
Abstract
Objective
To present magnetic resonance imaging (MRI) evidence of the regression or progression of chondroid tumors and to investigate whether MRI can be used to predict the evolution of chondroid tumors.
Materials and methods
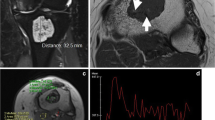
Twenty-one patients with enchondromas or atypical cartilaginous tumors who had undergone extremity MRI at least twice with a minimum 12-month interval between the MRIs were enrolled in this study. The diagnosis was based on the radiography and MRI findings. We classified the tumors into the following three groups according to changes between the MRIs: no change (NC), progression (P), and regression (R). We assessed the initial MRI features, including anatomical location, size, endosteal scalloping, peritumoral edema, fat entrapment, and direction of progression or regression. Nineteen of the 21 patients had contrast-enhanced images, and we analyzed the presence of atypical lobular enhancement against typical peripheral or septal enhancement.
Results
The R group comprised 11 cases (52%), the P group comprised five cases (24%), and the NC group comprised five cases (24%). None of the MRI features showed statistically significant differences among the groups. Atypical lobular enhancement was observed in the R (6 of 10, 60%) and NC (2 of 5, 40%) groups but not in the P group (0 of 4, 0%), although these differences were not statistically significant.
Conclusions
Chondroid tumors can either regress or progress in the MRI follow-up. Atypical lobular enhancement was seen only in stable or regressing tumors.



Similar content being viewed by others

References
Stomp W, Reijnierse M, Kloppenburg M, de Mutsert R, Bovee JV, den Heijer M, et al. Prevalence of cartilaginous tumours as an incidental finding on MRI of the knee. Eur Radiol. 2015;25(12):3480–7.
Parlier-Cuau C, Bousson V, Ogilvie CM, Lackman RD, Laredo JD. When should we biopsy a solitary central cartilaginous tumor of long bones? Literature review and management proposal. Eur J Radiol. 2011;77(1):6–12.
Deckers C, Schreuder BH, Hannink G, de Rooy JW, van der Geest IC. Radiologic follow-up of untreated enchondroma and atypical cartilaginous tumors in the long bones. J Surg Oncol. 2016;114(8):987–91.
Jo VY, Doyle LA. Refinements in sarcoma classification in the current 2013 World Health Organization classification of tumours of soft tissue and bone. Surg Oncol Clin N Am. 2016;25(4):621–43.
Crim J, Schmidt R, Layfield L, Hanrahan C, Manaster BJ. Can imaging criteria distinguish enchondroma from grade 1 chondrosarcoma? Eur J Radiol. 2015;84(11):2222–30.
Douis H, Saifuddin A. The imaging of cartilaginous bone tumours. I Benign lesions. Skelet Radiol. 2012;41(10):1195–212.
Douis H, Saifuddin A. The imaging of cartilaginous bone tumours. II Chondrosarcoma. Skelet Radiol. 2013;42(5):611–26.
Schwab JH, Wenger D, Unni K, Sim FH. Does local recurrence impact survival in low-grade chondrosarcoma of the long bones? Clin Orthop Relat Res. 2007;462:175–80.
Altay M, Bayrakci K, Yildiz Y, Erekul S, Saglik Y. Secondary chondrosarcoma in cartilage bone tumors: report of 32 patients. J Orthop Sci. 2007;12(5):415–23.
Sampath Kumar V, Tyrrell PN, Singh J, Gregory J, Cribb GL, Cool P. Surveillance of intramedullary cartilage tumours in long bones. Bone Joint J. 2016;98-B(11):1542–7.
Sensarma A, Madewell JE, Meis JM, Kumar R, Lin PP, Amini B. Regression of an enchondroma: a case report and proposed etiology. Skelet Radiol. 2015;44(5):739–42.
Yoo HJ, Hong SH, Choi JY, Moon KC, Kim HS, Choi JA, et al. Differentiating high-grade from low-grade chondrosarcoma with MR imaging. Eur Radiol. 2009;19(12):3008–14.
Murphey MD, Flemming DJ, Boyea SR, Bojescul JA, Sweet DE, Temple HT. Enchondroma versus chondrosarcoma in the appendicular skeleton: differentiating features. Radiographics. 1998;18(5):1213–37. quiz 1244-1215
Herget GW, Strohm P, Rottenburger C, Kontny U, Krauss T, Bohm J, et al. Insights into enchondroma, enchondromatosis and the risk of secondary chondrosarcoma. Review of the literature with an emphasis on the clinical behaviour, radiology, malignant transformation and the follow up. Neoplasma. 2014;61(4):365–78.
Baruchin A, Rosenberg L, Itzchaki M. Spontaneous restitution ad integrum of a fractured enchondroma in a finger. Int J Tissue React. 1981;3(1):17–20.
Passanise AM, Mehlman CT, Wall EJ, Dieterle JP. Radiographic evidence of regression of a solitary osteochondroma: a report of 4 cases and a literature review. J Pediatr Orthop. 2011;31(3):312–6.
Hill CE, Boyce L, van der Ploeg ID. Spontaneous resolution of a solitary osteochondroma of the distal femur: a case report and review of the literature. J Pediatr Orthop B. 2014;23(1):73–5.
Hansford BG, Stacy GS. From tumor to trauma: etiologically deconstructing a unique differential diagnosis of musculoskeletal entities with high signal intensity on T1-weighted MRI. AJR Am J Roentgenol. 2015;204(4):817–26.
Vanel D, Kreshak J, Larousserie F, Alberghini M, Mirra J, De Paolis M, et al. Enchondroma vs. chondrosarcoma: a simple, easy-to-use, new magnetic resonance sign. Eur J Radiol. 2013;82(12):2154–60.
Dirckx N, Van Hul M, Maes C. Osteoblast recruitment to sites of bone formation in skeletal development, homeostasis, and regeneration. Birth Defects Res C Embryo Today. 2013;99(3):170–91.
Ortega N, Behonick DJ, Werb Z. Matrix remodeling during endochondral ossification. Trends Cell Biol. 2004;14(2):86–93.
Brien EW, Mirra JM, Kerr R. Benign and malignant cartilage tumors of bone and joint: their anatomic and theoretical basis with an emphasis on radiology, pathology and clinical biology. I. The intramedullary cartilage tumors. Skelet Radiol. 1997;26(6):325–53.
Douis H, Davies AM, James SL, Kindblom LG, Grimer RJ, Johnson KJ. Can MR imaging challenge the commonly accepted theory of the pathogenesis of solitary enchondroma of long bone? Skelet Radiol. 2012;41(12):1537–42.
Amary MF, Bacsi K, Maggiani F, Damato S, Halai D, Berisha F, et al. IDH1 and IDH2 mutations are frequent events in central chondrosarcoma and central and periosteal chondromas but not in other mesenchymal tumours. J Pathol. 2011;224(3):334–43.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Rights and permissions
About this article

Cite this article
Chung, B.M., Hong, S.H., Yoo, H.J. et al. Magnetic resonance imaging follow-up of chondroid tumors: regression vs. progression. Skeletal Radiol 47, 755–761 (2018). https://doi.org/10.1007/s00256-017-2834-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-017-2834-z