
Abstract
Objective
Early clinical response to antidepressant treatment is an important therapeutic goal, considering the psychological, social and economic consequences of depression. The aim of the present study was to investigate the relationship between the time course of response and the concentration of venlafaxine (V), its active metabolite O-desmethylvenlafaxine (ODV) and enantiomeric ratios V(+)/V(−) and ODV(+)/ODV(−).
Methods
Depressed inpatients (n=35) received V orally at a fixed 300 mg daily dose. Accepted comedication included clorazepate (maximum 60 mg/day), zopiclone (maximum 15 mg/day) and low-dose trazodone (maximum 200 mg/day). Severity of depression was assessed on days 0, 4, 7, 11, 14, 21 and 28 (Montgomery and Åsberg Depression Rating Scale). Blood samples were taken on day 14 and day 28 and submitted to stereoselective determination. All measurements reflected trough steady-state values. First, pattern analysis was used to provide a categorical perspective of clinical response (50% improvement from baseline depression score). Patients displaying non-response, transient response, early persistent response and delayed persistent response were compared with respect to racemic concentrations and enantiomeric ratios. Second, in a dimensional perspective, mixed-effects modelling was used to analyse severity of depression versus time curves with respect to the possible influence of concentrations and enantiomeric ratios.
Results
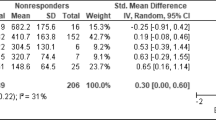
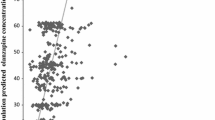
Comparison of patients with and without persistent response did not reveal any significant difference for V, ODV, V+ODV plasma levels or enantiomeric ratios. Persistent response was significantly associated with less frequent pre-study antidepressant medication and less frequent comedication with zopiclone (day 14) and clorazepate (day 28) during the study. Focus on patients with persistent response (n=19, 54.3%) indicated that early response, first observed before day 14, was associated with significantly higher V+ODV concentration than delayed response (median 725 ng/ml versus 554 ng/ml, P=0.023). No difference was found for pre-study medication or comedication during the study. Shorter time to onset of response was significantly associated with lower V(+)/V(−) enantiomeric ratio (rs=0.48, P<0.05). Mixed-effects modelling of depression severity versus time curves in patients with persistent response confirmed that either higher V+ODV plasma level or lower V(+)/V(−) ratio were significantly associated with more rapid decrease of depression score (likelihood ratio tests, P=0.012 and P=0.046, respectively).
Conclusion
Considering its modest sample size, naturalistic design and limited observation period, the present study provided preliminary indication that earlier clinical response may occur with higher V+ODV plasma level, extending previous dose-response studies. The hypothesis was also raised that exposure to a more potent noradrenergic therapeutic moiety, as reflected by a lower V(+)/V(−) ratio, may be relevant to early improvement of depression.



Similar content being viewed by others

References
Mendels J, Johnston R, Mattes J, Riesenberg R (1993) Efficacy and safety of b.i.d. doses of venlafaxine in a dose-response study. Psychopharmacol Bull 29:169–174
Kelsey JE (1996) Dose-response relationship with venlafaxine. J Clin Psychopharmacol 16:21S–26S
Rudolph RL, Fabre LF, Feighner JP, Rickels K, Entsuah R, Derivan AT (1998) A randomized, placebo-controlled, dose-response trial of venlafaxine hydrochloride in the treatment of major depression. J Clin Psychiatry 59:116–122
Preskorn SH (1994) Antidepressant drug selection: criteria and options. J Clin Psychiatry 55[Suppl A]:6–22
Khan A, Upton GV, Rudolph RL, Entsuah R, Leventer SM (1998) The use of venlafaxine in the treatment of major depression and major depression associated with anxiety: a dose-response study. J Clin Psychopharmacol 18:19–25
Derivan A, Entsuah AR, Kikta D (1995) Venlafaxine: measuring the onset of antidepressant action. Psychopharmacol Bull 31:439–447
Blier P, Bergeron R (1997) Early onset of therapeutic action in depression and greater efficacy of antidepressant treatments: are they related? Int Clin Psychopharmacol 12[Suppl3]:S21–S28
Nierenberg AA (2001) Do some antidepressants work faster than others? J Clin Psychiatry 62[Suppl15]:22–25
Roseboom PH, Kalin NH (2000) Neuropharmacology of venlafaxine. Depress Anxiety 12[Suppl1]:20–29
Guelfi JD, White C, Hackett D, Guichoux JY, Magni G (1995) Effectiveness of venlafaxine in patients hospitalized for major depression and melancholia. J Clin Psychiatry 56:450–457
Entsuah R, Derivan A, Kikta D (1998) Early onset of antidepressant action of venlafaxine: pattern analysis in intent-to-treat patients. Clin Ther 20:517–526
Benkert O, Grunder G, Wetzel H, Hackett D (1996) A randomized, double-blind comparison of a rapidly escalating dose of venlafaxine and imipramine in inpatients with major depression and melancholia. J Psychiatr Res 30:441–451
Entsuah AR, Huang H, Thase ME (2001) Response and remission rates in different subpopulations with major depressive disorder administered venlafaxine, selective serotonin reuptake inhibitors, or placebo. J Clin Psychiatry 62:869–877
Clerc GE, Ruimy P, Verdeau-Palles J (1994) A double-blind comparison of venlafaxine and fluoxetine in patients hospitalized for major depression and melancholia. Int Clin Psychopharmacol 9:139–143
Mehtonen OP, Sogaard J, Roponen P, Behnke K (2000) Randomized, double-blind comparison of venlafaxine and sertraline in outpatients with major depressive disorder. J Clin Psychiatry 61:95–100
Leon AC, Blier P, Culpepper L, Gorman JM, Hirschfeld RM, Nierenberg AA, Roose SP, Rosenbaum JF, Stahl SM, Trivedi MH (2001) An ideal trial to test differential onset of antidepressant effect. J Clin Psychiatry 62[Suppl4]:34–36
Katz MM, Halbreich UM, Bowden CL, Frazer A, Pinder RM, Rush AJ, Wheatley DP, Lebowitz BD (2002) Enhancing the technology of clinical trials and the trials model to evaluate newly developed, targeted antidepressants. Neuropsychopharmacology 27:319–328
Blier P (2003) The pharmacology of putative early-onset antidepressant strategies. Eur Neuropsychopharmacol 13:57–66
Tran PV, Bymaster FP, McNamara RK, Potter WZ (2003) Dual monoamine modulation for improved treatment of major depressive disorder. J Clin Psychopharmacol 23:78–86
Harvey AT, Rudolph RL, Preskorn SH (2000) Evidence of the dual mechanisms of action of venlafaxine. Arch Gen Psychiatry 57:503–509
Muth EA, Haskins JT, Moyer JA, Husbands GE, Nielsen ST, Sigg EB (1986) Antidepressant biochemical profile of the novel bicyclic compound Wy- 45,030, an ethyl cyclohexanol derivative. Biochem Pharmacol 35:4493–4497
Eap CB, Lessard E, Baumann P, Brawand-Amey M, Yessine MA, O’Hara G, Turgeon J (2003) Role of CYP2D6 in the stereoselective disposition of venlafaxine in humans. Pharmacogenetics 13:39–47
Gex-Fabry M, Rudaz S, Balant-Gorgia AE, Brachet A, Veuthey JL, Balant LP, Bertschy G (2002) Steady-state concentration of venlafaxine enantiomers: model-based analysis of between-patient variability. Eur J Clin Pharmacol 58:323–331
Charlier C, Pinto E, Ansseau M, Plomteux G (2002) Venlafaxine: the relationship between dose, plasma concentration and clinical response in depressive patients. J Psychopharmacol 16:369–372
Veefkind AH, Haffmans PMJ, Hoencamp E (2000) Venlafaxine serum levels and CYP2D6 genotype. Ther Drug Monit 22:202–208
Hoencamp E, Haffmans J, Dijken WA, Huijbrechts IP (2000) Lithium augmentation of venlafaxine: an open-label trial. J Clin Psychopharmacol 20:538–543
Bertschy G, Ragama-Pardos E, Aït-Ameur A, Muscionico M, Favre S, Roth L (2003) Lithium augmentation in venlafaxine non-responders: an open study. Eur Psychiatry 18:314–317
Quitkin FM, Rabkin JG, Ross D, Stewart JW (1984) Identification of true drug response to antidepressants. Use of pattern analysis. Arch Gen Psychiatry 41:782–786
Gibbons RD, Hedeker D, Waternaux C, Davis JM (1988) Random regression models: a comprehensive approach to the analysis of longitudinal psychiatric data. Psychopharmacol Bull 24:438–443
World Health Organization (1992) The ICD-10 classification of mental and behavioural disorders. Clinical descriptions and diagnostic guidelines. World Health Organization, Geneva
Montgomery SA, Åsberg M (1979) A new depression scale designed to be sensitive to change. Br J Psychiatry 134:382–389
Klamerus KJ, Parker VD, Rudolph RL, Derivan AT, Chiang ST (1996) Effects of age and gender on venlafaxine and O-desmethylvenlafaxine pharmacokinetics. Pharmacotherapy 16:915–923
Rudaz S, Stella C, Balant-Gorgia AE, Fanali S, Veuthey JL (2000) Simultaneous stereoselective analysis of venlafaxine and O-desmethylvenlafaxine enantiomers in clinical samples by capillary electrophoresis using charged cyclodextrins. J Pharm Biomed Anal 23:107–115
Khan A, Khan SR, Shankles EB, Polissar NL (2002) Relative sensitivity of the Montgomery-Åsberg Depression Rating Scale, the Hamilton Depression rating scale and the Clinical Global Impressions rating scale in antidepressant clinical trials. Int Clin Psychopharmacol 17:281–285
Hackett D (1998) Comparing onset of effect of antidepressants: pragmatic considerations on methods and end-points. Eur Psychiatry 13:117–123
Hedeker D, Gibbons RD (1996) MIXREG: a computer program for mixed-effects regression analysis with autocorrelated errors. Comput Methods Programs Biomed 49:229–252
Katz MM, Koslow SH, Frazer A (1996) Onset of antidepressant activity: reexamining the structure of depression and multiple actions of drugs. Depress Anxiety 4:257–267
Hirschfeld RM, Montgomery SA, Aguglia E, Amore M, Delgado PL, Gastpar M, Hawley C, Kasper S, Linden M, Massana J, Mendlewicz J, Moller HJ, Nemeroff CB, Saiz J, Such P, Torta R, Versiani M (2002) Partial response and nonresponse to antidepressant therapy: current approaches and treatment options. J Clin Psychiatry 63:826–837
Schweitzer I, Burrows G, Tuckwell V, Polonowita A, Flynn P, George T, Theodoros M, Mitchell P (2001) Sustained response to open-label venlafaxine in drug-resistant major depression. J Clin Psychopharmacol 21:185–189
Laska EM, Siegel C (1995) Characterizing onset in psychopharmacological clinical trials. Psychopharmacol Bull 31:29–35
Quitkin FM, Stewart JW, McGrath PJ, Nunes E, Ocepek-Welikson K, Tricamo E, Rabkin JG, Klein DF (1993) Further evidence that a placebo response to antidepressants can be identified. Am J Psychiatry 150:566–570
Lessard E, Yessine MA, Hamelin BA, O’Hara G, LeBlanc J, Turgeon J (1999) Influence of CYP2D6 activity on the disposition and cardiovascular toxicity of the antidepressant agent venlafaxine in humans. Pharmacogenetics 9:435–443
Thase ME (1999) Antidepressant treatment of the depressed patient with insomnia. J Clin Psychiatry 60[Suppl17]:28–31
Donovan SJ, Quitkin FM, Stewart JW, Ocepek-Welikson K, Harrison W, McGrath PJ, Nunes EV, Wager S, Tricamo E (1994) Duration of antidepressant trials: clinical and research implications. J Clin Psychopharmacol 14:64–66
Brunello N, Mendlewicz J, Kasper S, Leonard B, Montgomery S, Nelson J, Paykel E, Versiani M, Racagni G (2002) The role of noradrenaline and selective noradrenaline reuptake inhibition in depression. Eur Neuropsychopharmacol 12:461–475
Acknowledgement
This work was partially supported by a grant from Wyeth-Ayerst, Switzerland. The study complies with current laws in Switzerland.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gex-Fabry, M., Balant-Gorgia, A.E., Balant, L.P. et al. Time course of clinical response to venlafaxine: relevance of plasma level and chirality. Eur J Clin Pharmacol 59, 883–891 (2004). https://doi.org/10.1007/s00228-003-0710-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-003-0710-3