
Abstract
Summary
We found the risk of hip fracture was transiently elevated around twofold shortly after initiation of a loop or thiazide diuretic drug in a case-crossover and case–control study. No statistical association was found following the initiation of a comparator medication: ACE inhibitors. Awareness of these short-term risks may reduce hip fractures.
Introduction
Little is known about the acute effects of initiating a diuretic drug on risk of fracture. We evaluated the relationship between initiating a diuretic drug and the occurrence of hip fracture.
Methods
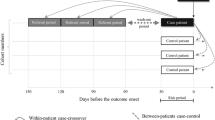
The study sample included 2,118,793 persons aged ≥50 years enrolled in The Health Improvement Network (THIN) between 1986 and 2010. The effect of a new start of a diuretic drug or comparator medication (ACE inhibitor) on risk of hip fracture was assessed using a case-crossover and case–control study during the 1–7, 8–14, 15–21, and 22–28 days following drug initiation.
Results
Included were 28,703 individuals with an incident hip fracture over a mean of 7.9 years follow-up. In the case-crossover study, the risk of experiencing a hip fracture was increased during the first 7 days following loop diuretic drug initiation (OR = 1.8; 95 % CI, 1.2, 2.7). The elevated risk did not continue during the 8–14, 15–21, or 22–28 days following drug initiation. For thiazide diuretics, the risk of hip fracture was elevated 8–14 days after drug initiation (OR = 2.2; 95 % CI, 1.2, 3.9). No such association was observed in the 1–7, 15–21, or 22–28 days following thiazide drug initiation. ACE inhibitor initiation was not associated with a statistically significant increased risk of hip fracture. Similar results were observed using a case–control study.
Conclusions
The risk of hip fracture was transiently elevated around twofold shortly after the new start of a loop or thiazide diuretic drug. Awareness of these short-term risks may reduce hip fractures and other injurious falls in vulnerable adults.


Similar content being viewed by others


References
Bolland MJ, Ames RW, Horne AM, Orr-Walker BJ, Gamble GD et al (2007) The effect of treatment with a thiazide diuretic for 4 years on bone density in normal postmenopausal women. Osteoporos Int 18:479–486
LaCroix AZ, Ott SM, Ichikawa L, Scholes D, Barlow WE (2000) Low-dose hydrochlorothiazide and preservation of bone mineral density in older adults. A randomized, double-blind, placebo-controlled trial. Ann Intern Med 133:516–526
Lim LS, Fink HA, Blackwell T, Taylor BC, Ensrud KE (2009) Loop diuretic use and rates of hip bone loss and risk of falls and fractures in older women. J Am Geriatr Soc 57:855–862
Rejnmark L, Vestergaard P, Heickendorff L, Andreasen F, Mosekilde L (2006) Loop diuretics increase bone turnover and decrease BMD in osteopenic postmenopausal women: results from a randomized controlled study with bumetanide. J Bone Miner Res 21:163–170
Woolcott JC, Richardson KJ, Wiens MO, Patel B, Marin J et al (2009) Meta-analysis of the impact of 9 medication classes on falls in elderly persons. Arch Intern Med 169:1952–1960
Rejnmark L, Vestergaard P, Mosekilde L (2005) Reduced fracture risk in users of thiazide diuretics. Calcif Tissue Int 76:167–175
Felson DT, Sloutskis D, Anderson JJ, Anthony JM, Kiel DP (1991) Thiazide diuretics and the risk of hip fracture. Results from the Framingham Study. JAMA 265:370–373
Schlienger RG, Kraenzlin ME, Jick SS, Meier CR (2004) Use of beta-blockers and risk of fractures. JAMA 292:1326–1332
Schoofs MW, van der Klift M, Hofman A, de Laet CE, Herings RM et al (2003) Thiazide diuretics and the risk for hip fracture. Ann Intern Med 139:476–482
Heidrich FE, Stergachis A, Gross KM (1991) Diuretic drug use and the risk for hip fracture. Ann Intern Med 115:1–6
Taggart HM (1988) Do drugs affect the risk of hip fracture in elderly women? J Am Geriatr Soc 36:1006–1010
Rejnmark L, Vestergaard P, Mosekilde L (2006) Fracture risk in patients treated with loop diuretics. J Intern Med 259:117–124
Carbone LD, Johnson KC, Bush AJ, Robbins J, Larson JC et al (2009) Loop diuretic use and fracture in postmenopausal women: findings from the Women's Health Initiative. Arch Intern Med 169:132–140
Maclure M (1991) The case-crossover design: a method for studying transient effects on the risk of acute events. Am J Epidemiol 133:144–153
Rodriguez LAG, Cea-Soriano L, Ruigomez A, Johansson S (2012) A UK Primary Care Study on Acid-Supressive Drugs and Hip Fracture: is there a link? GUT 60 (Supplement 3)
Wiens M, Etminan M, Gill SS, Takkouche B (2006) Effects of antihypertensive drug treatments on fracture outcomes: a meta-analysis of observational studies. J Intern Med 260:350–362
Aung K, Htay T (2011) Thiazide diuretics and the risk of hip fracture. Cochrane Database Syst Rev 10:CD005185
Solomon DH, Mogun H, Garneau K, Fischer MA (2011) Risk of fractures in older adults using antihypertensive medications. J Bone Miner Res 26:1561–1567
Leipzig RM, Cumming RG, Tinetti ME (1999) Drugs and falls in older people: a systematic review and meta-analysis: II. Cardiac and analgesic drugs. J Am Geriatr Soc 47:40–50
Berry SD, Mittleman MA, Zhang Y, Solomon DH, Lipsitz LA et al (2012) New loop diuretic prescriptions may be an acute risk factor for falls in the nursing home. Pharm Drug Saf 21:560–563
Rudy DW, Voelker JR, Greene PK, Esparza FA, Brater DC (1991) Loop diuretics for chronic renal insufficiency: a continuous infusion is more efficacious than bolus therapy. Ann Intern Med 115:360–366
Gribbin J, Hubbard R, Gladman J, Smith C, Lewis S (2011) Risk of falls associated with antihypertensive medication: self-controlled case series. Pharmacoepidemiol Drug Saf 20:879–884
van Staa TP, Dennison EM, Leufkens HG, Cooper C (2001) Epidemiology of fractures in England and Wales. Bone 29:517–522
Nyberg L, Gustafson Y, Berggren D, Brannstrom B, Bucht G (1996) Falls leading to femoral neck fractures in lucid older people. J Am Geriatr Soc 44:156–160
Klungel OH, Martens EP, Psaty BM, Grobbee DE, Sullivan SD et al (2004) Methods to assess intended effects of drug treatment in observational studies are reviewed. J Clin Epidemiol 57:1223–1231
Sennerby U, Melhus H, Gedeborg R, Byberg L, Garmo H et al (2009) Cardiovascular diseases and risk of hip fracture. JAMA 302:1666–1673
Acknowledgements and funding
This work was supported by a grant from the NIA (K23 AG033204), NIAMS (P60AR047785), Boston University School of Medicine, and the Men's Associates of Hebrew SeniorLife.
Conflicts of interest
The authors have no conflicts of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Appendix 1
Appendix 1
Read codes used to identify hip fracture are listed below. We considered a hip fracture using any procedural or diagnostic code as listed below.
7K1L400, 7K1L500, S30..00, S30..11, S300.00, S300000, S300100, S300200, S300300, S300311, S300400, S300500, S300600, S300700, S300800, S300900, S300A00, S300y00, S300y11, S300z00, S301.00, S301000, S301100, S301200, S301300, S301311, S301400, S301500, S301600, S301700, S301800, S301900, S301A00, S301y00, S301y11, S301z00, S302.00, S302000, S302011, S302012, S302100, S302200, S302300, S302400, S302z00, S303.00, S303000, S303011, S303012, S303100, S303200, S303300, S303400, S303z00, S304.00, S30w.00, S30x.00, S30y.00, S30y.11, S30z.00
Rights and permissions
About this article
Cite this article
Berry, S.D., Zhu, Y., Choi, H. et al. Diuretic initiation and the acute risk of hip fracture. Osteoporos Int 24, 689–695 (2013). https://doi.org/10.1007/s00198-012-2053-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-012-2053-3