
Abstract
We started a single-arm, phase II, open-label, prospective clinical trial using steroids-ruxolitinib as the first-line therapy for intermediate- to high-risk aGVHD (NCT04397367). Here, we report the association of a biomarker panel (sST2, REG3α, sTNFR1, IL-6 and IL-8) with responses to GVHD therapy. The novel first-line therapy for 39 patients with newly diagnosed aGVHD consisted of 1 mg/kg methylprednisolone and 5 mg/day ruxolitinib. The serum concentrations of the biomarkers were prospectively detected at planned time points. Of the 39 patients, the complete response rate at day 28 was 82.05%. In patients who achieved CR, the concentrations of REG3α (P14 = 0.01; P28 = 0.10) and sTNFR1 (P14 = 0.42; P28 = 0.04) declined at day 14 and day 28 compared with the pre-enrolment levels. In refractory patients, the levels of REG3α at day 14 were higher than those pre-enrolment (P = 0.04). REG3α (P = 0.02) was elevated in the refractory patients compared with the patients achieving CR at day 14 after enrolment, while there was no significant difference in the levels of sST2, sTNFR1 or IL-6. Elevated REG3α levels may predict refractory aGVHD after novel first-line therapy with steroids-ruxolitinib.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Acute graft-versus-host disease (aGVHD) is a main reason for treatment failure and delayed immune reconstitution after allogeneic haematopoietic stem cell transplantation [1,2,3,4,5,6]. The response rate to first-line corticosteroid therapy for aGVHD patients is approximately 50%. The overall survival of steroid-refractory aGVHD patients is only approximately 30% [7]. A new first-line therapy to improve the efficacy of treatment for aGVHD is of great significance.
MAGIC (The Mount Sinai Acute GVHD International Consortium) biomarkers, detected at the onset of acute GVHD, are based on the levels of sST2 and REG3α and can be used to categorize patients into three risk groups, 1, 2 and 3, representing a low, intermediate and high risk of aGVHD, respectively [8]. According to the MAGIC biomarker risk, the response rate of systemic corticosteroids in patients with newly diagnosed acute GVHD is low in the intermediate- and high-risk acute GVHD groups [9,10,11]. Recently, an association between the levels of IL-6, sTNFR1 and IL-8 and the severity of GVHD or the response to corticosteroid therapy has been published [12,13,14].
Ruxolitinib, a JAK1/JAK2 inhibitor, has been shown to be a promising agent for steroids-resistant aGVHD [15,16,17,18]. Delgado MC et al. [16] showed that ruxolitinib is capable of sensitizing cells to dexamethasone-induced apoptosis in vitro, suggesting that ruxolitinib may reverse resistance to corticosteroids. Ruxolitinib is mainly metabolized by the cytochrome P450 (CYP450) enzymes CYP2C9 and CYP3A4 [19]. In our centre, azoles are used to prevent fungal infection during GVHD treatment. Azoles are potent CYP3A4 inhibitors. When strong CYP3A4 inhibitors are concomitantly used, the efficacy of halving the dose of ruxolitinib has been established [19,20,21,22,23]. The half-life of ruxolitinib was extended from 3.7 to 6 h when given in combination with ketoconazole [23].
A safety study of ruxolitinib [23] for an episode of grade 4 neutropenia established 25 mg q12h as the maximum tolerated dose, whereas for qd dosing, the highest dose (100 mg q24h) was well tolerated. In this study, steroids-ruxolitinib was used as the first-line therapy for aGVHD patients. Treatment was initiated in most of these patients within 30 days after transplantation. The patients’ haematopoietic reconstitutions were fragile at that time. In our previous dose-finding study [24], we demonstrated that the combined use of 1 mg/kg methylprednisolone and 5 mg/day ruxolitinib yielded an optimal response and tolerance as first-line therapy. For these reasons, we chose a once-daily administration of ruxolitinib for our patients in our study. Hence, we started a single-arm, phase II, open-label, prospective clinical trial using steroids-ruxolitinib as the first-line therapy for aGVHD (NCT04397367). Here, we investigate the association of biomarker panels (sST2, REG3α, sTNFR1, IL-6, and IL-8) with responses to the steroids-ruxolitinib first-line therapy, along with the clinical outcomes in this trial.
Methods
Study design
This was a single-arm, phase II, open-label, prospective clinical trial (Clinical Trials.gov Identifier: NCT04397367) approved by the Ethics Committee of the Chinese PLA General Hospital. All participating patients provided signed informed consent. The inclusion criteria were as follows: (1) systematic aGVHD with biomarker panel detection and complete information at all time points, including day 0 prior to enrolment and day 7, day 14 and day 28 after enrolment; (2) 14 to 65 years of age; (3) newly diagnosed acute GVHD with moderate to severe risk (high Minnesota acute GVHD Risk Score or MAGIC biomarker 2/3 risk); and (4) haematological malignancy. The exclusion criteria were as follows: (1) incomplete aGVHD biomarker detection information due to the COVID-19 pandemic, patients’ desires or financial issues; (2) chronic GVHD (cGVHD); (3) late acute GVHD; (4) DLI-related aGVHD; and (5) contraindications to corticosteroid therapy.
A total of 160 patients underwent allogeneic haematopoietic cell transplantation at our unit from January 2, 2019, to May 10, 2020. Thirty-nine patients newly diagnosed with moderate to severe aGVHD received steroids-ruxolitinib as the first-line therapy and were tested for aGVHD biomarkers at designed time points (Figure S1). Their basic clinical data are shown in Table 1.
Monitoring of aGVHD biomarkers
The levels of aGVHD biomarkers, including sST2, REG3α, IL-6, IL-8 and sTNFR1, in serum samples were detected by Human Magnetic Luminex Screening Assay (5PLEX). Detection was performed according to a procedure specified by the manufacturer of the R&D system customized cytokine detection kit (LXSAHM-05). Detection was performed at aGVHD onset and before steroids-ruxolitinib therapy and at day 7, day 14 and day 28 after enrolment. All samples were fresh and analysed within 24 h at the Beijing Beaufre biolaboratory.
GVHD prophylaxis
All patients received modified BU/CY + ATG myeloablative conditioning regimens as previously described [25, 26]. Cyclosporin A (CsA), mycophenolate mofetil (MMF) and short-term methotrexate (MTX) were used for GVHD prophylaxis. CsA at a dose of 2 mg/kg was given intravenously from day − 10, with a trough concentration of 200 to 250 ng/ml. Three to six months after transplantation, in patients without a relapse of the underlying disease and without cGVHD, the dose of CsA was reduced by 25% every 2 weeks until discontinuation. MMF at a dose of 500 mg was orally administered twice daily from day − 10 to day + 30. MTX at a dose of 15 mg/m2 was administered intravenously on day + 1, followed by 10 mg/m2 on day + 3, day + 6 and day + 11. Rabbit anti-thymocyte globulin (rATG, thymoglobulin, rabbit; Genzyme Pharmaceutical Company, USA) was infused from day − 5 to day − 2 at a total dose of 10 mg/kg.
Acute GVHD therapy
Patients newly diagnosed with moderate- to severe-risk aGVHD were administered ruxolitinib (5 mg/day)-methylprednisolone (1 mg/kg/day) as the first-line therapy. Detailed information on the regimen was described in our previous study [24]. Blood samples were collected before corticosteroid therapy to assess biomarker status, with expected results within 48 h after corticosteroid therapy. Ruxolitinib therapy was administered within 48 h after corticosteroid therapy based on MAGIC biomarker risk eligibility (ruxolitinib therapy was not administered until biomarker results were available). In our study, methylprednisolone was first tapered, followed by cyclosporin, and then by ruxolitinib after acute GVHD CR. The initial dose of methylprednisolone (or prednisone dose equivalent) was 1 mg/kg/day for 5 days. A suggested dose-tapering plan was conducted as follows: the dose was decreased to 0.6 mg/kg/day after 5 days, 0.4 mg/kg/day after 5 days, 0.3 mg/kg/day after 5 days, 0.25 mg/kg/day after 5 days, 0.18 mg/kg/day after 5 days, 0.1 mg/kg/day at week 4 and 0.1 mg/kg/day every other day after 5 days, and methylprednisolone was stopped at week 6. The suggested cumulative methylprednisolone dose was 15.4 mg/kg, and the suggested time of discontinuation was 39 days. In the absence of recurrent acute GVHD and after methylprednisolone discontinuation, cyclosporin was tapered and withdrawn in the following 60 days. After cyclosporin discontinuation, ruxolitinib was tapered (approximately 95 days after ruxolitinib administration) in the absence of acute GVHD. Ruxolitinib was discontinued within 90 days after tapering, and the total duration of administration was approximately 6 months. Reasons for drug withdrawal included thrombocytopenia, leukaemia relapse, aGVHD recurrence, posttransplant lymphoproliferative disease (PTLD), cytomegalovirus encephalitis and pneumonia. In addition, clinicians might decide whether to reduce the dose of or completely withdraw the drug based on a comprehensive evaluation of the disease. Patients without response to the regimen were administered an anti-interleukin-2 receptor antibody (basiliximab) at a dose of 20 mg at day 1, day 4 and day 8 and then once a week for 4–6 doses.
CMV and EBV monitoring and supportive therapy
All patients received ganciclovir (day − 10 ~ day − 2) and acyclovir (day + 1 ~ day + 180) to prevent viral infection. Quantitative real-time PCR detection was performed once every week for EBV and CMV DNA contents from day + 14 to day + 90 and then twice every month from day + 100 to day + 180. Patients with a CMV DNA copy number above 1 × 103 copies/ml twice or above 1 × 104 copies/ml once were diagnosed as having CMV reactivation, which was an indication for anti-CMV pre-emptive therapy. Ganciclovir was given for at least 2 weeks until the CMV DNA copy number decreased. An EBV DNA copy number above 1 × 104 copies/ml twice was the indication for pre-emptive rituximab treatment. Supportive therapy, including intestinal sterilization, pneumocystis carinii pneumonia (PCP) preventive therapy and herpes simplex/shingles preventive therapy, was administered as previously described [27, 28].
Definitions
The last follow-up date was December 28, 2020, with dates before transplantation recorded as day − and those after transplantation as day + .
Response types for aGVHD treatment are defined as complete remission (CR), partial remission (PR), no remission (NR) or progressive disease (PD). CR refers to the complete disappearance of aGVHD manifestations in all GVHD-affected organs. PR was reflected by the improvement (at least one grade lower but not to the extent of CR) of aGVHD in all initially affected organs without aGVHD deterioration in any other target organ. NR refers to no improvement or the deterioration of aGVHD in all organs. PD refers to the deterioration of aGVHD (at least one grade worse) in at least one target organ, with or without improvement in other organs. PD and NR indicate no response to the therapy. Refractory acute GVHD was defined as (i) the progression of GVHD at least 3 days after enrolment; (ii) a lack of improvement in GVHD (PR or better) at least 7 days after enrolment; (iii) no CR at least 14 days after enrolment; or (iv) a loss of response, defined as a worsening or recurrence of GVHD at any time after initial CR.
Acute GVHD was graded by the “1994 Consensus” [29]. Overall survival (OS) was defined as the time from enrolment to death from any cause. Disease-free survival (DFS) was defined as the time from enrolment to relapse of the underlying malignancy. Relapse of the underlying malignancy was defined as blasts detected by morphological evidence in the peripheral blood, bone marrow or extramedullary sites. Nonrelapse mortality (NRM) was defined as death from causes other than a relapse of the underlying malignancy. Failure-free survival (FFS) was defined as survival without relapse, nonrelapse mortality or the addition of systemic therapy for acute GVHD.
Statistical analysis
IBM SPSS Statistics 24.0 software was used for statistical analysis. Biomarker levels were stratified by response (CR, refractory) for each enrolment arm; those that differed by response were analysed by logistic regression to assess the association (CR versus refractory). Changes in biomarker levels over time (pre-enrolment to day 7, day 14, day 28) were assessed via geometric mean values at each visit, along with the fold change from the pre-enrolment value. The chi-squared test and Fisher’s exact test were performed to analyse qualitative data (median, range) as appropriate. The area under the curve (AUC) values for the receiver operating characteristic (ROC) curve, calculated by GraphPad Prism 8.0 software, were compared among biomarkers at all time points, including day 0 prior to enrolment and day 7, day 14 and day 28 after enrolment. Kaplan–Meier curves were generated to assess OS, DFS and FFS. The cumulative incidences of relapse and NRM were analysed by competing risks. Relapse was considered a competing event for NRM. Transplant-related death was considered a competing event for relapse. Kaplan–Meier analysis and the competing risks were conducted by R 3.6 statistical software (“survival”, “survminer” and “cmprsk”). Two-sided P < 0.05 indicated statistical significance.
Results
Patient characteristics and the efficacy of steroids-ruxolitinib therapy
aGVHD
Steroids-ruxolitinib as the first-line therapy was administered to 39 patients with moderate to severe aGVHD. Eleven patients developed grade I aGVHD (28.21%), 25 developed grade II aGVHD (64.10%) and 3 developed grade III aGVHD (7.69%). The involved organs were the gastrointestinal tract only (n = 14, 35.89%) and the skin only (n = 14, 35.89%). Eleven patients had both gastrointestinal tract and skin involvement (28.21%). The median time for the onset of aGVHD was 21 (range, 11 to 43) days after transplantation.
First-line therapy
Novel first-line therapy was administered for a median of 126 (34 to 302) days. The planned duration of ruxolitinib is usually 180 days. Fourteen patients stopped ruxolitinib as planned. Ruxolitinib was discontinued earlier in 19 patients (48.7%) due to relapse (n = 9), PTLD/CMV encephalitis (n = 2), thrombocytopenia (n = 2), therapeutic DLI (n = 4) and at the doctor’s discretion (n = 2). In 6 patients, ruxolitinib was maintained for more than 180 days due to aGVHD recurrence. The mean cumulative dose of corticosteroids used was 15.97 ± 5.30 mg/kg, and the mean duration of corticosteroids use was 40.19 ± 15.66 days.
Response
The total response rate at day 28 after enrolment was 82.05% (95% CI, 67.33–91.02%). All patients with response achieved CR. Seven (17.95%) patients experienced refractory aGVHD with the involvement of the skin (n = 6) and gastrointestinal tract (n = 1). Three (7.69%) patients had aGVHD recurrence after initial complete remission within 100 days after transplantation (at day + 35, day + 58 and day + 67). Four patients (10.25%) developed late aGVHD involving the skin (at day 108, range: day + 103 ~ day + 111) due to decreased doses of cyclosporin or ruxolitinib. Two patients developed late aGVHD involving the skin (n = 1) and gastrointestinal tract (n = 1) after therapeutic DLI. Two of the six late aGVHD patients received second-line therapy, and four responded again after the dose of steroids was elevated by one or two steps in the tapering schedule. Five patients (12.82%) required second-line therapy with basiliximab because they were refractory to the steroids-ruxolitinib regimen as first-line therapy (n = 3) and developed therapeutic DLI-related late aGVHD (n = 2). All patients survived more than 100 days after transplantation and were evaluated for cGVHD. Two patients developed mild and moderate cGVHD after multiple late aGVHD recurrences. The patient with moderate cGVHD received additional immunosuppressive therapy and achieved complete remission (Table 2).
Survival
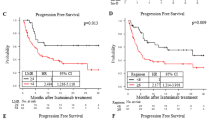
During follow-up, six patients died at a median of 223 (118 ~ 295) days from transplant-related reasons (n = 2, viral gastroenteritis and CMV encephalitis) and leukaemia relapse (n = 4). One patient developed viral enteritis with gastrointestinal haemorrhage after 76 days of ruxolitinib treatment with complete remission of aGVHD for 73 days. The patient died from viral enteritis 16 days after ruxolitinib withdrawal. The other patient developed CMV encephalitis 155 days after the withdrawal of ruxolitinib due to multiple aGVHD recurrences. He developed cGVHD with a poor response to treatment and died from CMV encephalitis (225 days after transplantation). Among the 39 aGVHD patients, a relapse of the malignant haematological disease was documented in 7 patients at a median of 126 days (range: 47–169 days) after transplantation. Four patients died of relapsed disease, and three achieved leukaemia-free survival after salvage therapy. The median survival time for relapsed patients was 221 days (range: 113–508 days) after transplantation.
The 180-day OS, DFS, cumulative relapse and FFS rates were 93.00% (95% CI 84.04–100.00%), 75.50% (95% CI 61.93–92.05%), 18.60% (95% CI 17.62–19.58%) and 57.53% (95% CI 42.03–76.89%), respectively. The 365-day OS, DFS, FFS, NRM and cumulative relapse rates were 75.82% (95% CI 60.44–95.09%), 66.94% (95% CI 51.61–86.83%), 57.53% (95% CI 43.04–76.89%), 7.17% (95% CI 6.67–7.67%), and 23.56% (95% CI 22.21–24.90%), respectively.
There were no significant differences in the day 28 CR rate, relapse rate of the underlying malignancy or NRM between the MAGIC high-risk (n = 22) and moderate-risk (n = 17) aGVHD patients (Table 3).
Side effects
During steroids-ruxolitinib therapy, 76.92% of patients had CMV viremia, which lasted 28 (3 ~ 98) days. Nine patients (30.00%) had CMV reactivation before steroids-ruxolitinib administration, and twenty-one patients (70.00%) developed CMV viremia after steroids-ruxolitinib therapy. CMV viremia was controlled with antiviral therapy without steroids-ruxolitinib therapy discontinuation. Two (5.13%) patients developed CMV encephalitis. One of them developed CMV encephalitis 5 months after the withdrawal of ruxolitinib due to aGVHD recurrence and poor control of cGVHD and died from CMV encephalitis. The other suffered from disease relapse and stopped ruxolitinib. He developed CMV encephalitis on the 57th day after ruxolitinib discontinuation.
During steroids-ruxolitinib therapy, 82.05% of patients had EBV viremia, which lasted 19 (3 ~ 66) days. Seven patients (21.87%) had EBV reactivation before steroids-ruxolitinib administration, and twenty-five patients (78.13%) developed EBV viremia after the steroids-ruxolitinib therapy. EBV reactivation was controlled with rituximab without steroids-ruxolitinib therapy discontinuation. Two patients (5.13%) developed PTLD, which was controlled well. Three patients developed thrombocytopenia during steroids-ruxolitinib administration. Ruxolitinib was discontinued in 2 patients. The patients experienced thrombocytopenia for 9 and 6 days and then recovered without ruxolitinib discontinuation.
REG3α and sTNFR1 decreased significantly in aGVHD patients achieving complete remission after steroids-ruxolitinib first-line therapy
In this study, aGVHD patients who achieved CR at day 7, day 14 and day 28 after first-line therapy with steroids-ruxolitinib were assessed for the aGVHD biomarker panel before and after enrolment.
At day 7, the levels of REG3α (P = 0.18), IL-6 (P = 0.37) and sTNFR1 (P < 0.01) decreased, among which sTNFR1 levels showed the most significant difference compared with their pre-enrolment levels. At day 14 and day 28 after enrolment, the levels of REG3α (P14 = 0.01; P28 = 0.10) and sTNFR1 (P14 = 0.42; P28 = 0.04) declined. IL-6 levels increased but not significantly (P14 = 0.82; P28 = 0.57) compared with the pre-enrolment values. The maximum change in REG3α from pre-enrolment levels was observed at day 14; the change was maintained at day 28 in CR patients (Fig. 1B–E).

aGVHD biomarker level changing trend in complete remission patients at exact time points using ruxolitinib combined with methylprednisolone. Asterisk, days from first treatment dose; sST2, soluble suppression of tumorigenicity 2; REG3α, regenerating islet-derived protein 3-alpha; IL-6, interleukin-6; IL-8, interleukin-8; sTNFR1, soluble TNF receptor 1
The levels of sST2 increased in CR patients at day 7 and day 14 compared with their pre-enrolment levels (P7 = 0.02; P14 = 0.07). When compared with the levels at day 7 after enrolment, the levels of sST2 decreased in patients achieving CR at days 14 and 28 after first-line therapy with steroids-ruxolitinib (day 14 versus day 7, P = 0.52; day 28 versus day 7, P < 0.01, Fig. 1A).
The MAGIC scores calculated based on sST2 and REG3α levels were higher at day 7 than the pre-enrolment scores (P < 0.01). The score at day 14, although lower than the score at day 7 (P < 0.05), was still higher than that before enrolment (P = 0.03). On day 28, the MAGIC scores decreased below the pre-enrolment scores (P = 0.08, Figure S2 A).
REG3α increased significantly in refractory aGVHD patients after first-line therapy with steroids-ruxolitinib
The plasma REG3α levels at day 7, day 14 and day 28 after enrolment in the refractory patients were higher than the pre-enrolment levels (P7 = 0.51, P14 = 0.04, P28 = 0.59). The levels of sTNFR1 at day 7, day 14 and day 28 after enrolment in the refractory patients were lower than those pre-enrolment, but the difference was not statistically significant (P7 = 0.39, P14 = 0.47, P28 = 0.14). The levels of sST2 and MAGIC scores in the refractory patients increased on day 7 (PsST2 = 0.07, PMAGIC = 0.47) and day 14 (PsST2 = 0.37, PMAGIC = 0.40) and decreased on day 28 (PsST2 = 0.04, PMAGIC = 0.13) compared with those pre-enrolment. On day 14, the levels of IL-6 and IL-8 were elevated when compared with those pre-enrolment, but the difference was not statistically significant (PIL-6 = 0.72, PIL-8 = 0.42) and at day 7, IL-6 and IL-8 decreased compared with those pre-enrolment(PIL-6 = 0.09, PIL-8 = 0.37, Fig. 2A).

Increased REG3α levels after steroids-ruxolitinib treatment in refractory aGVHD patients. A aGVHD biomarker changing trend in refractory patients pre-enrolment and at days 7, 14, and 28 after enrolment (independent-sample T test); B aGVHD biomarker changing trend in complete remission patients and the refractory patients at day 14 after enrolment (independent-sample T test); Asterisk, days from first treatment dose; aGVHD, acute graft-versus-host disease; sST2, soluble suppression of tumorigenicity 2; REG3α, regenerating islet-derived protein 3-alpha; IL-6, interleukin-6; IL-8, interleukin-8; sTNFR1, soluble TNF receptor 1
Elevated REG3α was associated with refractory aGVHD at day 14 after first-line therapy with steroids-ruxolitinib
There were no differences in the pre-enrolment levels of the five biomarkers and MAGIC scores between CR and refractory patients.
There were no significant differences in the levels of sST2, sTNFR1, IL-6 or IL-8 or MAGIC scores between CR and refractory aGVHD at day 7, day 14 and day 28. REG3α was increased in refractory patients compared with CR patients, with a statistically significant difference only at 14 days after enrolment (P = 0.02). No statistically significant difference in REG3α was found at other time points (Fig. 2B, Figure S2 B-D).
The area under the ROC curve (AUC) of REG3α at day 0, day 7, day 14 and day 28 after enrolment was 0.535 (95% CI: 0.336–0.733), 0.593 (95% CI: 0.132–1.000), 1.000 (95% CI: 1.000–1.000) and 0.583 (95% CI: 0.138–1.000), respectively. The AUC for REG3α at day 14 after enrolment was the largest, at 1.000, among the AUCs of other biomarkers at day 0, day 7, day 14 and day 28 after enrolment (0.500 to 0.792).
Discussion
This was the first prospective study assessing the kinetics of aGVHD biomarkers in response to novel first-line therapy with ruxolitinib (5 mg/day)-methylcorticosteroids (1 mg/kg/day). The patients were newly diagnosed with moderate- to severe-risk aGVHD. In all aGVHD patients treated with steroids-ruxolitinib therapy, the day 28 CR rate was 82.05%. In patients who achieved CR after therapy, the levels of REG3α and sTNFR1 declined at day 14 and day 28 compared with the pre-enrolment values. In patients who were refractory to therapy, the levels of REG3α at day 7, day 14 and day 28 after enrolment were higher than the pre-enrolment levels. There were no significant differences in the concentrations of sST2, sTNFR1 or IL-6 between CR and refractory patients at day 7, day 14 and day 28 after enrolment. No difference in MAGIC scores was noted in CR and refractory patients. REG3α was elevated in the refractory patients compared with the patients achieving CR at day 14 after enrolment. Increased REG3α levels may predict refractory aGVHD in patients administered steroids-ruxolitinib as first-line therapy.
The response rate of the novel first-line therapy, steroids-ruxolitinib, for aGVHD was promising in patients with moderate and high “Minnesota and MAGIC” risk. Grading based on the Minnesota and Glucksberg criteria was primarily developed as an important tool to determine the appropriate management of aGVHD and to assess the response to steroid therapy. The onset grade of 11 patients in this study was grade I, but the MAGIC biomarker risk status for those patients was high risk, which is predictive of a poor response to steroids. Based on these aspects, 11 patients were treated with novel first-line therapy with ruxolitinib to reverse potential steroid resistance.
In all aGVHD patients treated with steroids-ruxolitinib therapy, the day 28 CR rate was 82.05%. The day 28 CR rate of aGVHD patients with an affected gastrointestinal tract was 84.00% (21/25). There were no significant differences in day 28 CR rate or NRM between the MAGIC high-risk (n = 22) and moderate-risk (n = 17) aGVHD patients. There were no differences in the five biomarkers or MAGIC scores before treatment in CR and refractory patients. This suggested that first-line therapy with steroids-ruxolitinib results in a high response rate in patients newly diagnosed with moderate to severe aGVHD across different aGVHD grades, biomarker risks and involved organs.
Soluble suppression of tumorigenicity 2 (sST2), a member of the IL-1 receptor family, is highly secreted by endothelial cells and epithelial cells and stimulated by inflammation [30, 31]. The Vander Lugt research team pointed out that a high sST2 concentration could serve as an independent biomarker of drug resistance and mortality in aGVHD therapies [31]. Large amounts of regenerating islet-derived protein 3-alpha (REG3α) enter the systemic circulation when aGVHD develops in the gastrointestinal tract with mucosal epithelial barrier damage [32, 33]. REG3α was the best diagnostic biomarker for gastrointestinal GVHD. The concentration of REG3α decreased in the posttherapy peripheral blood of complete remission patients but increased in refractory patients at day 7, day 14 and day 28, suggesting that REG3α responds to ruxolitinib earlier than sST2 and may be associated with the treatment response, which still needs confirmation. The MAGIC scores at acute GVHD onset are based on two biomarkers (ST2 and REG3α), with higher scores reflecting elevated steroid resistance risk [8, 34]. In this study, we found that the trend of MAGIC scores after the treatment was similar to that of sST2 in the peripheral blood of patients, and there was no difference between the CR patients and the refractory patients. The profile of the REG3α level, but not the sST2 level, and the MAGIC score after first-line therapy with steroids-ruxolitinib, was of certain significance in evaluating treatment efficacy in these patients and needs to be further studied.
In conclusion, this study suggested that steroids-ruxolitinib first-line therapy could result in a high response rate in patients newly diagnosed with moderate- to severe-risk aGVHD. The kinetics of the aGVHD biomarkers were different after steroids-ruxolitinib therapy, which provides a basis for selecting the next treatment option. The profile of REG3α after first-line therapy with steroids-ruxolitinib is of certain significance in evaluating the treatment efficacy of the steroids-ruxolitinib regimen. However, the sample size in this study was small, and the above conclusions need to be confirmed in studies with larger sample sizes. In addition, it is essential to further explore the mechanism underlying the changes in aGVHD biomarkers after steroids-ruxolitinib treatment.
Data availability
The datasets generated and analysed in the present study are available from the corresponding author upon reasonable request.
References
Wang H, Liu YC, Zhu CY, Yan F, Wang MZ, Chen XS, Wang XK, Pang BX, Li YH, Liu DH, Gao CJ, Liu SJ, Dou LP (2020) Chidamide increases the sensitivity of refractory or relapsed acute myeloid leukemia cells to anthracyclines via regulation of the HDAC3 -AKT-P21-CDK2 signaling pathway. Journal of experimental & clinical cancer research: CR 39(1):278
Dou L, Xu Q, Wang M, Xiao Y, Cheng L, Li H, Huang W, Mei J, Jing Y, Bo J, Liu D, Yu L (2019) Clinical efficacy of decitabine in combination with standard-dose cytarabine, aclarubicin hydrochloride, and granulocyte colony-stimulating factor in the treatment of young patients with newly diagnosed acute myeloid leukemia. Onco Targets Ther 12:5013–5023
Zhou L, Wang Q, Chen X, Fu L, Zhang X, Wang L, Deng A, Li D, Liu J, Lv N, Wang L, Li Y, Liu D, Yu L, Dou L (2017) AML1-ETO promotes SIRT1 expression to enhance leukemogenesis of t(8;21) acute myeloid leukemia. Exp Hematol 46:62–69
Flowers ME, Inamoto Y, Carpenter PA, Lee SJ, Kiem HP, Petersdorf EW, Pereira SE, Nash RA, Mielcarek M, Fero ML, Warren EH, Sanders JE, Storb RF, Appelbaum FR, Storer BE, Martin PJ (2011) Comparative analysis of risk factors for acute graft-versus-host disease and for chronic graft-versus-host disease according to National Institutes of Health consensus criteria. Blood 117(11):3214–3219
Zeiser R, Blazar BR (2017) Acute graft-versus-host disease - biologic process, prevention, and therapy. N Engl J Med 377(22):2167–2179
Rezvani AR, Storb RF (2012) Prevention of graft-vs-host disease. Expert opinion on pharmacotherapy 13(12):1737–1750
Levine JE, Paczesny S, Mineishi S, Braun T, Choi SW, Hutchinson RJ, Jones D, Khaled Y, Kitko CL, Bickley D, Krijanovski O, Reddy P, Yanik G, Ferrara JL (2008) Etanercept plus methylprednisolone as initial therapy for acute graft-versus-host disease. Blood 111(4):2470–2475
Srinagesh HK, Özbek U, Kapoor U, Ayuk F, Aziz M, Ben-David K, Choe HK, DeFilipp Z, Etra A, Grupp SA, Hartwell MJ, Hexner EO, Hogan WJ, Karol AB, Kasikis S, Kitko CL, Kowalyk S, Lin JY, Major-Monfried H, Mielke S, Merli P, Morales G, Ordemann R, Pulsipher MA, Qayed M, Reddy P, Reshef R, Rösler W, Sandhu KS, Schechter T, Shah J, Sigel K, Weber D, Wölfl M, Wudhikarn K, Young R, Levine JE, Ferrara JLM (2019) The MAGIC algorithm probability is a validated response biomarker of treatment of acute graft-versus-host disease. Blood Adv 3(23):4034–4042
MacMillan ML, DeFor TE, Holtan SG, Rashidi A, Blazar BR, Weisdorf DJ (2020) Validation of Minnesota acute graft-versus-host disease Risk Score. Haematologica 105(2):519–524
Hartwell MJ, Özbek U, Holler E, Renteria AS, Major-Monfried H, Reddy P, Aziz M, Hogan WJ, Ayuk F, Efebera YA, Hexner EO, Bunworasate U, Qayed M, Ordemann R, Wölfl M, Mielke S, Pawarode A, Chen YB, Devine S, Harris AC, Jagasia M, Kitko CL, Litzow MR, Kröger N, Locatelli F, Morales G, Nakamura R, Reshef R, Rösler W, Weber D, Wudhikarn K, Yanik GA, Levine JE, Ferrara JL (2017) An early-biomarker algorithm predicts lethal graft-versus-host disease and survival. JCI insight 2(3):e89798
Ferrara JLM, Chaudhry MS (2018) GVHD: biology matters. Blood Adv 2(22):3411–3417
Chen X, Das R, Komorowski R, Beres A, Hessner MJ, Mihara M, Drobyski WR (2009) Blockade of interleukin-6 signaling augments regulatory T-cell reconstitution and attenuates the severity of graft-versus-host disease. Blood 114(4):891–900
Tawara I, Koyama M, Liu C, Toubai T, Thomas D, Evers R, Chockley P, Nieves E, Sun Y, Lowler KP, Malter C, Nishimoto N, Hill GR, Reddy P (2011) Interleukin-6 modulates graft-versus-host responses after experimental allogeneic bone marrow transplantation. Clinical cancer research : an official journal of the American Association for Cancer Research 17(1):77–88
Toubai T, Tanaka J, Paczesny S, Shono Y, Reddy P, Imamura M (2012) Role of cytokines in the pathophysiology of acute graft-versus-host disease (GVHD): are serum/plasma cytokines potential biomarkers for diagnosis of acute GVHD following allogeneic hematopoietic cell transplantation (Allo-HCT)? Curr Stem Cell Res Ther 7(3):229–239
Jagasia M, Perales MA, Schroeder MA, Ali H, Shah NN, Chen YB, Fazal S, Dawkins FW, Arbushites MC, Tian C, Connelly-Smith L, Howell MD, Khoury HJ (2020) Ruxolitinib for the treatment of steroid-refractory acute GVHD (REACH1): a multicenter, open-label phase 2 trial. Blood 135(20):1739–1749
Delgado-Martin C, Meyer LK, Huang BJ, Shimano KA, Zinter MS, Nguyen JV, Smith GA, Taunton J, Winter SS, Roderick JR, Kelliher MA, Horton TM, Wood BL, Teachey DT, Hermiston ML (2017) JAK/STAT pathway inhibition overcomes IL7-induced glucocorticoid resistance in a subset of human T-cell acute lymphoblastic leukemias. Leukemia 31(12):2568–2576
Przepiorka D, Luo L, Subramaniam S, Qiu J, Gudi R, Cunningham LC, Nie L, Leong R, Ma L, Sheth C, Deisseroth A, Goldberg KB, Blumenthal GM, Pazdur R (2020) FDA Approval summary: ruxolitinib for treatment of steroid-refractory acute graft-versus-host disease. Oncologist 25(2):e328–e334
Zeiser R, von Bubnoff N, Butler J, Mohty M, Niederwieser D, Or R, Szer J, Wagner EM, Zuckerman T, Mahuzier B, Xu J, Wilke C, Gandhi KK, Socié G (2020) Ruxolitinib for glucocorticoid-refractory acute graft-versus-host disease. N Engl J Med 382(19):1800–1810
Umehara K, Huth F, Jin Y, Schiller H, Aslanis V, Heimbach T, He H (2019) Drug-drug interaction (DDI) assessments of ruxolitinib, a dual substrate of CYP3A4 and CYP2C9, using a verified physiologically based pharmacokinetic (PBPK) model to support regulatory submissions. Drug metabolism and personalized therapy 34 (2).
Shi JG, Chen X, Emm T, Scherle PA, McGee RF, Lo Y, Landman RR, McKeever EG Jr, Punwani NG, Williams WV, Yeleswaram S (2012) The effect of CYP3A4 inhibition or induction on the pharmacokinetics and pharmacodynamics of orally administered ruxolitinib (INCB018424 phosphate) in healthy volunteers. J Clin Pharmacol 52(6):809–818
Aslanis V, Umehara K, Huth F, Ouatas T, Bharathy S, Butler AA, Zhou W, Gadbaw B (2019) Multiple administrations of fluconazole increase plasma exposure to ruxolitinib in healthy adult subjects. Cancer Chemother Pharmacol 84(4):749–757
Ogama Y, Mineyama T, Yamamoto A, Woo M, Shimada N, Amagasaki T, Natsume K (2013) A randomized dose-escalation study to assess the safety, tolerability, and pharmacokinetics of ruxolitinib (INC424) in healthy Japanese volunteers. Int J Hematol 97(3):351–359
Shi JG, Chen X, McGee RF, Landman RR, Emm T, Lo Y, Scherle PA, Punwani NG, Williams WV, Yeleswaram S (2011) The pharmacokinetics, pharmacodynamics, and safety of orally dosed INCB018424 phosphate in healthy volunteers. J Clin Pharmacol 51(12):1644–1654
Hou C, Dou L, Jia M, Li F, Wang S, Gao X, Wang L, Jin X, Wang L, Gao C, Liu D (2021) Ruxolitinib combined with corticosteroids as first-line therapy for acute graft-versus-host disease in haploidentical peripheral blood stem cell transplantation recipients. Transplantation and cellular therapy 27(1):75.e71-75.e10
Dou L, Hou C, Ma C, Li F, Gao X, Huang W, Wang S, Gao C, Yu L, Liu D (2020) Reduced risk of chronic GVHD by low-dose rATG in adult matched sibling donor peripheral blood stem cell transplantation for hematologic malignancies. Ann Hematol 99(1):167–179
Dou LP, Li HH, Wang L, Li F, Huang WR, Yu L, Liu DH (2018) Efficacy and safety of unmanipulated haploidentical related donor allogeneic peripheral blood stem cell transplantation in patients with relapsed/refractory acute Myeloid Leukemia. Chin Med J 131(7):790–798
Li HH, Li F, Gao CJ, Huang WR, Bo J, Dou LP, Wang LL, Jing Y, Wang L, Li WJ, Yu L, Liu DH (2017) Similar incidence of severe acute GVHD and less severe chronic GVHD in PBSCT from unmanipulated, haploidentical donors compared with that from matched sibling donors for patients with haematological malignancies. Br J Haematol 176(1):92–100
Dou LP, Hou C, Yang T, Cheng LC, Bo J (2020) Characteristics of pathogens detected in adults with hematological malignancies and nosocomial infections in the tropics. Chin Med J 133(14):1735–1737
Przepiorka D, Weisdorf D, Martin P, Klingemann HG, Beatty P, Hows J, Thomas ED (1995) 1994 Consensus conference on acute GVHD grading. Bone Marrow Transplant 15(6):825–828
Kumar S, Tzimas MN, Griswold DE, Young PR (1997) Expression of ST2, an interleukin-1 receptor homologue, is induced by proinflammatory stimuli. Biochem Biophys Res Commun 235:474–478
Vander Lugt MT, Braun TM, Hanash S et al (2013) ST2 as a marker for risk of therapy-resistant graft-versus-host disease and death. N Engl J Med 369:529–539
Presland RB (2017) Application of proteomics to graft-versus-host disease: from biomarker discovery to potential clinical applications. Expert Rev Proteomics 14:997–1006
Ferrara JL, Harris AC, Greenson JK et al (2011) Regenerating islet-derived 3-alpha is a biomarker of gastrointestinal graft-versus-host disease. Blood 118:6702–6708
Major-Monfried H, Renteria AS, Pawarode A, Reddy P, Ayuk F, Holler E, Efebera YA, Hogan WJ, Wölfl M, Qayed M, Hexner EO, Wudhikarn K, Ordemann R, Young R, Shah J, Hartwell MJ, Chaudhry MS, Aziz M, Etra A, Yanik GA, Kröger N, Weber D, Chen YB, Nakamura R, Rösler W, Kitko CL, Harris AC, Pulsipher M, Reshef R, Kowalyk S, Morales G, Torres I, Özbek U, Ferrara JLM, Levine JE (2018) MAGIC biomarkers predict long-term outcomes for steroid-resistant acute GVHD. Blood 131(25):2846–2855
Funding
This work was partially supported by grants from the Beijing Nova Program (2011114), the National Natural Science Foundation of China (Nos. 82070178, 81770203,81700122, 81270610, 30800482), the Beijing Natural Science Foundation of China (No. 7172200 and 7132217), the Capital’s Funds for Health Improvement and Research (No. 2016–1-4082), the Fund Sponsorship of the Capital Public Health Project for DH Liu and the Hainan Provincial Natural Science Foundation of China (818MS157), the Military Translational Medicine Fund of the Chinese PLA General Hospital (ZH19003) and the Medical Big Data and Artificial Intelligence Development Fund of the Chinese PLA General Hospital (2019MBD-016, 2019MBD-008).
Author information
Authors and Affiliations
Contributions
DL and LD, conceptualization, methodology, and writing—review and editing; JY, data curation and writing—original draft; BP and LW, data curation and visualization; FL and XL, validation; XJ, MJ, and LX, investigation and resources.
Corresponding authors
Ethics declarations
Ethics approval
This was a single-arm, phase II, open-label, prospective clinical trial (Clinical Trials.gov Identifier: NCT04397367) approved by the Ethics Committee of the Chinese PLA General Hospital. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the guidelines of the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Consent to participate
Written informed consent was obtained from all individual participants included in the study.
Consent for publication
Not applicable.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Jingjing Yang, Bo Peng and Lu Wang contributed equally to this study
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Yang, J., Peng, B., Wang, L. et al. Elevated REG3α predicts refractory aGVHD in patients who received steroids-ruxolitinib as first-line therapy. Ann Hematol 101, 621–630 (2022). https://doi.org/10.1007/s00277-021-04727-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00277-021-04727-1