trainees from different institutes in India. Those included had not completed their rheumatology training before 2021, were older than 18, and consented to participate in the survey. This survey was conducted by pure voluntary engagement of the participants and did not include personal identifiers, protected health information or incentives. Convenience sampling was used, so the sample size was not calculated.
Ethical statement
The protocol was cleared by the Institutional Ethics Committee of King George’s Medical University protocol no. VI-PGTSC-IIA/P48 dated 27.10.2021.
Respondents were required to verify their consent before they began the survey to understand the nature and value of the questions.
Data collection and statistical analysis
All respondents were included in the analysis. Data were represented as absolute numbers and percentages. The questionnaire contains 5-point Likert scales, multiple-choice questions, and some leading questions. Leading inquiries were replied to in ‘yes/no’ format, and if ‘yes’, they must specify their answer. 5-point Likert scale was based on whether it has a positive and negative impact, in terms of agreeing and disagreeing to that question. In addition, the extent of each component is specified (i.e., Agree and strongly agree). A neutral response was kept for the no impact component of the Likert scale.
Data are presented using descriptive statistics and processed using SPSSv23. Descriptive statistics were performed by calculating measures of central tendency for quantitative variables and using counts and percentages for qualitative and nominal variables.
Results
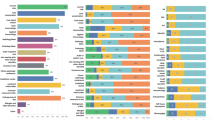
Seventy-eight trainees from 24 institutes in 12 states participated in the study. The mean age of the participants was 31, with 70% of trainees being male and 30% females. 56 (70%) participants were DM students, 15 (19%) were DNB students, five fellowship students and 2 Non-academic Senior Residents. An overwhelming majority of residents (84%) felt COVID-19 Pandemic negatively impacted their residency and their physical (65%), mental (74%) and social well-being (80%). 79% of trainees felt burnt out due to the pandemic. The majority of trainees felt the pandemic negatively impacted their training, with the majority of trainees feeling their clinical teaching(91%), clinical examination skills (74%), current(80%) and future(70%) research opportunities suffered during the pandemic (Fig. 1).

Impact on clinical training and trainee wellness are assessed by this questionnaire format. A five-point Likert scale response of trainees for each of the questions are represented as a horizontal bar diagram. Each bar represents color coded segment for different responses such as strongly agree (dark green), agree (light green), neutral (light brown), disagree (brown) and strongly disagree (red). Percentage of trainee’s response are expressed in numbers in each segment. Majority of them are responded in favor of the negative effect of COVID in their personal as well as professional life
Most residents reported reduction of both indoor admission and out-patient department (OPD) registrations (99%) with majority claiming a significant reduction (Reduction to less than half of pre-COVID levels) (72%). Similar overall and significant reduction in patients attending OPD (100% & 77%) and indoor admissions (99% & 67%) was reported. Trainees also reported an overall and significant reduction in academics (85% & 35%), procedures and interventions including biopsies and intra-articular injections (97% & 66%) and exposure to musculoskeletal ultrasound (96% & 71%) (Fig. 2). Almost 60% and 40% of trainees had their OPDs and indoor admissions stopped during the COVID-19 pandemic. Of these, 20% had their OPDs and Admissions closed for more than 6 months (Fig. 3).

Patient care services and learning during COVID times are represented in a horizontal bar diagram with a five-point Likert scale response. Questions regarding IPD, OPD, access to health care, MSK ultrasound, Daycare procedure and academic strength are expressed in separate row with different color-coded bars. Each bar contains percentage of response in each color-coded segment such as strongly reduced (pink), moderately reduced (light pink), mildly reduced (light green), not reduced (green) and increased (dark green). Most of them agreed that COVID pandemic has restricted learning opportunity and patient care services. Significantly reduced (reduced less than half of pre-COVID), moderately reduced (reduced by 25–50%) mildly reduced (reduced by no more the 25%) not reduced

Duration of restricted access to health care services in institutes are observed with varying grades. Restriction to OPD as well as IPD services and deployment of trainees in COVID postings are depicted as a horizontal bar diagram with different color labels. Durations are mentioned as No restriction/duty (green), < 1 months (light pink), 1–3 months (light brown), 3–6 months (light red) and > 6 months (red)
85% of the participants had one or the other psychological symptoms, with almost half experiencing anxiety (44%), low mood (47%) or lack of sleep (41%); 85% were concerned about their family members being infected, and 40% had lost a close relative to COVID. 91% of the trainee were posted in COVID duties, 2/3rd of them in ICUs, 50% being posted for 1–3 months and 20% more than 3 months, a quarter of trainees got infected during their duties (COVID and Non-COVID), and though most had asymptomatic to mild COVID, 15% still had moderate to severe COVID (Fig. 4).

Pie charts are made from separate multiple choice question responses to understand the attitude of trainees towards different aspects of training. A Pie chart represents personal difficulties created by COVID related duties; B different causes for retraction of new research; C type of COVID posting; D exposure to COVID infection; and E severity of COVID infection across trainees
Teleconsultation was started by the institutes majorly in post COVID-19 era (54%). The teleconsultation platform existed as a model of patient follow-up in 29% of institutes before the COVID outbreak, but a significant proportion (15%) was unable to provide teleconsultation services in the COVID era also. The majority of teleconsultations (80%) were supervised by senior faculty members according to case-to-case basis, whether partial(50%) or full (30%) engagement was necessary (Fig. 5). Opinions regarding satisfaction with teleconsultation services were mixed, with 54% not truly satisfied.

Telehealth services during COVID as a part of healthcare delivery are expressed in separate pie charts. A Teleconsultation status in pre and post COVID era; B supervision status of teleconsultation by senior faculty members; and C trainee satisfaction regarding teleconsultation services
Discussion
The study of 78 rheumatology trainees across India showed a substantial impact of COVID 19 on rheumatological training and trainees’ wellbeing. Different domains of rheumatology training were affected with a significant effect on patient care.
Impact on clinical training and patient care
Most trainees agreed that the COVID-19 pandemic had negatively impacted their rheumatology training. Though the recommendation and guidelines for rheumatology training vary across countries but most countries advocate appropriate patient exposure, ample research opportunities and adequate laboratory experience, MSK ultrasound and necessary interventions are essential for a good training experience [4, 5]. Different studies in other specialities across the globe reported a higher number of redeployment to a non-specialist role with an increase in working hours and often without proper personal protective measures [6, 7]. A paediatric gastroenterology residents survey [8], reported a significant reduction in clinical training (52%), research projects(46%), and procedural confidence (41%), which was similar to what we have observed in our study. Many rheumatology trainees were reassigned to new roles with mandatory COVID duty during their tenure. A survey conducted by allergy & immunology trainees in USA found that 12% of fellows in training were reassigned to COVID-19 duty, and a majority of them were concerned about the clinical experience they would gain during the fellowship [9]. In our study, most trainees were posted for 1–3 months in COVID duty in between specialists’ duty; however, a few had to work in covid up to 6 months, accounting for almost 20% of their total training duration. Outpatient and inpatient services were transiently hampered due to significant disruption in patient care services [7]. New research opportunities and ongoing research projects were affected in terms of acquisition of funds, reduction in sample size, and ability of physician to continue research after a significant increase in working hours [10,11,12].
Impact on trainee wellness
In our survey, most of the Rheumatology trainee agreed that the COVID pandemic had negatively impacted their general well-being. A global trainee survey of 1420 trainees noted that a strong predictor of physician burnout was related to more exposure to COVID-19 patients and having a COVID-positive colleague triggers emotional concern and stress [13]. Trainees in Saudi Arabia during the COVID pandemic reported low mood and anxiety [14]. Decreased clinical experience, reduced case volume, disrupted education activities and deteriorated mental health are significant concerns in the Trainee survey [15]. Though long-term effects of negative psychological impacts are not mentioned but physicians' burnout generates depression, suicidal ideation, substance abuse, relationship difficulties, decreased productivity, work dissatisfaction, medical errors and suboptimal patient care [16]. A global Rheumatology trainee survey showed that physician stress (> 75%) and burnouts (> 50%) were quite common among trainees [3]. Studies from the subcontinent echoed similar concerns [17] (Table 1).
Telehealth
The concept of telemedicine has evolved at an unprecedented pace over the last few years with the advent of the pandemic. This concept was implemented in several institutes across globe during lockdown to maintain the platform for remote patient interaction [18,19,20,21]. Teleconsultation is technology-intensive, and its use has been limited by lack of access in the developing world. As echoed in our survey findings, lack of training regarding telehealth protocols, and difficulty in a comprehensive assessment of patient status are current limitations.
Virtual education
Virtual conferences and multiple virtual educational resources were a boon to the trainees during the pandemic, virtual education allow easy access across regional and national boundaries and are less intimidating to students compared to their in-person counterparts although with lesser interaction and attention [34]. International collaborations such as the Global Rheumatology Alliance has shown how the pandemic bought us together as a community during times of adversity to fight an unknown enemy.
The way forward
The pandemic has helped streamline online education and conferences, we need to understand the lacunae/deficiencies and improve upon them to make the virtual learning process more immersive. Institutions need to devise/improve virtual examination and teleconsultation protocols to ensure future pandemics have a ready mechanism with minimal disruptions in patient care [34]. International Grand Rounds, greater collaborations and Virtual mentors would further help in improving trainee education and understanding.
Limitations
The Questionnaire was not independently validated though it was based on the Global Rheumatology alliance questionnaire with country and context-specific modifications.
We tried to include all the trainees in India but could manage 75% of those who were under training in the survey period. We did not ask questions on the effect of digital education and virtual conferences and no questions on cross-speciality interactions were asked.
Conclusions
The COVID-19 Pandemic has completely altered the status quo for rheumatology trainees and has affected their physical, social and mental wellbeing. Academic and clinical training has been significantly hampered, and conducting current, and future research has become difficult. Significant disruptions in OPDs, IPDs, daycare procedures and musculoskeletal ultrasound have adversely impacted training and patient care. Recurrent exhaustive COVID postings and redeployment increased burnout and psychosocial stress on trainees. New adaptation in patient care services such as telemedicine was welcomed, but the satisfaction with teleconsultation is low, and a lot needs to be done for proper acclimatisation with the system.
Data availability
Data are available upon reasonable request by any qualified researchers who engage in rigorous, independent scientific research, and will be provided following review and approval of a research proposal and Statistical Analysis Plan (SAP) and execution of a Data Sharing Agreement (DSA). All data relevant to the study are included in the article.
References
Enujioke SC, McBrayer K, Soe KC, Imburgia TM, Robbins C (2021) Impact of COVID-19 on post graduate medical education and training. BMC Med Educ 21(1):580
Kannampallil TG, Goss CW, Evanoff BA, Strickland JR, McAlister RP, Duncan J (2020) Exposure to COVID-19 patients increases physician trainee stress and burnout. PLoS ONE 15(8):e0237301
Young K, Yeoh SA, Putman M, Sattui S, Conway R, Graef E et al (2022) The impact of COVID-19 on rheumatology training—results from the COVID-19 Global Rheumatology Alliance trainee survey. Rheumatol Adv Pract 6(1):rkac001
Core-Curriculum-Outline.pdf [Internet]. [cited 22 May 2022]. Available from: https://www.rheumatology.org/Portals/0/Files/Core-Curriculum-Outline.pdf
Woolf AD. Training Rheumatologists in Europe.19.
Hope C, Reilly JJ, Griffiths G, Lund J, Humes D (2021) The impact of COVID-19 on surgical training: a systematic review. Tech Coloproctology 25(5):505–520
An TW, Henry JK, Igboechi O, Wang P, Yerrapragada A, Lin CA et al (2020) How are orthopaedic surgery residencies responding to the COVID-19 pandemic? An assessment of resident experiences in cities of major virus outbreak. J Am Acad Orthop Surg. https://doi.org/10.5435/JAAOS-D-20-00397
Irastorza LE, Hopson P, Ta A, Kemme S, Mallon D, Lee CK (2021) The impact of COVID-19 on job prospects and educational training for pediatric gastroenterology fellows. J Pediatr Gastroenterol Nutr 72:514–519
Kahwash BM, Deshpande DR, Guo C, Panganiban CM, Wangberg H, Craig TJ (2021) Allergy/immunology trainee experiences during the COVID-19 pandemic: AAAAI work group report of the fellows-in-training committee. J Allergy Clin Immunol Pract 9(1):1-6.e1
The Impact of the COVID-19 Pandemic on the Extramural Scientific Workforce—outcomes from an NIH-Led Survey—NIH Extramural Nexus [Internet]. [cited 25 May 2022]. Available from: https://nexus.od.nih.gov/all/2021/03/25/the-impact-of-the-covid-19-pandemic-on-the-extramural-scientific-workforce-outcomes-from-an-nih-led-survey/
Squazzoni F, Bravo G, Grimaldo F, Garcıa-Costa D, Farjam M, Mehmani B. Only Second-Class Tickets for Women in the COVID-19 Race. A Study on Manuscript Submissions and Reviews in 2329 Elsevier Journals [Internet]. Rochester, NY: Social Science Research Network; 2020 Oct [cited 25 May 2022]. Report No.: 3712813. Available from: https://papers.ssrn.com/abstract=3712813
Breuning M, Fattore C, Ramos J, Scalera J. Gender, parenting, and scholarly productivity during the global pandemic. 2020 Jul 21 [cited 2022 May 25]; Available from: https://preprints.apsanet.org/engage/apsa/article-details/5f16fc5660b4ad001212f977
Cravero AL, Kim NJ, Feld LD, Berry K, Rabiee A, Bazarbashi N et al (2021) Impact of exposure to patients with COVID-19 on residents and fellows: an international survey of 1420 trainees. Postgrad Med J 97(1153):706–715
Chen SY, Lo HY, Hung SK (2021) What is the impact of the COVID-19 pandemic on residency training: a systematic review and analysis. BMC Med Educ 15(21):618
Cubitt LJ, Im YR, Scott CJ, Jeynes LC, Molyneux PD (2021) Beyond PPE: a mixed qualitative–quantitative study capturing the wider issues affecting doctors’ well-being during the COVID-19 pandemic. BMJ Open 11(3):e050223
De Hert S (2020) Burnout in healthcare workers: prevalence, impact and preventative strategies. Local Reg Anesth 28(13):171–183
Sharma D, Bhaskar S. Addressing the Covid-19 Burden on Medical Education and Training: The Role of Telemedicine and Tele-Education During and Beyond the Pandemic. Front Public Health [Internet]. 2020 [cited 23 May 2022];8. Available from: https://www.frontiersin.org/article/https://doi.org/10.3389/fpubh.2020.589669
Jethwa H, Abraham S (2021) Training the trainees: COVID-19 and rheumatologists of the future. Clin Med 21(1):e94–e95
Zhang Y, Wang J, Zhao L, Xiao J, Shi Z (2021) Online management of rheumatoid arthritis during COVID-19 pandemic. Ann Rheum Dis 80:e4–e4
López-Medina C, Escudero A, Collantes-Estevez E (2020) COVID-19 pandemic: an opportunity to assess the utility of telemedicine in patients with rheumatic diseases. Ann Rheum Dis 80:e50 (annrheumdis-2020-218008)
Kirby T (2020) Rheumatologists rapidly adjust patient care during COVID-19 pandemic. Lancet Rheumatol 2(5):e258
Chang DG, Park JB, Baek GH, Kim HJ, Bosco A, Hey HWD et al (2020) The impact of COVID-19 pandemic on orthopaedic resident education: a nationwide survey study in South Korea. Int Orthop 10:1–8
Mishra D, Nair AG, Gandhi RA, Gogate PJ, Mathur S, Bhushan P et al (2020) The impact of COVID-19 related lockdown on ophthalmology training programs in India—outcomes of a survey. Indian J Ophthalmol 68(6):999–1004
Nguyen HT, Do BN, Pham KM, Kim GB, Dam HTB, Nguyen TT et al (2020) Fear of COVID-19 scale—associations of its scores with health literacy and health-related behaviors among medical students. Int J Environ Res Public Health 17(11):4164
Compton S, Sarraf-Yazdi S, Rustandy F, Kumar Radha Krishna L (2020) Medical students’ preference for returning to the clinical setting during the COVID-19 pandemic. Med Educ. https://doi.org/10.1111/medu.14268
Khanna RC, Honavar SG, Metla AL, Bhattacharya A, Maulik PK (2020) Psychological impact of COVID-19 on ophthalmologists-in-training and practising ophthalmologists in India. Indian J Ophthalmol 68(6):994–998
Li Y, Wang Y, Jiang J, Valdimarsdóttir UA et al (2021) Psychological distress among health professional students during the COVID-19 outbreak. Psychol Med. 51(11):1952–1954. https://doi.org/10.1017/S0033291720001555
Liu J, Zhu Q, Fan W, Makamure J, Zheng C, Wang J. Online mental health survey in a Medical College in China During the COVID-19 Outbreak. Front Psychiatry [Internet]. 2020 [cited 23 May 2022];11. Available from: https://www.frontiersin.org/article/https://doi.org/10.3389/fpsyt.2020.00459
Abbasi S, Ayoob T, Malik A, Memon SI (2020) Perceptions of students regarding E-learning during Covid-19 at a private medical college. Pak J Med Sci. 36(COVID19-S4):S57-61
Foong WS, Teo HLT, Wang DHB, Loh SYJ (2020) Challenges and adaptations in training during pandemic COVID-19: observations by an orthopedic resident in Singapore. Acta Orthop 91(5):562–566
Sethi BA, Sethi A, Ali S, Aamir HS (2020) Impact of coronavirus disease (COVID-19) pandemic on health professionals. Pak J Med Sci 36(COVID19-S4):S6-11
Ikhlaq A, Bint-E-Riaz H, Bashir I, Ijaz F (2020) Awareness and attitude of undergraduate medical students towards 2019-novel corona virus. Pak J Med Sci. 36(COVID19-S4):S32–S36
Lin Y, Hu Z, Alias H, Wong LP (2020) Influence of mass and social media on psychobehavioral responses among medical students during the downward trend of COVID-19 in Fujian, China: cross-sectional study. J Med Internet Res 22(7):e19982
Chandwar K, Dixit J, Kishor K, Ekbote D, Dogga P (2021) COVID-19 anniversary—the hits, the misses, and the way forward: a resident’s view. Indian J Rheumatol 16(4):481–482. https://doi.org/10.4103/injr.injr_97_21
Acknowledgements
The Submitted article was accepted to be published as an abstract: AB1501 Effect of SARS-COV-19 Pandemic on Rheumatology Training in India at EULAR 2022 with a https://doi.org/10.1136/annrheumdis-2022-eular.325.
Funding
No specific funding was received from any bodies in the public, commercial or not-for-profit sectors to carry out the work described in this article.
Author information
Authors and Affiliations
Contributions
Conceptualisation: KC. Data curation: all authors. Formal analysis: KC; funding acquisition: N/A. Investigation: KC, KK, PD, JD, DE, SM. Methodology: KC; visualisation: KC, UD. Writing—original draft: SM, KC. Writing, review and editing—all authors.
Corresponding author
Ethics declarations
Conflict of interest
All authors disclose that they do not have any direct or indirect interests (dual commitments), financial or otherwise, that might affect or be perceived to affect the conduct or reporting of the work they have submitted.
Ethical approval
The protocol was cleared by the Institutional Ethics Committee of King George’s Medical University protocol no. VI-PGTSC-IIA/P48 dated 27.10.2021.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Chandwar, K., Mukherjee, S., Ekbote, D. et al. Impact of COVID-19 pandemic on rheumatology trainees: an online survey. Rheumatol Int 43, 59–68 (2023). https://doi.org/10.1007/s00296-022-05225-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-022-05225-x