
Summary
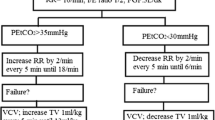
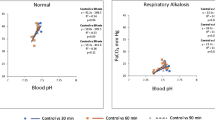
Respiratory alkalosis produced by ippb in patients undergoing cardiothoracic surgery may reduce cardiac output, facilitate the induction of cardiac arrhythmias, induce digitalis toxitity, decrease cerebral blood flow and shift the oxyhaemoglobin dissociation curve to the left. These effects are most threatening in patients undergoing cardiac surgery whose cardiac reserve is poor and whose myoeardial irritability is enhanced. This study was carried out in HO patients who underwent either open or closed heart surgery for acquired cardiac disease. Three groups of patients were each managed in a different way. Group a (48 patients) was ventilated with the carbon dioxide absorber in place and no carbon dioxide added to the breathing mixture; Group b (27 patients) had the carbon dioxide absorber eliminated from the circuit; and Group c (35 patients) had the carbon dioxide absorber eliminated from the circuit and 2.5 per cent carbon dioxide added to the breathing mixture. All patients were ventilated with tidal volumes which were 1,5 to 3.4 times greater than those recommended by Radford. All had satisfactory Pco2. The Paco2 and pH were significantly different for the three groups. The mean Paco2 for Groups a, b, and c were 30.6, 36.7, and 44.7 mm Hg respectively. An arterial pH greater than 7.44 was observed in 88 per cent of Group à and 33 per cent of Group b, but in only 6 per cent of Group c patients. A greater latitude in ventilatory volume was permissible in Group c subjects to attain à homogeneous result within à desired range of Paco2 levels. Severe acidaemia was not à problem. This study shows that respiratory alkalosis can be avoided while maintaining suitable oxygenation without risk of respiratory acidaemia in patients undergoing cardiac surgery. Empirically, this can be predictably obtained by the use of at least 6 liters of fresh gas, tidal volumes 2.0 to 2.5 times that calculated from the Radford nomogram, removal of the carbon dioxide absorber and addition of 2.5 per cent of carbon dioxide and 50 per cent of oxygen to the inspired mixture.
Résumé
L’alcalose respiratoire produite par la ippb chez des malades soumis à de la chirurgie cardiothoracique peut diminuer le débit cardiaque, prélisposer à 1’apparition d’arythmies, favoriser une intoxication digitalique, diminuer le débit sanguin cerebal et pousser vers la gauche le courbe de dissociation de l’oxy-hémoglobine. Ces effets sont plus pénibles pour Ies malades soumis à la chirurgie cardiaque dont la réserve cardiaque est Iimitée et dont 1’irritabilité cardiaque est accrue. Notre etude a porté sur 110 malades soumis à de la chirurgie cardiaque à coeur ouvert ou fermé pour des maladies cardiaques acquises. Nous avons partagé les malades en trois groupes et chacun de ces groupes a été traiti de façon différente. Le groupe à (48 malades) a été ventilé alors que l’absorbant du CO2 était en place et nous n’avons pas ajouté de CO2 dans le mélange inspiré le groupe b (27 malades) a été ventilé sans absorbant de CO2 et nous avons ajouté au mélange inspiré un taux de 2.5 pour cent de CO2. Nous avons ventilé tous Ies malades avec un air courant qui était de 1.5 à 3.4 fois plus grand que ceux mentionnés par Radford. Tous Ies malades avaient une Pao., satisfaisante. La Paco2 et le pH útaient legerement differents d’un groupe à Tautre. Pour chacun des groupes a.b.c., la Paco2 moyenne était respectivement de 30.6, 36.7 et 44.7 mm Hg. Chez 88 pour cent des malades du groupe a, nous avons observé un pH au-dessus de 7.44; chez Ies malades du groupe B, la même observation a été faite chez 33 pour cent des malades et chez Ies malades du groupe c, seulement chez 6 pour cent.
Chez Ies malades du groupe c, nous avons toléré une plus grande latitude dans le volume de ventilation pour obtenir un résultat bomogène en deça de lirnites désirées des taux de Paco2 L’acidhémie grave n’a pas été un probléme. Cette étude prouve que l’alcalose respiratoire peut être évitée tout en maintenant une oxygénation convenable sans risque d’acidhémie respiratoire chez des malades soumis à la chirurgie cardiaque. Empiriquement, ceci peut être obtenu de façon prévisible en utihsant un débit d’au moins 6 litres de gaz frais, un air courant de 2 à 2.5 fois plus grand que celui mentionné dans le nomogramme de Radford, en enlevant 1’absorbant du gaz carbonique (CO2) et l’addition de 2.5 pour cent de CO2 et 50 pour cent d’oxygéne dans l’air inspiré.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Cournand, A., Motley, H. L., Werks, L., & Richards, D. W., Jr., Physiological studies of effects of intermittent positive pressure breathing on cardiac output in man. Am. J. Physiol.,152: 162 (1948).
Theye, R. A., Milde, J. H., &Michenfeldeb, J. D. Effect of hypocapnia on cardiac output during anesthesia, Anesthesiology,72: 778 (1966).
Prys-Robebts, C., Kelman, G. R., Kain, M. L., Gbeenbaum, R., &Bay, J. Cardiac output and blood carbon dioxide levels during halothane anesthesia in man. Brit. J. Anaesth.,39: 687 (1967).
Morgan, B. C., Crawford, E. W.,Hohnbein, T. F., MaBtin, W. E., &Guntheroth, W. G. Hemodynamie effects of changes in arterial carbon dioxide tension during intermittent positive pressure ventilation. Anesthesiology,28: 866 (1967).
Cullen, D. J., Eger, E. I., II, &Gregory, G. A., The cardiovascular effects of carbon dioxide in man, conscious and during cyclopropane anesthesia. Anesthesiology,31: 407 (1969).
Wright, B. D. &Digiovanni, A. J. Respiratory alkalosis, hypokalemia, and repeated ventricular fibrillation associated with mechanical ventilation. Anesth. & Aanlg.,48: 487 (1969).
Flemma, R. J. & Young, W. G., Jr, The metabolic effects of mechanical ventilation and respiratory alkalosis in postoperative patients. Surgery,56: 36 (1964).
Scribner, G. H., Fremont-Smith, K., &Burneix, J. M. The effect of acute respiratory acidosis on the internal equilibrium of potassium. J. din. Invest.,34: 1276 (1955),
Haix, K. D. &Vartanian, V. Control of serum potassium levels in the hyperventilated postoperative cardiac patient. South. M. J.,61: 416 (1958).
Sokcmloff, L. The action of drugs on the cerebral circulation. Pharmacol. Rev.,11: 1 (1959).
Alexander, S. C., Cohen, P. J., Wollman, H., Smith, T. C., Reivich, M., &Vander Molen, R. A. Cerebral carbohydrate metabolism during hypocarbia in man, Anesthesiology,26: 624 (1965).
Fhoman, C. Adverse effects of low carbon dioxide tensions during mechanical over-ventilation of patients with combined head and chest injuries. Brit. J. Anaesth.,40: 383 (1968).
Anderson, O. S. &Engel, K. A. A new acid-base nomogram. An improved method for the calculation of the relevant blood acid-base data, Scandinav. J. Clin. & Lab. Invest.,12: 177 (1960).
RADFORD, E. P., Jr. Ventilation standards for use in artificial respiration, J. Appl. Physiol.,7: 451 (1955).
Gold, M. I. &Helrich, M. Ventilation and blood gases in anesthetized patients. Canad. Anaesth. Soc. J.,14: 424 (1967).
Johnstone, M. Hypocapnic vasoconstriction during halothane anaesthesia in surgical patients. Brit. J. Anaesth.,40: 602 (1968).
Huckabee, W. E. Relationship of pyruvate and lactate during anaerobic metabolism. Effects of infusion of pyruvate or glucose and of hyperventilation, J. Clin. Invest.,37: 244 (1958).
Allan-Carson, S. A. &MoRris, L. E. Controlled acid-base status with cardiopulmonaiy bypass and hypothermia, Anesthesiology,23: 618 (1962).
Nunn, J. F., Bergman, N. A., &Coleman, A. J. Factors influencing the arterial oxygen tension during anesthesia with artificial ventilation. Brit. J. Anaesth..,37: 898 (1965).
Bendixen, H. H., Hedley-Whyte, J., &Laver, M. B. Impaired oxygenation in surgical patients during general anesthesia with controlled ventilation. A concept of atelectasis. New England J. M.,269: 991 (1963).
Babaka, A., Smith, C. O., &Shroff, P. E. Controlled normocarbia during IPPB with the Emerson anesthetic ventilator. Anesthesiology,32: 369 (1970).
Ocbo, E. M. &TeRRY, R. N. Proposed formula for ventilatory requirements in apneic anesthetized patients. Anesth. & Analg.,48: 455 (1969).
Keeri-Szanto, M. Isokapnic ventilation during surgical operations: Description of equipment and first results. Anesth. & Analg.,49: 406 (1970).
Suwa, K. &Yamamura, H. The effect of gas inflow on the regulation of CO2 levels with hyperventilation during anesthesia, Anesthesiology,33: 440 (1970).
Suwa, K., Geffin, B., Pontoppidan, H., &Bendixen, H. H., A Nomogram for deadspace requirement during prolonged artificial ventilation. Anesthesiology,29: 1206 (1968).
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Lipton, B., Kahn, M. Carbon dioxide and large volume ventilation in the management of patients undergoing cardiac surgery. Canad. Anaesth. Soc. J. 19, 49–59 (1972). https://doi.org/10.1007/BF03006907
Issue Date:
DOI: https://doi.org/10.1007/BF03006907