
Abstract
Purpose
This study investigates the interactions between midazolam premedication and propofol infusion induction of anesthesia for multiple anesthetic endpoints including: loss of verbal contact (LVC; hypnotic), dropping an infusion flex (DF; motor), loss of reaction to painful stimulation (LRP; antinociceptive) and attainment of electroencephalographic burst suppression (BUR; EEG).
Methods
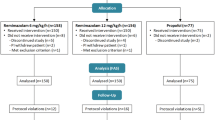
In a double blind, controlled, randomized and prospective study, 24 ASA I-II patients received either midazolam 0.05 mg· kg−1 (PM; n= 13) or saline placebo (P0; n=11)iv premedication. Twenty minutes later, anesthesia was induced by propofol infusion at 30 mg·kg−1· hr−1. ED50, ED95 and group medians for times and doses were determined and compared at multiple anesthetic endpoints.
Results
At the hypnotic, motor and EEG endpoints, midazolam premedication significantly and similarly reduced propofol ED50 (reduction: 18%, 13% and 20% respectively; P < 0.05 vs unpremedicated patients) and ED95 (reduction: 20%, 11% and 20% respectively; P < 0.05 vs unpremedicated patients). For antinociception (LRP), dose reduction by premedication was greater for propofol ED95 (reduction: 41 %; P < 0.05 vs unpremedicated patients) than ED50 (reduction: 18%; P < 0.05 vs unpremedicated patients). Hemodynamic values were similar in both groups at the various endpoints.
Conclusions
Midazolam premedication 20 min prior to induction of anesthesia reduces the propofol doses necessary to attain the multiple anesthetic endpoints studied without affecting hemodynamics in this otherwise healthy population. The interaction differs for different anesthetic endpoints (e.g., antinociception vs hypnosis) and propofol doses (e.g., ED50 vs ED95).
Résumé
Objectif
Examiner les interactions entre la prémédication avec du midazoiam et l’induction de l’anesthésie avec une perfusion de propofol en regard de divers paramètres comprenant: la perte du contact verbal (PCV; hypnotique), le relâchement de la main (RM; moteur), l’absence de réaction à une stimulation douloureuse (ARD; antinociceptif) et la suppression des salves d’activité électroencéphalographiques (SUP; EEG).
Méthodes
L’étude prospective, contrôlée, randomisée et à double insu concerne 24 patients ASA l-ll qui ont reçu, soit 0,05 mg· kg−1 de midazolam (PM; n = 13), soit une solution salée placebo (PO; n = 11) iv comme prémédication. L’anesthésie a été induite, 20 min plus tard, avec une perfusion de propofol à 30 mg· kg−1· hr−1. Les ED50, ED95 et les médianes pour les temps et les doses dans chaque groupe ont été déterminées et comparées pour divers paramètres anesthésiques.
Résultats
Pour les variables hypnotique, motrice et EEG, la prémédication au midazolam a réduit pareillement et de façon significative la ED50 de propofol (réduction: 18%, 13% et 20% respectivement; P < 0,05 vs les patients sans prémédication) et la ED95 (réduction: 20 %, 11% et 20% respectivement; P < 0,05 vs les patients sans prémédication). Concernant l’antinociception (ARD), la réduction de la dose par la prémédication a été plus importante pour la ED95 de propofol (réduction: 41%; P < 0,05 vs les patients sans prémédication) que pour la ED50 (réduction: 18%; P < 0,05 vs les patients sans prémédication). Les valeurs hémodynamiques ont été similaires chez les patients des deux groupes quant aux divers paramètres étudiés.
Conclusions
La prémédication avec du midazolam, 20 min avant l’induction de l’anesthésie, permet de réduire les doses de propofol nécessaires à l’atteinte des divers objectifs anesthésiques étudiés sans modifier l’hémodynamie chez une population de patients en bonne santé. Les interactions diffèrent en fonction des paramètres anesthésiques (ex., l’antinociception vs l’hypnose) et selon les doses de propofol (ex., ED50 vs ED95).
Article PDF
Similar content being viewed by others

References
Avram MJ, Sanghvi R, Henthorn TK, et al. Determinants of thiopental induction dose requirements. Anesth Analg 1993; 76: 10–7.
Jacobs JR, Reves JG. Effect site equilibration time is a determinant of induction dose requirement (Editorial). Anesth Analg 1993; 76: 1–6.
Wilder-Smith OHG, Ravussin PA, Decosterd LA, Despland PA, Bissonnette B. Midazolam premedication and thiopental induction of anaesthesia: interactions at multiple endpoints. Br J Anaesth 1999; 83: 590–5.
Short TG, Chui PT. Propofol and midazolam act synergistically in combination. Br J Anaesth 1991; 67: 539–45.
Short TG, Plummer JL, Chui PT. Hypnotic and anaesthetic interactions between midazolam, propofol and alfentanil. Br J Anaesth 1992; 69: 162–7.
Vinik HR, Bradley EL, Kissin L. Triple anesthetic combination: propofol-midazolam-alfentanil. Anesth Analg 1994; 78: 354–8.
Peacock JE, Spiers SP, McLauchlan GA, Edmondson WC, Berthoud M, Reilly CS. Infusion of propofol to identify smallest effective doses for induction of anaesthesia in young and elderly patients. Br J Anaesth 1992; 69: 363–7.
Naguib M, Sari-Kouzel A Thiopentone-propofol hypnotic synergism in patients. Br J Anaesth 1991; 67: 4–6.
Naguib M, Sari-Kouzel A, Seraj M, el-Gammal M, Gomma M. Induction dose-responses studies with propofol and thiopentone. Br J Anaesth 1992; 68: 308–10.
Van Hemelrijck J, Muller P, Van Aken H, White PF. Relative potency of eltanolone, propofol, and thiopental for induction of anesthesia. Anesthesiology 1994; 80: 36–41.
Oxorn DC, Terris LE, Harrington E, Orser BA. The effects of midazolam on propofol-induced anesthesia: propofol dose requirements, mood profiles, and perioperative dreams. Anesth Analg 1997; 85: 553–9.
Gentry WB, Krejcie TC, Henthorn TK, et al. Effect of infusion rate on thiopental dose-response relationships. Assessment of a pharmacokinetic-pharmacodynamic model. Anesthesiology 1994; 81: 316–24.
McAdam LC, MacDonald JT, Orser BA. Isobolographic analysis of the interactions between midazolam and propofol at GABA A receptors in embryonic mouse neurons. Anesthesiology 1998; 89: 1444–54.
Author information
Authors and Affiliations
Corresponding author
Additional information
Work was carried out at the Department of Anaesthesiology, Lausanne University Hospital (CHUV), Lausanne, Switzerland.
Financial Support: Partially supported by a grant from Roche Pharma (Switzerland) A.G.
Rights and permissions
About this article
Cite this article
Wilder-Smith, O.H.G., Ravussin, P.A., Decosterd, L.A. et al. Midazolam premedication reduces propofol dose requirements for multiple anesthetic endpoints. Can J Anesth 48, 439–445 (2001). https://doi.org/10.1007/BF03028305
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03028305