
Abstract
Objective
To compare the safety and effectiveness between bronchial artery embolisation (BAE) and conservative treatment for bronchiectasis-related nonmassive haemoptysis patients.
Materials and Methods
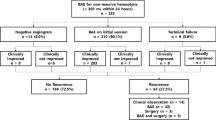
From January 2015 to December 2020, consecutive bronchiectasis-related nonmassive haemoptysis patients who underwent either BAE (n = 98) or conservative treatment (n = 118) were included. Treatment-related complications, length of hospital stays, clinical success rate, patient satisfaction, and recurrence-free survival rates were compared between groups. Prognostic factors related to recurrence were also analysed.
Results
During a median follow-up time of 44.8 months (range, 2.4–83.6 months), 34 and 66 patients in the BAE and conservative treatment groups suffered relapse. The 1-year, 2-year, 3-year and 5-year haemoptysis-free survival rates in the BAE and conservative treatment groups were 79.2%, 68.1%, 62.8%, and 57.6% and 64.0%, 52.8%, 44.1%, and 37.0%, respectively (P = 0.007). The minor complication rate after BAE was higher than that after conservative treatment (23/98 vs. 12/118, P = 0.008). BAE was associated with shorter hospital stays (5.0 vs. 7.0 days, P = 0.042) and higher patient satisfaction (88.8% vs. 74.6%, P = 0.008) than those for conservative treatment and with comparable clinical success rates (95.9% vs. 91.5%, P = 0.192). Treatment type, haemoptysis duration, and bronchiectasis severity were independently significant predictors of recurrence for these patients.
Conclusions
BAE could be another option for bronchiectasis-related nonmassive haemoptysis patients. In the patients with longer duration and more severe bronchiectasis, BAE still appeared to have better long-term haemoptysis control than conservative therapy.


Similar content being viewed by others

References
Chalmers JD, Chang AB, Chotirmall SH, et al. Bronchiectasis. Nat Rev Dis Primers. 2018;4:45. https://doi.org/10.1038/s41572-018-0042-3.
Guan WJ, Gao YH, Xu G, et al. Aetiology of bronchiectasis in Guangzhou. South China Respirol. 2015;20:739–48. https://doi.org/10.1111/resp.12528.
Pasteur MC, Bilton D, Hill AT, et al. British thoracic society guideline for non-CF bronchiectasis. Thorax. 2010;65:i1–58. https://doi.org/10.1136/thx.2010.136119.
Quint JK, Smith MP. Paediatric and adult bronchiectasis: diagnosis disease burden and prognosis. Respirology. 2019;24:413–22. https://doi.org/10.1111/resp.13495.
King PT, Holdsworth SR, Freezer NJ, et al. Characterisation of the onset and presenting clinical features of adult bronchiectasis. Respir Med. 2006;100:2183–9. https://doi.org/10.1016/j.rmed.2006.03.012.
Nicotra MB, Rivera M, Dale AM, et al. Clinical, pathophysiologic, and microbiologic characterization of bronchiectasis in an aging cohort. Chest. 1995;108:955–61. https://doi.org/10.1378/chest.108.4.955.
Panda A, Bhalla AS, Goyal A. Bronchial artery embolization in hemoptysis: a systematic review. Diagn Interv Radiol. 2017;23:307–17. https://doi.org/10.5152/dir.2017.16454.
Chun JY, Morgan R, Belli AM. Radiological management of hemoptysis: a comprehensive review of diagnostic imaging and bronchial arterial embolization. Cardiovasc Intervent Radiol. 2010;33:240–50. https://doi.org/10.1007/s00270-009-9788-z.
Davidson K, Shojaee S. Managing massive hemoptysis. Chest. 2020;157:77–88. https://doi.org/10.1016/j.chest.2019.07.012.
Kathuria H, Hollingsworth HM, Vilvendhan R, et al. Management of life-threatening hemoptysis. J Intensive Care. 2020;8:23. https://doi.org/10.1186/s40560-020-00441-8.
van den Heuvel MM, Els Z, Koegelenberg CF, et al. Risk factors for recurrence of haemoptysis following bronchial artery embolisation for life-threatening haemoptysis. Int J Tuberc Lung Dis. 2007;11:909–14 (PMID: 17705959).
Anuradha C, Shyamkumar NK, Vinu M, et al. outcomes of bronchial artery embolization for life-threatening hemoptysis due to tuberculosis and post-tuberculosis sequelae. Diagn Interv Radiol. 2012;18:96–101. https://doi.org/10.4261/1305-3825.DIR.3876-11.2.
Pei R, Zhou Y, Wang G, et al. Outcomes of bronchial artery embolization for life-threatening hemoptysis secondary to tuberculosis. Plos One. 2014;9:e115956. https://doi.org/10.1371/journal.pone.0115956.
Baltacioğlu F, Cimşit NC, Bostanci K, et al. Transarterial microcatheter glue embolization of the bronchial artery for life-threatening hemoptysis: technical and clinical results. Eur J Radiol. 2010;73:380–4. https://doi.org/10.1016/j.ejrad.2008.10.017.
Antonelli M, Midulla F, Tancredi G, et al. Bronchial artery embolization for the management of nonmassive hemoptysis in cystic fibrosis. Chest. 2002;121:796–801. https://doi.org/10.1378/chest.121.3.796.
Choi J, Baik JH, Kim CH, et al. Long-term outcomes and prognostic factors in patients with mild hemoptysis. Am J Emerg Med. 2018;36:1160–5. https://doi.org/10.1016/j.ajem.2017.11.053.
Hwang JH, Kim JH, Park S, et al. Feasibility and outcomes of bronchial artery embolization in patients with non-massive hemoptysis. Respir Res. 2021;22:221. https://doi.org/10.1186/s12931-021-01820-x.
Yan HT, Lu GD, Huang XZ, et al. A nomogram to predict recurrence after bronchial artery embolization for hemoptysis due to bronchiectasis. Cardiovasc Intervent Radiol. 2021;44:1609–17. https://doi.org/10.1007/s00270-021-02923-0.
Lu GD, Yan HT, Zhang JX, et al. Bronchial artery embolization for the management of frequent hemoptysis caused by bronchiectasis. BMC Pulm Med. 2022;22:394. https://doi.org/10.1186/s12890-022-02198-2.
Tiddens HAWM, Meerburg JJ, van der Eerden MM, et al. The radiological diagnosis of bronchiectasis: what’s in a name? Eur Respir Rev. 2020;29:190120. https://doi.org/10.1183/16000617.0120-2019.
Bedi P, Chalmers JD, Goeminne PC, et al. The BRICS (bronchiectasis radiologically indexed CT score): a multicenter study score for use in idiopathic and postinfective bronchiectasis. Chest. 2018;153:1177–86. https://doi.org/10.1016/j.chest.2017.11.033.
Yoon W, Kim YH, Kim JK, et al. Massive hemoptysis: prediction of nonbronchial systemic arterial supply with chest CT. Radiology. 2003;227:232–8. https://doi.org/10.1148/radiol.2271020324.
Sayir F, Ocakcioglu I, Şehitoğulları A, et al. Clinical analysis of pneumonectomy for destroyed lung: a retrospective study of 32 patients. Gen Thorac Cardiovasc Surg. 2019;67:530–6. https://doi.org/10.1007/s11748-018-01055-6.
Kettenbach J, Ittrich H, Gaubert JY, et al. CIRSE standards of practice on bronchial artery embolisation. Cardiovasc Intervent Radiol. 2022;45:721–32. https://doi.org/10.1007/s00270-022-03127-w.
Jones PW, Quirk FH, Baveystock CM, et al. A self-complete measure of health status for chronic airflow limitation. The St. George’s respiratory questionnaire. Am Rev Respir Dis. 1992;145:1321–7. https://doi.org/10.1164/ajrccm/145.6.1321.
Dariushnia SR, Redstone EA, Heran MKS, et al. Society of interventional radiology quality improvement standards for percutaneous transcatheter embolization. J Vasc Interv Radiol. 2021;32:476.e1-476.e33. https://doi.org/10.1016/j.jvir.2020.10.022.
Kato A, Kudo S, Matsumoto K, et al. Bronchial artery embolization for hemoptysis due to benign diseases: immediate and long-term results. Cardiovasc Intervent Radiol. 2000;23:351–7. https://doi.org/10.1007/s002700010062.
Lee JH, Kwon SY, Yoon HI, et al. Haemoptysis due to chronic tuberculosis Vs. bronchiectasis: comparison of long-term outcome of arterial embolisation. Int J Tuberc Lung Dis. 2007;11:781–7.
Lu GD, Zhang JX, Zhou CG, et al. Arterial embolization for hemoptysis in patients with chronic pulmonary tuberculosis and in patients with bronchiectasis. Acta Radiol. 2019;60:866–72. https://doi.org/10.1177/0284185118805258.
McDonald DM. Angiogenesis and remodeling of airway vasculature in chronic inflammation. Am J Respir Crit Care Med. 2001;164:S39–45. https://doi.org/10.1164/ajrccm.164.supplement_2.2106065.
McCullagh A, Rosenthal M, Wanner A, et al. The bronchial circulation-worth a closer look: a review of the relationship between the bronchial vasculature and airway inflammation. Pediatr Pulmonol. 2010;45:1–13. https://doi.org/10.1002/ppul.21135. (PMID: 20025051).
Polverino E, Goeminne PC, McDonnell MJ, et al. European respiratory society guidelines for the management of adult bronchiectasis. Eur Respir J. 2017;50:1700629. https://doi.org/10.1183/13993003.00629-2017.
Funding
This study was funded by Jiangsu Province’s Key Talents Program (QNRC2016559 to Qing-Quan Zu) and Construction Program of Jiangsu Province Clinical Research Center Support System (BL2014084 to Qing-Quan Zu).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional (Ethical review no. 2018-SR-097) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this retrospective study, formal consent was not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Yan, HT., Lu, GD., Zhang, JX. et al. Comparison of Bronchial Artery Embolisation Versus Conservative Treatment for Bronchiectasis-Related Nonmassive Haemoptysis: A Single-Centre Retrospective Study. Cardiovasc Intervent Radiol 46, 369–376 (2023). https://doi.org/10.1007/s00270-023-03361-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-023-03361-w