
Abstract
Background
We describe institutional vasopressor usage, and examine the effect of vasopressors on hemodynamics: heart rate (HR), mean arterial blood pressure (MAP), intracranial pressure (ICP), cerebral perfusion pressure (CPP), brain tissue oxygenation (PbtO2), and jugular venous oximetry (SjVO2) in adults with severe traumatic brain injury (TBI).
Methods
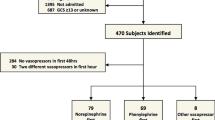
We performed a retrospective analysis of 114 severely head injured patients who were admitted to the neurocritical care unit of Level 1 trauma center and who received vasopressors (phenylephrine, norepinephrine, dopamine, vasopressin or epinephrine) to increase blood pressure
Results
Phenylephrine was the most commonly used vasopressor (43%), followed by norepinephrine (30%), dopamine (22%), and vasopressin (5%). Adjusted for age, gender, injury severity score, vasopressor dose, baseline blood pressure, fluid administration, propofol sedation, and hypertonic saline infusion, phenylephrine use was associated with 8 mmHg higher mean arterial pressure (MAP) than dopamine (P = 0.03), and 12 mmHg higher cerebral perfusion pressure (CPP) than norepinephrine (P = 0.02) during the 3 h after vasopressor start. There was no difference in ICP between the drug groups, either at baseline or after vasopressor treatment.
Conclusions
Most severe TBI patients received phenylephrine. Patients who received phenylephrine had higher MAP and CPP than patients who received dopamine and norepinephrine, respectively.



Similar content being viewed by others


References
Selassie AW, Zaloshnja E, Langlois JA, et al. Incidence of long-term disability following traumatic brain injury hospitalization, United States, 2003. J Head Trauma Rehabil. 2008;23(2):123–31.
Rutland-Brown W, Langlois JA, Thomas KE, et al. Incidence of traumatic brain injury in the United States, 2003. J Head Trauma Rehabil. 2006;21(6):544–8.
Vavilala MS, Lee LA, Lam AM. Cerebral blood flow and vascular physiology. Anesthesiol Clin North America. 2002;20(2):247–64.
Jünger EC, Newell DW, Grant GA, et al. Cerebral autoregulation following minor head injury. J Neurosurg. 1997;86(3):425–32.
Sahuquillo J, Munar F, Baguena M, et al. Evaluation of cerebrovascular CO2-reactivity and autoregulation in patients with post-traumatic diffuse brain swelling (diffuse injury III). Acta Neurochir Suppl. 1998;71:233–6.
Brain Trauma Foundation, American Association of Neurological Surgeons, Congress of Neurological Surgeons, Joint Section on Neurotrauma and Critical Care, AANS/CNS, Bratton SL, Chestnut RM, Ghajar J, et al. Guidelines for the management of severe traumatic brain injury. I. Blood pressure and oxygenation. J Neurotrauma. 2007;24:S7–13.
Brain Trauma Foundation, American Association of Neurological Surgeons, Congress of Neurological Surgeons, Joint Section on Neurotrauma and Critical Care, AANS/CNS, Bratton SL, Chestnut RM, Ghajar J, et al. Guidelines for the management of severe traumatic brain injury. IX. Cerebral perfusion thresholds. J Neurotrauma. 2007;24:S59–64.
Bouma GJ, Muizelaar JP. Relationship between cardiac output and cerebral blood flow in patients with intact and with impaired autoregulation. J Neurosurg. 1990;73(3):368–74.
Ract C, Vigué B. Comparison of the cerebral effects of dopamine and norepinephrine in severely head-injured patients. Intensive Care Med. 2001;27(1):101–6.
Steiner LA, Johnston AJ, Czosnyka M, et al. Direct comparison of cerebrovascular effects of norepinephrine and dopamine in head-injured patients. Crit Care Med. 2004;32(4):1049–54.
Johnston AJ, Steiner LA, Chatfield DA, et al. Effect of cerebral perfusion pressure augmentation with dopamine and norepinephrine on global and focal brain oxygenation after traumatic brain injury. Intensive Care Med. 2004;30(5):791–7.
Bulger EM, Nathens AB, Rivara FP, et al. Management of severe head injury: institutional variations in care and effect on outcome. Crit Care Med. 2002;30:1870–6.
Drummond JC, Shapiro HM. Cerebral physiology. In: Miller RD, editor. Anesthesia. Edinburgh: Churchill Livingstone; 1994. p. 689–730.
Rosner MJ, Rosner SD, Johnson AH, et al. Cerebral perfusion pressure: management protocol and clinical results. J Neurosurg. 1995;83(6):949–62.
Bevan JA, Duckworth J, Laher I, et al. Sympathetic control of cerebral arteries: specialization in receptor type, reserve, affinity, and distribution. FASEB J. 1987;1(3):193–8.
Starkey K, Docherty J. Alpha 1 and alpha 2 adrenoreceptors: pharmacology and clinical implications. J Cardiovasc Pharmacol. 1981;3(Suppl 1):514–6.
Guimarães S, Moura D. Vascular adrenoceptors: an update. Pharmacol Rev. 2001;53(2):319–56.
Kroppenstedt SN, Sakowitz OW, Thomale UW, et al. Norepinephrine is superior to dopamine in increasing cortical perfusion following controlled cortical impact injury in rats. Acta Neurochir Suppl. 2002;81:225–7.
Kroppenstedt SN, Sakowitz OW, Thomale UW, et al. Influence of norepinephrine and dopamine on cortical perfusion, EEG activity, extracellular glutamate, and brain edema in rats after controlled cortical impact injury. J Neurotrauma. 2002;19(11):1421–32.
Dudkiewicz M, Proctor KG. Tissue oxygenation during management of cerebral perfusion pressure with phenylephrine or vasopressin. Crit Care Med. 2008;36(9):2641–50.
Stubbe HD, Greiner C, Westphal M, et al. Cerebral response to norepinephrine compared with fluid resuscitation in ovine traumatic brain injury and systemic inflammation. Crit Care Med. 2006;34(10):2651–7.
Cherian L, Chacko G, Goodman JC, et al. Cerebral hemodynamic effects of phenylephrine and L-arginine after cortical impact injury. Crit Care Med. 1999;27(11):2512–7.
Ract C, Vigué B, Bodjarian N, et al. Comparison of dopamine and norepinephrine after traumatic brain injury and hypoxic-hypotensive insult. J Neurotrauma. 2001;18:1247–54.
Malhotra AK, Schweitzer JB, Fox JL, et al. Cerebral perfusion pressure directed therapy following traumatic brain injury and hypotension in swine. J Neurotrauma. 2003;20(9):827–39.
Beaumont A, Hayasaki K, Marmarou A, et al. Contrasting effects of dopamine therapy in experimental brain injury. J Neurotrauma. 2001;18(12):1359–72.
Feinstein AJ, Patel MB, Sanui M, et al. Resuscitation with pressors after traumatic brain injury. J Am Coll Surg. 2005;201(4):536–45.
Kroppenstedt SN, Thomale UW, Griebenow M, et al. Effects of early and late intravenous norepinephrine infusion on cerebral perfusion, microcirculation, brain-tissue oxygenation, and edema formation in brain-injured rats. Crit Care Med. 2003;31(8):2211–21.
Robertson CS, Valadka AB, Hannay HJ, et al. Prevention of secondary ischemic insults after severe head injury. Crit Care Med. 1999;27(10):2086–95.
Acknowledgment
Funding
This work was funded by Departmental Sources.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sookplung, P., Siriussawakul, A., Malakouti, A. et al. Vasopressor Use and Effect on Blood Pressure After Severe Adult Traumatic Brain Injury. Neurocrit Care 15, 46–54 (2011). https://doi.org/10.1007/s12028-010-9448-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-010-9448-9