
Abstract
Objective
No studies have reported the use of ultrasound for the evaluation of trigger finger after steroid injection. We evaluated the clinical features and ultrasound appearance of trigger finger before and after steroid injection under ultrasound guidance.
Materials and methods
Thirty-eight digits with triggering were included. A single steroid injection into the tendon sheath was administered. Ultrasound findings and clinical symptoms, including pain, triggering, and the Quinnell score, were analyzed before injection and at 1 and 3 weeks after injection.
Results
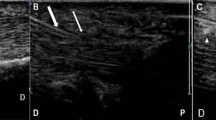
Ultrasound indicated that the thickness of the flexor tendons and the thickness of A1 pulleys were significantly greater in the trigger fingers than in controls before steroid injection. Three weeks after injection, these two parameters decreased, and there was no significant difference in the two parameters between the trigger finger and the controls. The visual analogue scales at 1 and 3 weeks after the injection were significantly lower than those before the injection. The Quinnell grading system scores significantly improved at 1 and 3 weeks after injection compared with the scores before injection. Moreover, a tendency was seen for the more clinically severe cases to show more swelling of the tendon and pulley.
Conclusion
In conclusion, ultrasound assessments could reveal that the thickened A1 pulley and flexor tendon significantly improved after steroid injection, which enables us to confirm the therapeutic effects of the steroid injection. Therefore, ultrasound assessments can be a useful adjunct to understand the response to treatment with the steroid injection.




Similar content being viewed by others


References
Strom L. Trigger finger in diabetes. J Med Soc N J. 1977;74:951–4.
Howard Jr LD, Pratt DR, Bunnell S. The use of compound F (hydrocortone) in operative and non-operative conditions of the hand. J Bone Joint Surg Am. 1953;35-A:994–1002.
Anderson B, Kaye S. Treatment of flexor tenosynovitis of the hand (‘trigger finger’) with corticosteroids. a prospective study of the response to local injection. Arch Intern Med. 1991;151(1):153–6.
Wilson SM, Roulot E, Le Viet D. Closed rupture of the thumb flexor tendon pulleys. J Hand Surg (Br). 2005;30:621–3.
Fornage BD, Rifkin MD. Ultrasound examination of the hand and foot. Radiol Clin North Am. 1988;26:109–29.
Bonvin F, Montet X, Copercini M, et al. Imaging of fractures of the lateral process of the talus, a frequently missed diagnosis. Eur J Radiol. 2003;47(1):64–70.
Quinnell RC. Conservative management of trigger finger. Practitioner. 1980;224:187–90.
Boutry N, Titecat M, Demondion X, Glaude E, Fontaine C, Cotten A. High-frequency ultrasonographic examination of the finger pulley system. J Ultrasound Med. 2005;24:1333–9.
Bianchi S, Martinoli C, Abdelwahab IF. High-frequency ultrasound examination of the wrist and hand. Skeletal Radiol. 1999;28:121–9.
Klauser A, Frauscher F, Bodner G, Halpern EJ, Schocke MF, Springer P, et al. Finger pulley injuries in extreme rock climbers: depiction with dynamic US. Radiology. 2002;222:755–61.
Jacob D, Cohen M, Bianchi S. Ultrasound imaging of non-traumatic lesions of wrist and hand tendons. Eur Radiol. 2007;17:2237–47.
Kim SJ, Lee CH, Choi WS, Lee BG, Kim JH, Lee KH. The thickness of the A2 pulley and the flexor tendon are related to the severity of trigger finger: results of a prospective study using high-resolution ultrasonography. J Hand Surg Eur. 2015;41:204–11.
Klauser A, Stadlbauer KH, Frauscher F, Herold M, Klima G, Schirmer M, et al. Value of transducer positions in the measurement of finger flexor tendon thickness by sonography. J Ultrasound Med. 2004;23:331–7.
Sampson SP, Badalamente MA, Hurst LC, Seidman J. Pathobiology of the human A1 pulley in trigger finger. J Hand Surg [Am]. 1991;16:714–21.
Niessen FB, Spauwen PH, Schalkwijk J, Kon M. On the nature of hypertrophic scars and keloids: a review. Plast Reconstr Surg. 1999;104:1435–58.
Muto T, Kokubu T, Mifune Y, Sakata R, Nagura I, Nishimoto H, et al. Platelet-rich plasma protects rotator cuff-derived cells from the deleterious effects of triamcinolone acetonide. J Orthop Res. 2013;31:976–82.
Ketchum LD, Robinson DW, Masters FW. The degradation of mature collagen: a laboratory study. Plast Reconstr Surg. 1967;40:89–91.
Mardani Kivi M, Lahiji FA, Jandaghi AB, Saheb Ekhtiari K, Hashemi MK. Efficacy of sonographically guided intra-flexoral sheath corticosteroid injection in the treatment of trigger thumb. Acta Orthop Traumatol Turc. 2012;46:346–52.
Kamhin M, Engel J, Heim M. The fate of injected trigger fingers. Hand. 1983;15:218–20.
Lee DH, Han SB, Park JW, Lee SH, Kim KW, Jeong WK. Sonographically guided tendon sheath injections are more accurate than blind injections: implications for trigger finger treatment. J Ultrasound Med. 2011;30:197–203.
Cecen GS, Gulabi D, Saglam F, et al. Corticosteroid injection for trigger finger: blinded or ultrasound-guided injection? Arch Orthop Trauma Surg. 2015;135(1):125–31.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
All authors declare that they have no conflicts of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Mifune, Y., Inui, A., Sakata, R. et al. High-resolution ultrasound in the diagnosis of trigger finger and evaluation of response to steroid injection. Skeletal Radiol 45, 1661–1667 (2016). https://doi.org/10.1007/s00256-016-2485-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-016-2485-5