
Abstract
Bcl I in the promoter polymorphism observed within h-GR/NR3C1 gene may play an important role in the development of bronchial asthma and resistance to GCs in the severe bronchial asthma. The aim of the investigation was to study the correlation between this h-GR/NR3C1 gene polymorphism and occurrence of asthma in the population of Polish asthmatics. Peripheral blood was obtained from 70 healthy volunteers and 59 asthma patients. Structuralized anamnesis, spirometry and allergy skin prick tests were performed in all participants. Genotyping was carried out with PCR–RFLP method. In healthy, non-atopic population variants of Bcl I: GG, GC, CC were found with frequency 0.129/0.471/0.400, respectively. In asthma patients Bcl I: GG, GC, CC occurred with respective frequencies of 0.410/0.462/0.128. Chi-square analysis revealed a significantly different (P < 0.05) distribution between cases and controls for the Bcl I polymorphism. The Bcl I polymorphism of h-GR/NR3C1 gene is significantly associated with bronchial asthma, susceptibility to the development of severe form and resistance to GCs in Polish population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Bronchial asthma is a disease with multifactor etiology [1]. The mutual correlations among the groups of factors predisposing to the development of the disease and the prevalence of asthma are complex in character [2]. The hereditary component of asthma is determined polygenetically [3]. The environmental component is implied significantly by neuroimmune reactions occurring at the molecular level. It should be emphasized that bronchial asthma is a disorder whose primary cause can probably be traced in the disturbed immunoregulatory mechanisms at the lymphocyte level, with secondary overproduction of IgE class antibodies and allergic inflammatory condition [3]. Glucocorticosteroids (GCS) constitute the basic group of medications used to control inflammatory conditions in patients with bronchial asthma. They exert a multidirectional and specific effect on various cell types. They regulate the expression of specific genes within the cell nuclei via the corticosteroid/receptor complex/receptor (GCS/GR) [4].
Glucocorticosteroid resistance is a complex problem [5]. It may be constitutional in character, or develop as a sequel to an inflammatory process. It should be emphasized that each tissue represents different sensitivity to GCS. There are serious doubts whether we are born with steroid-resistant asthma, or we acquire it during our lifetime, i.e. if it is dependent on genetic or environmental factors.
The genes involved in increased production of allergen-specific IgE class antibodies (atopy), bronchial hyperreactivity, production of inflammatory response mediators, and Th1 and Th2 lymphocyte population sizes play a role in the etiopathogenesis of the disease [6, 7]. It is notable that the results of search for the gene or genes predisposing for the development of atopy or bronchial asthma obtained so far are not consistent, and the research is still going on.
The human glucocorticoid receptor gene/nuclear receptor subfamily 3, group C, member 1 gene h-GR/NR3C1 is localized on chromosome 5q31–q32 and consists of nine exon [8]. The mRNA transcript for h-GR/NR3C1 gene protein undergoes splicing, which leads to the formation of four mRNA isoforms: GRα, GRβ, GRδ and GRγ [9, 10]. The only active form of the receptor is GRα. The remaining isoforms are post-transcriptional modifications of the h-GR/NR3C1 gene lacking the full potential [3]. The glucocorticoid receptor is a protein made up of a single polypeptide chain consisting of 777 amino acids [11]. A few domains can be distinguished within the receptor. Domain C, which is the carrier of immunogenicity and other biological characteristics, is located between amino acids 1–421, which account for a half of the receptor size. The central GR area (between amino acids 421–486) is responsible for DNA binding (domain B). It contains cysteine residues forming complexes with zinc, facilitating DNA binding and determining its tertiary structure. In the terminal portion of the receptor molecule, there is a segment (domain A) which controls binding of a hormone molecule—GCS [12]. The molecular mechanism of action of GCS involves binding of the specific ligand/glucocorticoid receptor to the sequences of regulator genes encoding the synthesis of anti-inflammatory proteins determining the clinical effects of GCS.
Resistance to GCS at the molecular level results from many mechanisms modifying the function of GR in the cells. Reduced response to drugs of this group can be explained by decreased expression of GR, impairment of their ability to bind DNA, or enhanced expression of transcriptional factors.
Currently, a complex mechanism of GCS resistance development in patients with severe bronchial asthma is postulated. Schwartz et al. [13] associated it with various mechanisms related to GR function, Carmichael et al. [14] studied the density of complement receptors on monocytes and demonstrated no changes in GR expression after administration of GCS, Corrigan et al. [15] described reduced GR affinity to the ligand as a result of p38MAP kinase activation by IL-2 and IL-4, Adcock et al. [16] demonstrated development of GCS resistance associated with increased AP-1 (activator protein 1) activity, or increased affinity of AP-1 to GR.
Polymorphisms present within the h-GR/NR3C1 gene may inhibit formation of GR/GCS complexes, reduce transcription and cause transrepression of the genes encoding proteins synthesized within the framework of cellular response to GCS [17]. Bcl I RFLP is formed as a result of changes in a single base. A C/G single nucleotide polymorphism (SNP) within the h-GR/NR3C1 gene promoter has been localized in the intron 647 bp away from the exon/intron binding site. Allele G is particularly associated with sensitivity to GCS. It increases the cellular response to GCS and occurs less frequently than allele C [17–19]. Polymorphism Bcl I (C>G) within h-GR/NR3C1 gene promoter demonstrates correlations with sensitivity to steroids, multiple sclerosis and hypothalamo-pituitary-adrenal axis [20].
Because of complex etiopathogenesis of bronchial asthma, its heterogeneous nature, incomplete gene penetration, presence of phenocopies, differentiated gene expression and gene–gene interactions, thorough investigation of molecular mechanisms leading to the development of bronchial asthma is a difficult problem, which requires continuous evaluation [21].
The aim of the investigation was to study the correlation between Bcl I single nucleotide polymorphism of h-GR/NR3C1 gene promoter and occurrence of bronchial asthma in the Polish population.
Materials and methods
The study was approved by the local ethics committee (Consent of Research Review Board at the Medical University of Lodz, Poland, No RNN/133/09/KE). At the commencement of the study, participants were invited to attend voluntarily. Before admission, written informed consent was obtained from every patient.
The study was conducted in a group of 55 patients with bronchial asthma. Asthma diagnosis was established according to GINA recommendations, based on clinical asthma symptoms and lung function test. The control arm included a group of 70 healthy adults, who met the following criteria: no history or symptoms of either bronchial asthma, or other pulmonary diseases, no history or symptoms of allergy, no history or symptoms of atopic dermatitis, no history or signs of hypersensitivity to aspirin, negative results of skin tests for 12 common allergens, no first-degree relatives with bronchial asthma or atopic disorders.
Venous blood samples were collected from the participants onto EDTAK3, DNA was obtained from peripheral blood leukocyte fraction. The genetic material was isolated using Wizard DNA Isolation Kit (Promesa, Madison, WI) according to the guidelines provided by the manufacturer. The investigated polymorphisms were analyzed using PCR–RFLP method.
Amplification of DNA segments for Bcl I polymorphism was conducted using a forward primer (5′-GAG AAA TTC ACC CCT ACC AAC-3′) and a reverse primer (5′-AGA GCC CTA TTC TTC AAA CTG-3′) according to standard PCR protocol. Starter binding to complementary DNA matrix sites was accomplished at 56°C. Amplified DNA sequences of 418 bp length were obtained. The material was incubated with Bcl I restriction enzyme (New England Biolabs, Neverly, MA) at 50°C for 10 h. DNA fragments containing 263 and 151 bp identified as a set of representative, typical (wild type) alleles were obtained, as well as segments with 418, 263 and 151 bp. RFLP of 418 bp length was identified as the set of polymorphic alleles. RFLP products were separated by electrophoresis on 2% agarose gel, stained with ethidine bromide and observed in UV light. Representative, typical homozygotes, as well as heterozygotes were sequenced and used as internal control.
The obtained results were subjected to descriptive statistical analysis with calculation of arithmetic means and standard deviations. The significance of differences between mean values was determined by means of Chi2, with P < 0.05 adopted as the significance level.
Results
The control group consisted of 70 healthy volunteers (women 48.6%, men 51.4%), aged on the average 63.11 years, SD ± 5.00, with the youngest subject 55 and the oldest 75 years old, bias 0.19, standard error of the bias 0.28. The following frequencies of Bcl I polymorphism of h-GR/NR3C1 gene promoter—GG, GC, CC—were obtained: 0.129/0.471/0.400, respectively. The group of asthmatic patients consisted of 59 healthy volunteers (women 71.2%, men 28.8%), aged on the average 50.81 years, SD ± 13.65, with the youngest subject 23 and the oldest 77 years old, bias −0.32, standard error of the bias 0.31. The following frequencies of Bcl I polymorphism of h-GR/NR3C1 gene promoter—GG, GC, CC—were obtained: 0.436/0.455/0.109, respectively. Comprehensive comparison of the analyzed groups is presented in Table 1.
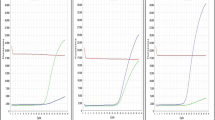
The alleles of the investigated polymorphism in both groups demonstrate distribution consistent with Hardy–Weinberg equilibrium [22–24]. Figure 1 illustrates de Finetti distributions of the investigated genotypes [25–27].

De Finetti diagram with Hardy–Weinberg parabola was drawn using The Helmholtz Zentrum München free software, Germany. Description of diagram: black line—controls; blue lines— cases. (Color figure online)
Significant statistical differences between the investigated genotypes were demonstrated (P < 0.05). Patients with bronchial asthma presented allele G of the investigated Bcl I polymorphism significantly more frequently. The frequency of allele G versus C correlated with increased occurrence of bronchial asthma in the investigated population (OR = 3.44, CI: 95% confidence interval, CI = 2.03–5.81, χ2 = 22.08, P = 2.61e-06). Genotype GG versus CC was characterized by OR = 12.44, CI: 95% confidence interval, CI = 3.87–540.01, χ2 = 20.55 with P = 5.82e-06. The carriers of allele G (GG + GC) versus CC developed bronchial asthma significantly more often (OR = 5.44, CI: 95% confidence interval, CI = 2.05–14.41, χ2 = 13.16, P = 0.00029). Mutation SNP G/C within the Bcl I polymorphism of h-GR/NR3C1 gene promoter had a protective effect and reduced the risk of developing bronchial asthma. The occurrence of allele C versus G reduced in a statistically significant manner the risk of the disease (OR = 0.29, CI: 95% confidence interval, CI = 0.17–0.049, χ2 = 22.08, P = 2.61e-06). The carriers of allele C (CC + CG) developed bronchial asthma significantly less frequently (OR = 0.08, CI: 95% confidence interval, CI = 0.02-0.25, χ2 = 20.55, P = 5.82e-06.) Table 2 contains the description of statistics for the analyzed genotype frequencies.
No intra- and inter-group correlations among the gender, occurrence of allergy and age (P > 0.05) were demonstrated.
Discussion
Bronchial asthma is a disease with multifactor etiology. It develops on the background of mutual interactions between genetic and environmental factors. Numerous studies have confirmed that various responses to GCS can be observed in healthy population. The genetic variability with respect to SNPs and mutual gene–gene interactions are the important elements in the development of bronchial asthma. The key loci determining the development of this disease are localized in chromosome 5q31–q32 (gene encoding IL-3, IL-4, IL-5, IL-9, IL-13, GM-CSF, CD14, LTC4S as well as h-GR/NR3C1 and β2-adrenergic receptor).
The tissue specificity of GCS effect on the transcription of genes encoding the synthesis of anti-inflammatory proteins, determining the therapeutic effect, is dependent on many factors. Numerous regulatory elements of DNA within the h-GR/NR3C1 gene promoter, coactivator proteins, cAMP activity, as well as complex protein kinase signal pathways play the crucial role here [3, 28–32]. Binding of the GCS-GR complex with the DNA of regulator gene sequences is a key signal for co-activator proteins CBP (CREB Winding protein) and pCAF (CBP associated factor) as well as SRC-1 (steroid receptor coactivator-1) [1, 3]. Coactivator proteins unwind the DNA strand, combine with RNA polymerase II and bind with the TATA sequence (TATA-box binding protein, TBP). These interaction lead to initiation of transcription [1, 3]. In view of the discussed processes, the interactions between GCS-GR homodimer and regulatory DNA sequences within the h-GR/NR3C1 gene promoter seem to play the key role [3, 17–20]. Clinical observations and studies conducted by many investigators allow to put forward a hypothesis concerning a cause-and-result relationship between the presence of SNPs within the h-GR/NR3C1 gene promoter, and the development of bronchial asthma and resistance to GCS [3, 18–20, 33].
The presented study emphasizes the role of Bcl I polymorphism of h-GR/NR3C1 gene promoter in the etiopathogenesis of bronchial asthma. It should be emphasized that the analysis of SNPs confirmed the correlation between the DNA promoter sequences of the investigated gene and the frequency of bronchial asthma. Undoubtedly, too small sized of the studied groups are still a shortcoming of our project. Nevertheless, the observed variations indicate allele G as a factor promoting the development of bronchial asthma. Mutation G/C within the gene promoter is protective in character and correlates with reduced frequency of the disease. The study needs to be confirmed in large populations of asthmatic patients, especially those with treatment-resistant asthma. It is noteworthy that the significantly increasing prevalence of steroid resistance (35–50%) among patients with severe asthma requires not only correlation of SNP frequencies within the regulatory domains of h-GR/NR3C1 gene promoter, but also assessment of gene couplings crucial for the development of asthma and resistance to treatment.
The latest reports pay attention to the role of gene polymorphisms, genetic variations in receptor expressed and extra receptor transcriptional factors in the etiopathogenesis of asthma and steroid resistance phenomenon. Supposedly, disturbances at the level of AP-1 affinity to GR are one of the molecular pathways of cellular resistance to the effect of GCS. Transcriptional factors, and among them AP-1 (activator protein-1) and nuclear factor kappa B (NF-kB) in particular, are the modulators of activity of numerous genes responsible for the development of inflammation, which, binding to GR block GCS-GR binding with DNA sequences of specific response elements (GRE) [34–38].
Conclusions
To date, it has been impossible to define precisely the role of single loci, regions of the particular genes, and individual SNPs of the h-GR/NR3C1 gene in the etiopathogenesis of bronchial asthma and response of the patients to GCS therapy. In view of the applicable paradigms of modern genetics, the key role is attributed to determination of the gene structure and its allelic variants, as well as to assessment of the correlation between the level of expression and biological properties of proteins.
Marker RFLP of the h-GR/NR3C1 gene is an important factor in the development of asthma. In the Authors’ opinion, allele G of Bcl I polymorphism of h-GR/NR3C1 gene promoter demonstrates a marked correlation with the development of bronchial asthma. Its evaluation requires intensive research on hereditary factors linking the particular SNPs with the development of bronchial asthma.
It should be emphasized that no studies concerning the frequency of h-GR/NR3C1 glucocorticoid receptor gene polymorphisms in bronchial asthma patients, including those with severe, treatment-resistant asthma, have been conducted in Poland to date.
The Authors believe that genotyping utilizing the PCR–RFLP techniques will allow in the future to create a bronchial asthma patient profile—phenotype of the Polish patients. The presented study is a preliminary stage for more profound analysis of correlations between the prevalence of the particular allelic variants of the h-GR/NR3C1 gene and the development of bronchial asthma, including severe, treatment-resistant forms of the disease.
References
Ito K, Chung K, Adcock I (2006) Update on glucocorticoid action and resistance. J Allergy Clin Immunol 117:522–543
Masoli M, Fabian D, Holt S (2004) The global burden of asthma: executive summary of the GINA Dissemination Committee report. Allergy 59:469–478
Droszcz W (2007) Astma. Wydawnictwo Lekarskie PZWL, Warszawa
Stahl S (2008) Stahl’s essentials psychopharmacology. Wydawnictwo Cambridge University Press, New York
Holloway J, Beghé B, Holgate S (1999) The genetic basis of atopic asthma. Clin Exp Allergy 29:1023–1032
Wiesch D, Meyers D, Bleecker E (1999) Genetics of asthma. J Allergy Clin Immunol 104:895–901
Strachan D (1989) Hay fever, hygiene, and household size. BMJ 299:1259–1260
Hawkins G, Amelung P, Smith R et al (2004) Identification of polymorphisms in the human glucocorticoid receptor gene (NR3C1) in a multi-racial asthma case and control screening panel. DNA Seq 15:167–173
Murray R, Granner D, Mayes P et al (1998) Biochemia Harpera. Wydawnictwo Lekarskie PZWL, Warszawa
Rivers C, Levy A, Hancock J et al (1999) Insertion of an amino acid in the DNA-binding domain of the glucocorticoid receptor as a result of alternative splicing. J Clin Endocrinol Metab 84:4283–4286
Hollenberg S, Weinberger C, Ong E et al (1986) Primary structure and expression of a functional human glucocorticoid receptor cDNA. Nature 318:635–641
Grzanka A, Rogala B (2000) Molecular mechanism of glucocorticoids and difficult asthma. Allerg Asthma Immunol 5:247–252
Schwartz H, Lowell F, Melby J (1968) Steroid resistance in bronchial asthma. Ann Intern Med 69:493–499
Carmichael J, Paterson I, Diaz P (1981) Corticosteroid resistance in chronic asthma. Br Med J 282:1419–1422
Corrigan C, Brown P, Barnes N et al (1991) Glucocorticoid resistance in chronic asthma. Glucocorticoid pharmacokinetics, glucocorticoid receptor characteristics, and inhibition of peripheral blood T cell proliferation by glucocorticoids in vitro. Am Rev Respir Dis 144:1016–1025
Adcock I, Lane S, Brown C et al (1995) Abnormal glucocorticoid receptor-activator protein 1 interaction in steroid-resistant asthma. J Exp Med 182:1951–1958
Maltese P, Canestrari E, Palma L et al (2009) High resolution melting (HRM) analysis for the detection of ER22/23EK, Bcl I, and N363S polymorphisms of the glucocorticoid receptor gene. J Steroid Biochem Mol Biol 113:269–274
van Rossum E, Koper J, van den Beld A et al (2003) Identification of the Bcl I polymorphism in the glucocorticoid receptor gene: association with sensitivity to glucocorticoids in vivo, and body mass index. Clin Endocrinol 59:585–592
Panarelli M, Holloway C, Fraser R et al (1998) Glucocorticoid receptor polymorphism, skin vasoconstriction, and other metabolic intermediate phenotypes in normal human subjects. J Clin Endocrinol Metab 83:1846–1852
Gergics P, Patocs A, Majnik J et al (2006) Detection of the Bcl I polymorphism of the glucocorticoid receptor gene by single-tube allele-specific polymerase chain reaction. J Steroid Biochem Mol Biol 100:161–166
Fal A, Biegus J, Rosiek M (2003) New aspects of bronchial asthma genetics—ADAM 33 gene. Alergia Astma Immunologia 8:111–116
Cannings C, Edwards A (1968) Natural selection and the de Finetti diagram. Ann Hum Genet 31:421–428
Elston R, Forthofer R (1977) Testing for Hardy–Weinberg equilibrium in small samples. Biometrics 33:536–542
Mendell N, Simon G (1984) A general expression for the variance-covariance matrix of estimates of gene frequency: the effects of departures from Hardy–Weinberg equilibrium. Ann Hum Genet 48:283–286
Sasieni P (1997) From genotypes to genes: doubling the sample size. Biometrics 53:1253–1261
Smith C (1970) A note on testing the Hardy–Weinberg Law. Ann Hum Genet 33:377–383
Weir B (1996) Statitical data analysis II methods for discrete population genetic data. Sinauer Associates, Massachusetts
Goleva E, Eves P (2006) Increased glucocorticoid receptor beta alters steroid response in glucocorticoid insensitive asthma. Am J Respir Crit Care Med 173:607–616
Lewis-Tuffin L, Jewell C, Bienstock R (2007) Human glucocorticoid receptor beta binds RU-486 and is transcriptionally active. Mol Cell Biol 27:2266–2282
Loke T, Mallett K, Ratoff J (2006) Systemic glucocorticoid reduces bronchial mucosal activation of activator protein 1 components in glucocorticoid-sensitive but not glucocorticoid-resistant asthmatic patients. J Allergy Clin Immunol 118:368–375
Ito K, Yamamura S, Essilfie-Quaye S (2006) Histone deacetylase 2-mediated deacetylation of the glucocorticoid receptor enables NF-kappaB suppression. J Exp Med 203:7–13
Abraham S, Lawrence T, Kleiman A (2006) Antiinflammatory effects of dexamethasone are partly dependent on induction of dual specificity phosphatase 1. J Exp Med 203:1883–1889
Webster J, Oakley R, Jewell C et al (2001) Proinflammatory cytokines regulate human glucocorticoids receptor gene expression and lead to the accumulation of the dominant negative beta isoform: mechanism for the generation of glucocorticoids resistance. Proc Natl Acad Sci 98:6865–6870
DeRijk R, Schaaf M, de Kloet E (2002) Glucocorticoid receptor variants: clinical implications. J Steroid Biochem Mol Biol 81:103–122
de Lange P, Koper J, Brinkmann A (1999) Natural variants of the beta-isoform of the human glucocorticoid receptor do not alter sensitivity to glucocorticoids. Mol Cell Endocrinol 153:163–168
de Lange P, Koper J, Huizinga N et al (1997) Differential hormone-dependent transcriptional activation and repression by naturally occurring human glucocorticoid receptor variants. Mol Endocrinol 11:1156–1164
Wang J, Xu Y, Zhao H et al (2009) Genetic variations in chemoattractant receptor expressed on Th2 cells (CRTH2) is associated with asthma susceptibility in Chinese children. Mol Biol Rep 36:1549–1553
Zhang X, Su D, Zhang X et al (2009) Association of ADAM33 gene polymorphisms with adult concomitant allergic rhinitis and asthma in Chinese. Han population. Mol Biol Rep 36:1505–1509
Acknowledgments
The study was partially financed from the Grant No N N402 374638 of The Minister of Science and Higher Education of Polish Republic received by Michał Panek, MD and Prof. Piotr Kuna and N N 402 350838 received by Prof Janusz Szemraj. The study was partially financed from the grant received by Michał Panek, MD within the framework of a project supporting innovative doctoral studies, entitled: “Scholarships supporting innovative doctoral studies” based on funds provided by the EU European Social Fund and Polish state budget allocation for Integrated Operational Plan for Regional Development according to Lodz Region Innovation Strategy—RSI LORIS. Program title: ZPORR. Sector: 2.6 Regional Innovation Strategies and Transfer of Knowledge. Project title: “Scholarships supporting innovative doctoral studies”. Project number: Z/2.10/II/2.6/1/09. The project is financed in 75% from the European Social Fund and in 25% from the state budget.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Pietras, T., Panek, M., Tworek, D. et al. The Bcl I single nucleotide polymorphism of the human glucocorticoid receptor gene h-GR/NR3C1 promoter in patients with bronchial asthma: pilot study. Mol Biol Rep 38, 3953–3958 (2011). https://doi.org/10.1007/s11033-010-0512-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11033-010-0512-5