
Abstract
Purpose: To ultrasonically identify the presence of septae within the neurovascular sheath and to assess their effect on local anesthetic spread when performing infraclavicular brachial plexus blocks.
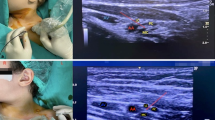
Clinical features: Thirty ASA status I and II patients scheduled for minor hand surgeries were enrolled in the study. Ultrasound guided infraclavicular brachial plexus blocks were performed on 28 patients. The images of the local anesthetic spread and the effect of the septum within the neurovascular sheath were analyzed. Septae were present in four of six patients where unilateral local anesthetic spread was seen. Septae were not visualized in the 22 patients with unrestricted local anesthetic spread after the initial injection. All 28 patients underwent their planned operations successfully with adequate anesthesia.
Conclusions: Our study shows that the presence of septae within the neurovascular sheath may influence the pattern of local anesthetic spread associated with the infraclavicular approach to brachial plexus blocks.
Résumé
Objectif: Identifier par échoguidage la présence de septa dans la gaine neurovasculaire et évaluer leur effet sur la diffusion de l’anesthésique local lors de blocs infraclaviculaires du plexus brachial.
Éléments cliniques: Trente patients ASA statut I et II devant subir des chirurgies mineures de la main ont participé à cette étude. Vingt-huit patients ont eu des blocs infraclaviculaires du plexus brachial échoguidés. Les images de la diffusion de l’anesthésique local et l’effet du septum dans la gaine neurovasculaire ont été analysés. Des septa étaient présents chez quatre des six patients chez qui on avait observé une diffusion unilatérale de l’anesthésique local. Aucun septum n’a été observé chez les 22 patients où la propagation de l’anesthésique local n’a pas été restreinte après l’injection initiale. Les chirurgies prévues chez les 28 patients se sont bien déroulées avec une anesthésie satisfaisante.
Conclusion: Notre étude montre que la présence de septa dans la gaine neurovasculaire peut influencer le mode de diffusion de l’anesthésique local associé à une approche infraclaviculaire pour les blocs du plexus brachial.
Article PDF
Similar content being viewed by others


References
Thompson GE, Rorie DK. Functional anatomy of the brachial plexus sheaths. Anesthesiology 1983; 59: 117–22.
Partridge BL, Katz J, Benirschke K. Functional anatomy of the brachial plexus sheath: implications for anesthesia. Anesthesiology 1987; 66: 743–7.
Lecamwasam H, Mayfield J, Rosow L, Chang Y, Carter C, Rosow C. Stimulation of the posterior cord predicts successful infraclavicular block. Anesth Analg 2006; 102: 1564–8.
Rodriguez J, Barcena M, Taboada-Muniz M, Lagunilla J, Alvarez J. A comparison of single versus multiple injections on the extent of anesthesia with coracoid infraclavicular brachial plexus block. Anesth Analg 2004; 99: 1225–30.
Gaertner E, Estebe JP, Zamfir A, Cuby C, Macaire P. Infraclavicular plexus block: multiple injection versus single injection. Reg Anesth Pain Med 2002; 27: 590–4.
Porter JM, McCartney CJ, Chan VW. Needle placement and injection posterior to the axillary artery may predict successful infraclavicular brachial plexus block: a report of three cases. Can J Anesth 2005; 52: 69–73.
Sandhu NS, Capan LM. Ultrasound-guided infraclavicular brachial plexus block. Br J Anaesth 2002; 89: 254–9.
Klaastad O, Smith HJ, Smedby O, et al. A novel infraclavicular brachial plexus block: the lateral and sagittal technique, developed by magnetic resonance imaging studies. Anesth Analg 2004; 98: 252–6.
Sauter AR, Smith HJ, Stubhaug A, Dodgson MS, Klaastad O. Use of magnetic resonance imaging to define the anatomical location closest to all three cords of the infraclavicular brachial plexus. Anesth Analg 2006; 103: 1574–6.
Chan VW, Perlas A, Rawson R, Odukoya O. Ultrasound-guided supraclavicular brachial plexus block. Anesth Analg 2003; 97: 1514–7.
Bloc S, Garnier T, Komly B, et al. Spread of injectate associated with radial or median nerve-type motor response during infraclavicular brachial-plexus block: an ultrasound evaluation. Reg Anesth Pain Med 2007; 32: 130–5.
Klaastad O, Smedby O, Thompson GE, et al. Distribution of local anesthetic in axillary brachial plexus block: a clinical and magnetic resonance imaging study. Anesthesiology 2002; 96: 1315–24.
Sandhu NS, Bahniwal CS, Capan LM. Feasibility of an infraclavicular block with a reduced volume of lidocaine with sonographic guidance. J Ultrasound Med 2006; 25: 51–6.
Author information
Authors and Affiliations
Corresponding author
Additional information
Funding source: None
Rights and permissions
About this article
Cite this article
Morimoto, M., Popovic, J., Kim, J.T. et al. Case series: Septa can influence local anesthetic spread during infraclavicular brachial plexus blocks. Can J Anesth 54, 1006–1010 (2007). https://doi.org/10.1007/BF03016635
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03016635