
Abstract
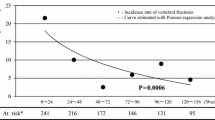
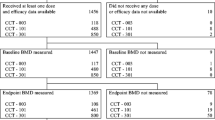
Osteoporosis is prevalent in men with an estimated one in eight men older than 50 years suffering from osteoporotic fracture, and a higher mortality rate after fracture among men compared with women. There are few approved therapies for osteoporosis in men. This observational study assesses the efficacy and safety of risedronate in the treatment of men with primary and secondary osteoporosis. A single-center, open label, randomized, prospective 1-year study was conducted in men with primary or secondary osteoporosis. Patients were randomized to risedronate (risedronate 5 mg/day plus calcium 1,000 mg/day and vitamin D 800 IU/day) or control groups (alfacalcidol 1 μg/day plus calcium 500 mg/day or vitamin D 1,000 IU/day plus calcium 800 mg/day). Bone mineral density (BMD) measurements, X-rays of the spine, a medical history and physical exam, and patient self-assessments of back pain were performed at baseline and 12 months. Blinded semi-quantitative fracture assessment was conducted by a radiologist. A total of 316 men with osteoporosis were enrolled in the trial (risedronate, n=158; control, n=158). At 1 year lumbar spine BMD increased by 4.7% in the risedronate group versus an increase of 1.0% in the control group (P<0.001). Significant increases in BMD at the total hip and femoral neck were also observed with risedronate compared with the control group. The incidence of new vertebral fracture in the risedronate group was reduced by 60% versus the control group (P=0.028). Daily treatment with risedronate for 12 months significantly increased BMD at the lumbar spine, femoral neck and total hip and significantly reduced the incidence of new vertebral fractures. This is the first prospective, randomized, controlled trial to demonstrate a significant reduction in vertebral fractures in 1 year in men with primary or secondary osteoporosis.



Similar content being viewed by others

References
Barrett-Connor E (1995) The economic and human costs of osteoporotic fracture. Am J Med 98(2A):3S–8S
Campion JM, Maricic MJ (2003) Osteoporosis in men. Am Fam Physician 67(7):1521–1526
Center JR et al (1999) Mortality after all major types of osteoporotic fracture in men and women: an observational study. Lancet 353(9156):878–882
Olszynski WP et al (2004) Osteoporosis in men: epidemiology, diagnosis, prevention, and treatment. Clin Ther 26(1):15–28
Kiebzak GM et al (2002) Undertreatment of osteoporosis in men with hip fracture. Arch Intern Med 162(19):2217–2222
Nguyen TV, Center JR, Eisman JA (2004) Osteoporosis: underrated, underdiagnosed and undertreated. Med J Aust 180(5 Suppl):S18–S22
Snyder PJ et al (2000) Effects of testosterone replacement in hypogonadal men. J Clin Endocrinol Metab 85(8):2670–2677
Orwoll E et al (2000) Alendronate for the treatment of osteoporosis in men. N Engl J Med 343(9):604–610
Ringe JD, Orwoll E, Daifotis A, Lombardi A (2002) Treatment of male osteoporosis: recent advances with alendronate. Osteoporos Int 13:195–199
Ringe JD, Dorst A, Faber H, Ibach K (2004) Alendonate treatment of established primary osteoporosis in men: 3-year results of a prospective, comparative, two-arm study. Rheumatol Int 24:110–113
Physicians’ desk reference: PDR (2003) 57th edn. Thomson PDR, Montvale, p 3550
Roux C et al (2004) Efficacy of risedronate on clinical vertebral fractures within six months. Curr Med Res Opin 20(4):433–439
Harrington T et al (2004) Risedronate rapidly reduces the risk for non-vertebral fractures in women with postmenopausal osteoporosis. Calcif Tissue Int 74:129–135
McClung MR et al (2001) Effect of risedronate on the risk of hip fracture in elderly women Hip Intervention Program Study Group. N Engl J Med 344(5):333–340
Reid DM et al (2001) Risedronate increases bone density and reduces vertebral fracture risk within one year in men on corticosteroid therapy. Calcif Tissue Int 69(4):242–247
Lindsay R et al (2001) Risk of new vertebral fracture in the year following a fracture. JAMA 285(3):320–323
Ringe JD (2000) Osteoporosis in men. In: Hosking D, Ringe J (eds) Treatment of metabolic bone disease. Management strategy and drug therapy. Martin Dunitz, London
Hasserius R et al (2003) Prevalent vertebral deformities predict increased mortality and increased fracture rate in both men and women: a 10-year population-based study of 598 individuals from the Swedish cohort in the European Vertebral Osteoporosis Study. Osteoporos Int 4(1):61–68
Ross PD et al (1991) Pre-existing fractures and bone mass predict vertebral fracture incidence in women. Ann Intern Med 114(11):919–923
Harris ST et al (1999) Effects of risedronate treatment on vertebral and nonvertebral fractures in women with postmenopausal osteoporosis: a randomized controlled trial. Vertebral Efficacy With Risedronate Therapy (VERT) Study Group. JAMA 282(14):1344–1352
Reginster J et al (2000) Randomized trial of the effects of risedronate on vertebral fractures in women with established postmenopausal osteoporosis. Vertebral Efficacy with Risedronate Therapy (VERT) Study Group. Osteoporos Int 11(1):83–91
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ringe, J., Faber, H., Farahmand, P. et al. Efficacy of risedronate in men with primary and secondary osteoporosis: results of a 1-year study. Rheumatol Int 26, 427–431 (2006). https://doi.org/10.1007/s00296-005-0004-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-005-0004-4