
Purpose:
Since the 20th century, radiotherapy (RT) has been used for treatment of symptomatic splenomegaly (SM). SM occurs in association with hematologic disorders. The purpose of this analysis was to determine the indication, treatment concepts, and efficiency of RT.
Material and Methods:
Clinical features, treatment concepts, and outcome data during the past 20 years were analyzed. Endpoints were pain relief, symptomatic and hematological response, and treatment-related side effects.
Results:
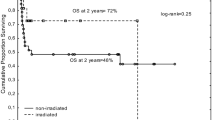
From 1989–2009, a total of 122 patients received 246 RT courses because of symptomatic SM. Overall 31 patients had chronic myelogenous leukemia (CML), 37 had chronic lymphocytic leukemia (CLL), 23 had osteomyelofibrosis (OMF), 17 had polycythemia vera (PV), 5 had acute myelogenous leukemia, 4 had idiopathic thrombocytopenic purpura (ITP), 3 had non-Hodgkin lymphoma (NHL), and 2 had multiple myeloma (MM). Patients were treated with 60Co gamma rays or 5–15MV photons. The fraction size ranged from 10–200 cGy and the total dose per treatment course from 30–1600 cGy. Significant pain relief was achieved for 74.8% of the RT courses given for splenic pain. At least 50% regression was attained for 77% of the RT courses given for SM. 36 patients died within 2 months due to the terminal nature of their disease. Of the RT courses applied for cytopenia, 73.6% achieved a significant improvement of hematological parameters and reduction of transfusion need. Notable hematologic toxicities were reported < EORTC/RTOG II°.
Conclusion:
The present analysis documents the efficacy of RT. In addition, RT as a palliative treatment option for symptomatic SM should not be forgotten.
Einleitung:
Seit Beginn des 20. Jahrhunderts hat die Radiotherapie (RT) ihren festen Stellenwert in der Behandlung einer symptomatischen Splenomegalie (SM). Die SM tritt bei hämatologischen Erkrankungen auf. Klinisch stehen Kapselschmerz sowie eine Zytopenie im Vordergrund. Die vorliegende Analyse untersucht Indikation, RT-Konzepte und die Effektivität der RT.
Material und Methode:
Patientendaten der letzten 20 Jahre wurden hinsichtlich klinischer Angaben, RT-Konzepte und Ergebnisse evaluiert. Endpunkte waren Schmerzfreiheit, hämatologisches Ansprechen nach RT sowie therapieassoziierte Nebenwirkungen.
Ergebnisse:
Zwischen 1989 und 2009 wurden 122 Patienten (79 Männer und 43 Frauen) mit insgesamt 246 RT-Serien behandelt. Folgende Grunderkrankungen waren Ursache für die Splenomegalie: CML (31), CLL (37), Osteomyelofibrose, (23), Polycyt haemia vera (17), AML (5), idiopathische Thrombozytopenie (4), Non-Hodgkin-Lymphom (3) und Plasmozytom (2) (Tabelle1). Die Behandlung erfolgte am Telekobalttherapiegerät oder am Linearbeschleuniger (5–15 MeV Photonen). Es wurden Einzelreferenzdosen zwischen 0,1–2 Gy und Gesamtreferenzdosen zwischen 3–16 Gy appliziert (Tabelle 2). Bei 74,8% der RT-Serien (74,8%), die aufgrund einer schmerzhaften Splenomegalie durchgeführt wurden, konnte eine Schmerzlinderung erzielt werden. Bei 77% der RT-Serien kam es zu einer Verkleinerung der Milz um bis zu 50% (Abbildung 1). 36 Patienten verstarben weniger als 2 Monaten nach Abschluss der RT im Rahmen der infausten Prognose ihrer Grunderkrankung. Bei 73,6% der RT-Serien kam es zu einer Verbesserung hinsichtlich Thrombozytopenien und die Transfusionsfrequenz nahm ab (Tabelle 3). Es wurden lediglich hämatologische Toxizitäten < II° (EORTC/RTOG) beobachtet.
Schlussfolgerung:
Die vorliegende Analyse belegt die hohe Effektivität der RT bei geringem Nebenwirkungsspektrum. Die RT der symptomatischen Splenomegalie sollte als wirksame palliative Option nicht in Vergessenheit geraten.
Similar content being viewed by others


References
Calverly D, Jones G, Kelton J. Splenic radiation for corticosteroid-resistant immune thrombocytopenia. Ann Intern Med 1992;116:977–81.
Dörr W, Herrmann T. Second tumors after oncologic treatment. Strahlenther Onkol 2008;184:67–72.
Eich HT, Heimann M, Kriz J et al. Long term outcome and prognostic factors in early stage nodal low-grade non Hodgkin’s lymphoma treated with radiotherapy. Strahlenther Onkol 2009;185:288–95.
Eich HT, Müller R-P, Engenhart-Cabillic R et al (2008) Involved node radiotherapy in early-stage Hodgkin’s lymphoma — definition and guidelines of the German Hodgkin Study Group (GHSG). Strahlenther Onkol 184:406–10.
Elliot MA, Chen MG Silverstein MN et al. Splenic irradiation for symptomatic splenomegaly associated with myelofibrosis with myeloid metaplasia. Br J Haematol 1998;103:505–11.
Elliot MA, Tefferi A. Splenic irradiation in myelofibrosis with myeloid metaplasia a review. Blood Rev 1999;13:163–70.
Guckenberger M, OK S, Polat B et al. Toxicity after intensity-modulated, image-guided radiotherapy for prostate cancer. Strahlenther Onkol 2010;186:535–43.
Greenberg JS, Chaffey JT, Rosenthal DS et al. Irradiation for control of hypersplenism and painful splenomegaly in myeloid metaplasia. Int J radiat Oncol Biol Phys 1977;2:1083–90.
Guiney MJ. A study of splenic irradiation in chronic lymphocytic leukemia. Int J Radiat Oncol Biol Phys 1988;16:225–9.
Kopecky J, Priester P, Slovacek L et al. Aplastic anaemia as a cause of death in a patient with glioblastoma multiforme treated with temozolomide. Starhlenther Onkol 2010;86:452–7.
Malmeus J, Akre T, Adami HO et al. Early postoperative course following elective splenectomy in hematological diseases: a high complication rate in patients with myeloproliferative disorders. Br J Surg 1986;73:720–3.
McFarland JT, Kuzma C, Millard et al. Palliative irradiation of the spleen. Am J Clin Oncol 2003;26:178–83.
Mesa RA, Tefferi A, Jacobsen SJ et al. The incidence and epidemiology of essential thrombocythemia and agnogenic myeloid metaplasia: an Olmsted County Study (Abstract). Blood 1997;90(Suppl 1):347a. sai]14._Mesa RA. How I treat symptomatic splenomegaly in patients with myelofibrosis. Blood 2009;113:5394–400.
Parmentier C, Charbord P, Tibi M et al. Splenic irradiation in myelofibrosis. Clinical findings and ferrokinetics. Int J Radiat Oncol Biol Phys 1977;2:1075–81.
Portaluri M, Fucilli F, Gianicolo E et al. Collection and evaluation of incidents in a radiotherapy department: a reactive risk analysis. Strahlenther Onkol 2010;186:693–9.
Claßen J, Nitzsche S, Wallwiener D et al. Fibrotic changes after postmastectomy radiotherapy and reconstructive surgery in breast cancer. A retrospective analysis in 109 patients. Strahlenther Onkol 2010;186:630–6.
Schratter-Sehn AU, Cerveny M, Simmel H et al. Short-time splenic irradiation for splenomegaly. Onkologie 2003;26:21–4.
Senn N. Case of spleno-medullary leukemia successfully treated by use of roentgen ray. Med Rec New York 1903;63:281.
Shrimali RK, Correa PD, O’Rourke N. Low-dose palliative splenic irradiation in haematolymphoid malignancy. J Med Imaging Radiat Oncol 2008;52: 297–302.
Spivak J. Idiopathic myelofibrosis. In: Harrison’s principles of internal medicine. San Francisco: McGraw-Hill 1998:682.
Wagner H Jr, McKeough PG, Desforges J et al. Splenic irradiation in the treatment of patients with chronic myelogenous leukemia or myelofibrosis with myeloid metaplasia. Results of daily and intermittend fraction with or without concomitant hydoxyurea. Cancer 1986;58:1204–7.
Weinmann M, Becker G, Einsele H et al. Clinical indications and biological mechanisms of splenic irradiation in chronic leukemias and myeloproliverative disordes. Radiother Oncol 2001;58:235–46.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kriz, J., Micke, O., Bruns, F. et al. Radiotherapy of splenomegaly. Strahlenther Onkol 187, 221–224 (2011). https://doi.org/10.1007/s00066-011-2252-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-011-2252-4