
Abstract
Background
Worldwide, music is commonly played in the operation room. The effect of music on surgical performance reportedly has varying results, while its effect on mental workload and key surgical stressor domains has only sparingly been investigated. Therefore, the aim is to assess the effect of recorded preferred music versus operating room noise on laparoscopic task performance and mental workload in a simulated setting.
Methods
A four-sequence, four-period, two-treatment, randomized controlled crossover study design was used. Medical students, novices to laparoscopy, were eligible for inclusion. Participants were randomly allocated to one of four sequences, which decided the exposure order to music and operation room noise during the four periods. Laparoscopic task performance was assessed through motion analysis with a laparoscopic box simulator. Each period consisted of ten alternating peg transfer tasks. To account for the learning curve, a preparation phase was employed. Mental workload was assessed using the Surgery Task Load Index. This study was registered with the Netherlands Trial Register (NL7961).
Results
From October 29, 2019 until March 12, 2020, 107 participants completed the study, with 97 included for analyzation. Laparoscopic task performance increased significantly during the preparation phase. No significant beneficial effect of music versus operating room noise was observed on time to task completion, path length, speed, or motion smoothness. Music significantly decreased mental workload, reflected by a lower score of the total weighted Surgery Task Load Index in all but one of the six workload dimensions.
Conclusion
Music significantly reduced mental workload overall and of several previously identified key surgical stressor domains, and its use in the operating room is reportedly viewed favorably. Music did not significantly improve laparoscopic task performance of novice laparoscopists in a simulated setting. Although varying results have been reported previously, it seems that surgical experience and task demand are more determinative.
Similar content being viewed by others


Worldwide, music is commonly played during surgery [1]. Perioperative music has been extensively investigated in adult surgical patients with several beneficial effects [2,3,4]. However, no definitive conclusion on the effect of music on surgical task performance can currently be drawn due to conflicting study results, inconsistent data reporting methods, and varying study designs in previously published studies [5]. To date, all these studies have been conducted in a simulated setting [5], as surgical performance in a simulated setting correlates to performance during actual real-world surgery and influences postoperative patient outcome [6,7,8,9]. It is unclear whether the reported beneficial effects of music on surgical performance are due to an auditory stimulus and not music per se, as all but one [10] of the previous studies used silence as a control [11,12,13,14,15,16,17,18]. Given that high noise level settings are commonly prevalent in the operation room (OR) [19], it could be argued that using silence as a control factor is therefore not appropriate when evaluating the effect of music on surgical performance.
Some surveys have shown that music is well liked by surgical personnel and can improve focus during surgery [1], while others mentioned that it can be distracting and reduce vigilance [20, 21]. Therefore, music during surgery could potentially influence mental workload, which can be defined as the attention that can be directed to a surgical task and the balance of the attention amount used and additionally available when necessary. Increased mental workload is associated with decreased surgical task performance [22]. While perioperative music has a significant beneficial attenuating effect on the physiological stress response in adult surgical patients [3], its effect on mental workload and stress while performing a surgical task has only sparingly been investigated [23].
Laparoscopic surgery requires different skills compared to conventional open surgery due to the use of long instruments and the fulcrum effect, two-dimensional screen visualization which can impair depth perception, and limited tactile feedback [24]. Therefore, simulation using either a box trainer or virtual reality is increasingly used to provide a safe environment for the early learning curve phase. Successfully completing the Fundamentals of Laparoscopic Surgery program is required to become board certified as a general surgeon in the United States [25]. The acquired competencies in a simulated setting seem to be transferable to the real word setting with favorable effects on skill, knowledge, and patient outcome [6, 9, 26]. The purpose of this randomized crossover study is to investigate the effect of participant-selected recorded music versus recorded OR noise on laparoscopic task performance, mental workload, and heart rate variability (HRV) in a simulated setting.
Materials and methods
This study was approved in September 2019 by the Medical Ethics Committee Erasmus MC (MEC-2019-0537) and prospectively registered with the Netherlands Trial Register (Trial NL7961). The study was performed in accordance with the ethical standards of the Helsinki Declaration of 1975. No study protocol amendments were required. Reporting adhered to the 2010 Consolidated Standard of Reporting Trials (CONSORT) extension for randomized crossover trials [27].
Study design
A study procedure timeline overview is presented in Fig. 1. A four-sequence, four-period, two-treatment, randomized controlled crossover study design was used to investigate the effects of recorded, participant-selected music versus recorded OR noise on laparoscopic task performance, mental workload, and HRV. Medical students who were novices to laparoscopy and provided written informed consent were eligible for study participation. Severe hearing impairment, visual impairment, physical handicap that impairs laparoscopic task performance, or use of cardiac medication were considered as exclusion criteria. Participants were instructed to bring music they would like to listen to while performing a laparoscopic task and to abstain from alcohol for 12 h prior to the experiment. The 10 min OR noise recording was selected from a list by three authors (VF, PO and JJ) with prior surgical experience in the OR to represent noise during a routine laparoscopic surgical procedure (i.e., no orthopedic drilling noise). Laparoscopic task performance was assessed with a validated, custom-made laparoscopic box simulator using the peg transfer task [23], during which a blue and red peg are moved with a grasper forceps to a predefined location shown on a monitor. This task is part of the Fundamentals of Laparoscopic Surgery program for surgical residents in the United States [28]. Motion data to assess laparoscopic task performance were captured using a Leap Motion Device (LMC, Leap Motion Inc., LM-010), a compact sensor modified and customized for motion analysis, connected to a computer with monitor, and a webcam (Gemini Gembird) functioning as camera with a frame rate of 60 Hz. Motion data were progressed using a custom-made software program (OCRAM technologies) combined with Python version 2.7.

Study procedure overview timeline. Timeline detailing study procedures. Depending on the sequence, consisting of 4 periods, participants were exposed to either music or operation room noise. Preparation phase = 30 alternating peg transfer tasks. Period = 10 alternating peg transfer tasks, M Exposure to recorded, participant-selected music, C Exposure to recorded operation room noise, SURG-TLX surgery task load index, HRV heart rate variability, measured continuously throughout the experiment
After signing the informed consent form, a chest band was fitted to continuously measure HRV throughout the entire experimental session [29]. A custom demographic questionnaire evaluating music importance and preferences, listening to music while studying, and whether a music instrument is or was played, was filled out. Participants were randomly allocated using the sealed envelope method and a 1:1:1:1 allocation ratio to one of four sequences. Each sequence consisted of a preparation phase followed by two periods of recorded, participant-selected music and two periods recorded OR noise, with the order of exposure decided by the previously mentioned randomization. To account for the learning curve, all participants completed a preparation phase consisting of 30 peg transfer tasks, alternating between the right and left hand (i.e., the first peg transfer was performed using the right hand, the second using the left hand, the third using the right hand again and so on), as it was previously observed that the learning curve flattened after 20 repetitions [23]. During each period, 10 alternating peg transfer tasks were performed while listening to either music or OR noise using noise-canceling headphones (Bose Quietcomfort 35ii). Volume level was adjusted at the start by the participant and was therefore consistent during the entire experiment. The Surgery Task Load Index (SURG-TLX) questionnaire evaluating mental workload was filled out after the preparation phase and each period for a total of five times, which led to a washout period of at least several minutes.
Outcome parameters
The primary outcome measure was time to task completion, defined as the time in seconds (s) required to complete a 10 peg transfer task period, consisting of alternating peg transfers with the dominant and non-dominant hand. Time to task completion of the peg transfer task is the main score attribute in the Fundamentals of Laparoscopic Surgery program [28]. Furthermore, path length, the total distance traveled in millimeters (mm) by the instrument tip, speed, the ratio of path length and time to task completion (mm/s), and motion smoothness, the normalized jerk or the rate of instrument tip acceleration change (mm/s3), were measured. To assess the benefit of the preparation phase, motion analysis of the first 10 peg transfers in this phase was compared to the last 10 peg transfers additionally.
Mental workload was assessed using the SURG-TLX, an in laparoscopic surgery validated, adapted version of the National Aeronautics and Space Administration Task Load Index (NASA-TLX) questionnaire [30]. This weighted questionnaire assesses six dimensions of workload (mental demands, physical demands, temporal demands, task complexity, situation stress and distractions) using a visual analog scale (VAS) and was filled out by all participants after the preparation phase and each period.
Heart rate and HRV, defined as the variation in time between each heartbeat (NN), were continuously measured from the preparation phase start until experiment end using the commercially available, validated BM-CS5EU wireless chest band (BM innovations, Acentas GmbH) [29]. Short-term HRV measurements [31], lasting approximately five minute during each of the four periods as well as the first five and last five minutes of the preparation phase, were analyzed (ATS 2.4.6., BM Innovations). HRV can represent the physiological state of autonomic nervous system activity and has been used to assess mental strain in surgeons during laparoscopic task performance [32]. A lower HRV implicates dominance by the sympathetic nervous system and has been regarded as higher mental strain. HRV quantification was presented using the time-domain variable standard deviation of all NN intervals (SDNN) in milliseconds (ms).
Blinding and data analysis
Obviously, the participants in this experiment could not be blinded. Headphones were employed partly to blind the research assistant overseeing the experiment. However, as participants brought their preferred music using different devices, transferring music to the laptop which contained the OR noise recording in order to be played during the experiment was impractical. Therefore, the music intervention was directly played while the headphones were attached to the participant’s phone or music player. Although the research assistant was separated from the participant by an opaque screen during the experiment in order to reduce any influence to the fullest extent, the assistant was not considered to be blinded. All questionnaires were filled out using a secure, computerized questionnaire by the participants themselves and were therefore not administered by the research assistant. Heart rate and HRV data were processed through a validated software program. Motion data analysis was computerized using a software script validated in previous studies [23], while the person responsible for data retrieval and preparing it for analysis was blinded to the allocation sequence. All data were only analyzed after the last participant had completed the experiment.
Data were statistically analyzed using the IBM Statistical Package for the Social Sciences (SPSS) version 24.0. Data were presented as mean and standard deviation (SD) if data were normally distributed, and median and interquartile range (IQR) if not. Normality of data was assessed using the Kolmogorov–Smirnov test and visually in Q–Q plots. Continuous variables were compared using a paired-samples T test or Wilcoxon signed rank test, as appropriate. Within subject differences were presented by subtracting the control group from the intervention group. Categorical variables were presented as absolute number and percentage. Two tailed testing was used with statistical significance inferred at p < 0.05.
Sample size calculation
Based on our previous study using the same laparoscopic box simulator [23], an effect size of 0.3 was deemed clinically relevant. With alpha set at 0.05, power of 0.80 and two-sided dependent testing, 90 participants would be required. Given that there were four randomization sequences, we chose to set the sample size at 92 participants to allow for equal distribution among the sequences. Taking into account a 10 percentage exclusion rate, total sample size was set at 104 participants.
Results
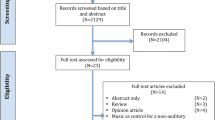
From October 29, 2019 until March 12, 2020, 107 participants were recruited. Ten participants were excluded because of equipment failure at the start of the study. Motion analysis and mental workload assessment using the SURG-TLX was performed of all 97 participants who completed the study. Due to missing data, heart rate and HRV analysis was performed of 93 participants (Fig. 2).

CONSORT flow diagram. Inclusion flowchart. N number of participants, SURG-TLX surgery task load index, HR heart rate, HRV heart rate variability
Demographic characteristics
An overview of demographic characteristics of the full cohort (n = 97) can be found in Table 1. Median age was 20 (IQR 18 to 21), with the majority of the medical students being in their first three years of study (77%), right-handed (85%), and female (57%). A little over half of participants (54%) had experience with a musical instrument, with 31 (32%) currently playing and 21 (22%) previously playing an instrument. Music was deemed important in daily life with a median numeric rating scale (NRS) of 8 (IQR 7 to 8), with 68 (70%) participants listening to music while studying. Favorite genres while studying were classical (20%) and pop (16%), while 18% specified music that could not be classified under commonly described genres. Top music genres chosen for this experiment were pop (47%), classical (21%), and hip hop (9.3%) (Online Appendix A).
Laparoscopic task performance
Laparoscopic task performance improved during the preparation phase (Table 2), with time to task completion of the last 10 alternating peg transfer tasks being significantly faster compared to the first 10 tasks (median 250 s [IQR 218 to 327] versus 433 s [335 to 532], p < 0.001). A significant reduction in path length of the last 10 compared to the first 10 tasks during the preparation phase (8375 mm [6107 to 12397] versus 12810 mm [8813 to 18168], p < 0.001) and improved motion smoothness in the form of normalized jerk was also observed (236596 mm/s3 [102441 to 471534] versus 857493 mm/s3 [407460 to 1833467], p < 0.001).
No statistically significant difference in laparoscopic task performance parameters were observed during exposure to the different auditory stimuli (Table 3). Time to task completion was not statistically significantly faster while listening to music compared to OR noise (210 s [191 to 262] versus 221 s [188 to 257], p = 0.518) and path length was not reduced (7606 mm [5725 to 9182] versus 7462 mm [5833 to 8952], p = 0.434). Speed did not differ (434 mm/s [321 to 552] versus 436 mm/s [324 to 556], p = 0.758), nor did motion smoothness in the form of normalized jerk (180687 mm/s3 [83581 to 281566] versus 171957 mm/s3 [95905 to 316327], p = 0.125). Additionally, there was no significant difference by music compared to OR noise in laparoscopic task performance parameters of the dominant and non-dominant hand, when these were assessed separately from each other. When assessing the participants who preferred to listen to music when studying (n = 68) as a separate group, no significant difference was observed. No difference was observed when taking experience with playing a musical instrument into account, or gender (Table 4).
Mental workload, heart rate, and HRV
A significant beneficial effect of music was observed on mental workload as the weighted SURG-TLX score was lower (27.0 [17.3 to 38.3] versus 33.7 [21.2 to 43.3], p < 0.001). This was also reflected in all but one of the SURG-TLX dimensions (Table 3, Online Appendix B). Mental demands (25.0 [15.0 to 37.5] versus 30.0 [20.0 to 50.0], p < 0.001), physical demands (20.0 [12.5 to 32.5] versus 22.5 [12.5 to 31.3], p = 0.012), temporal demands (35.0 [20.0 to 47.5] versus 37.5 [22.5 to 50], p = 0.010), situational stress (17.5 [10.0 to 30.0] versus 25.0 [12.5 to 40.0], p < 0.001), and distractions (15.0 [10.0 to 30.0] versus 32.5 [20.0 to 47.5], p < 0.001) were all significantly lower when exposed to music. Only in the task complexity dimension, no significant difference was observed (25.0 [12.5 to 42.5] versus 25.0 [15.0 to 43.8], p = 0.471).
In four participants (4.1%), heart rate and HRV data were not registered, and data were therefore analyzed of 93 participants. None of the included participants had known cardiac diseases or arrhythmias or used any cardiac medication. Median duration of HRV measurement was 4.25 min [3.59 to 5.11] over the experiment (93 measurements per period) as a whole. Of the 372 total heart rate and HRV measurements, the measurement duration of 173 (47%) were at least 4.5 min or more, 166 (45%) were between 3.5 and 4.5 min, and 33 were below 3.5 min (8.9%). Heart rate during the last 5 min of the preparation phase was statistically significantly increased compared to the first 5 min (91 [80 to 106] versus 87 [75 to 101], p < 0.001), while HRV was statistically significantly lower (48 [38 to 63] versus 52 [40 to 71], p < 0.001) (Table 2). During the experiment, heart rate was statistically significantly higher while exposed to music (88 [78 to 102] versus 87 [77 to 102], p = 0.046). HRV was statistically significantly lower while exposed to music (49 [40 to 63] versus 52 [41 to 68], p = 0.015) (Table 3).
No correlation was present between HRV and mental workload assessed using the SURG-TLX (Spearman’s rho 0.060, p = 0.565), nor between heart rate and SURG-TLX (Spearman’s rho -0.022, p = 0.836).
Discussion
This randomized controlled crossover study with the largest sample size to date assessed the effect of participant-selected recorded music on laparoscopic task performance and mental workload in a simulated setting. No statistically significant beneficial effect of participant-selected music was observed regarding laparoscopic task performance while compared to OR noise in novice laparoscopists. Previous studies, all performed in a simulated setting, reported varying results [5]. Two studies with a similar study design and comparable tasks by the same lead author evaluated the effect of music on laparoscopic task performance. A beneficial effect on task accuracy in expert surgeons was observed [11], but not in junior residents with no previous laparoscopic experience [12]. No beneficial effects were observed in junior novice surgeons asked to perform part of a laparoscopic cholecystectomy [15], nor in 12 surgeons with varying experience placing laparoscopic knots [10]. Although considered a basic skill, laparoscopic knot tying is reportedly the most difficult laparoscopic skill to master [33, 34]. In aforementioned studies, preselected music by the research team was used. A positive trend between likability of the music and a beneficial effect was noted [15]. In practice, it seems less likely that surgeons would listen to music that they do not prefer. Surgeons did choose the music played in the OR in a majority of cases [35,36,37]. Hence, participant-selected preferred music was used which we believe to be more clinically relevant. Recently, we observed a significant beneficial effect on time to task completion (4.68%, p = 0.037) and path length (6.35%, p = 0.019) of participant-selected music versus silence in 60 medical students in our previous study. Surgical experience level was comparable, as they were also novices of laparoscopy, and a similar study setup was employed, although the modified peg transfer task was only performed 5 times with solely the dominant hand [23]. It could be argued that the different results compared to this study on task performance can partly be attributed due to a more demanding task, with a higher SURG-TLX and heart rate in this study [23]. Therefore, given the previously mentioned studies, it might be possible that depending on experience and task complexity, music could be beneficial when the surgical task is considered to be relatively easy and manageable, but that this effect disappears when the motor task is more difficult and increasingly demanding on mental workload.
An important component during laparoscopic surgery besides motor task execution and performance is the cognitive decision making to determine which motor steps should be executed. Reducing mental workload, often reported as stress by the surgeon, will leave more mental resource capacity for both components [38]. Indeed, laparoscopic task performance has been correlated to stress experienced by the surgeon [39], with identified key stressors in the form of time pressure, noise and distractions impairing dexterity, and increasing error rate [40]. Mental workload assessed using the SURG-TLX questionnaire was significantly reduced by music, which was especially profound in the domains mental demands (within subject difference -5.0, p = 0.000) and distractions (within subject difference -10.0, p = 0.000), while reflected to a slightly lower but still significant degree in temporal demands (within subject difference -2.5, p = 0.010). While secondary outcome measure results should always be interpreted with caution, these findings mimic our previous study which also observed a beneficial effect by music on mental workload during laparoscopic task performance [23]. Previous surveys also observed favorable responses in general towards the use of music by surgeons, especially in regard to stress [36, 41, 42]. Although reporting bias cannot be entirely ruled out, the SURG-TLX follows the trend of objective parameters like salivary cortisol levels [43]. HRV seems to be an adequate method to assess mental surgical stress as well [44]. While heart rate was statistically significantly higher (within subject difference 1.0 bpm, p = 0.046) and HRV lower (within subject difference − 2.5, p = 0.015) in the music group, the absolute difference observed cannot be considered clinically relevant. It was expected that each period in this experiment would allow for short-term HRV analysis (nominal 5 min duration), but 54% of HRV measurements lasted 4.5 min or less. Given that the validity of ultra short-term HRV analysis has been questioned [31], as well as the lack of correlation with mental workload in this study, interpretation of these results as a reflection of mental strain in our study should be done with caution.
Major strong points of this study was the largest sample size to date and the rigorous study design, which reduces a potential carryover effect [45]. While computerized randomization would preferably be used, we considered non-random allocation risk to be minimal. All participants acted as their own control. The research assistant overseeing the experiment execution had no incentive to influence allocation as they had no information on the participant during the experiment, given that all questionnaires were filled out using secure computerized questionnaire. These data were only revealed and analyzed after all inclusions had been completed. The envelope deciding allocation sequence was chosen before the preparation phase, preventing any potential influence of this phase on the allocation sequence. A maximum envelope number per sequence based on the sample size calculation assured equal allocation. A previously validated, custom-made laparoscopic box trainer was used [23], with real surgical instruments and pegs allowing for realistic tactile sense and haptic feedback that is not provided by all virtual reality simulators. To get acquainted with the box trainer and eliminate the learning curve as the foremost potential biasing factor, a preparation phase was incorporated. The number of peg transfer tasks necessary for this was based on a previously conducted study with the same box trainer [23]. Its success is evident through the fact that time to task completion rapidly decreased in the preparation phase, while it stayed almost consistent during the experiment (for either treatment factor). Since previous studies did not employ a preparation phase, it is difficult to ascertain whether the previously reported effects partly reflect the learning curve. Moreover, participant-selected instead of researcher-selected recorded music was used and the volume adjusted by the participants themselves to more accurately represent the real-world setting, while recorded OR noise acted as a control instead of silence in order to account for auditory stimulation as a factor. Nonetheless, several limitations can still be observed. The peg transfer task was chosen, which does not require surgical knowledge that could potentially influence task performance. However, this task with an average observed duration of approximately 3.5 min per period takes significantly shorter than any surgical procedure. Still, earlier studies reported that even relatively simple, short-lasting tasks and drills like these can improve relevant laparoscopic surgical tasks and should therefore not be disregarded [46, 47]. We chose to perform the study in medical students who were inexperienced with laparoscopy in order to reduce potential previous experience influencing laparoscopic task performance. Studies evaluating noise in the OR found higher subjective distraction levels in assisting surgeons with less experience compared to the main, more experienced surgeons [48], while the negative impact on clinical reasoning was lower when anesthesiological residents were more experienced [49]. It has been theorized that more experienced surgeons can block out noise and music more effectively [10], theoretically decreasing potential effect size and increasing the required number of participants. It would have been impractical therefore to try to investigate the effects of music using more experienced residents or surgeons in such large numbers without the present data and our recently published study [23]. Finally, a major factor affecting teamwork in the OR is communication, with a considerable percentage of surgical errors involving communication between surgical personnel [50]. This factor could not be evaluated. These limitations make extrapolation of the observed results to the real-world setting less appropriate, limiting conclusions to a simulated setting.
Although varying results regarding the effects of music on laparoscopic task performance have been reported, it seems that surgical experience and task demand can be more determinative. Future studies should take these factors into account and evaluate surgeons with different experience levels in a more lifelike setting. While several studies evaluated the effect of music on laparoscopic task performance through short-lasting laparoscopic and surgical tasks to date [5], important elements like simulated surgical procedures, communication, and performance of the entire OR team have only sparingly been investigated [51, 52]. Auditory intervention should preferably consist of music combined with OR noise versus OR noise through speakers, with music chosen by both the surgeon and OR team. Music did significantly reduce mental workload and several previously identified key stressors of surgery, and its use in the operating theater is reportedly viewed favorably. Higher perceived stress is associated with a decreased HRV even throughout the night, indicative of a protracted recovery time [44]. As music can attenuate the stress response to surgery in patients undergoing surgery, future research should incorporate its effect on mental workload through HRV with attention to recovery from surgical task performance as well.
Conclusion
In this four-sequence, four-period, two-treatment, randomized controlled crossover study of 97 laparoscopy novices, recorded preferred music significantly reduced mental workload overall and in key surgical stressor domains during laparoscopic task performance in a simulated setting when compared to OR noise, but no beneficial effect on task performance itself was observed.
Abbreviations
- bpm:
-
Beats per minutes
- CONSORT:
-
Consolidated standard of reporting trials
- ECG:
-
Electrocardiography
- HRV:
-
Heart rate variability
- IQR:
-
Interquartile range
- mm:
-
Millimeter
- ms:
-
Millisecond
- NASA-TLX:
-
National aeronautics and space administration task load index
- NN:
-
Interval between two heartbeats
- NRS:
-
Numeric rating scale
- OR:
-
Operating room
- RCT:
-
Randomized controlled trial
- s:
-
Second
- SD:
-
Standard deviation
- SDNN:
-
Standard deviation of all NN intervals, representing HRV median variability
- SPSS:
-
Statistical package for the social sciences
- SURG-TLX:
-
Surgery task load index
- VAS:
-
Visual analog scale
References
Yamasaki A, Mise Y, Lee JE, Aloia TA, Katz MH, Chang GJ, Lillemoe KD, Raut CP, Conrad C (2016) Musical preference correlates closely to professional roles and specialties in operating room: a multicenter cross-sectional cohort study with 672 participants. Surgery 159:1260–1268
Fu VX, Oomens P, Klimek M, Verhofstad MHJ, Jeekel J (2019) The effect of perioperative music on medication requirement and hospital length of stay: a meta-analysis. Ann Surg
Fu VX, Oomens P, Sneiders D, van den Berg SAA, Feelders RA, Wijnhoven BPL, Jeekel J (2019) The effect of perioperative music on the stress response to surgery: a meta-analysis. J Surg Res 244:444–455
Kuhlmann AYR, de Rooij A, Kroese LF, van Dijk M, Hunink MGM, Jeekel J (2018) Meta-analysis evaluating music interventions for anxiety and pain in surgery. Br J Surg 105:773
Oomens P, Fu VX, Kleinrensink GJ, Jeekel J (2019) The effect of music on simulated surgical performance: a systematic review. Surg Endosc 33:2774–2784
Sturm LP, Windsor JA, Cosman PH, Cregan P, Hewett PJ, Maddern GJ (2008) A systematic review of skills transfer after surgical simulation training. Ann Surg 248:166–179
Thomsen AS, Smith P, Subhi Y, Cour M, Tang L, Saleh GM, Konge L (2017) High correlation between performance on a virtual-reality simulator and real-life cataract surgery. Acta Ophthalmol 95:307–311
Agha RA, Fowler AJ (2015) The role and validity of surgical simulation. Int Surg 100:350–357
Zendejas B, Cook DA, Bingener J, Huebner M, Dunn WF, Sarr MG, Farley DR (2011) Simulation-based mastery learning improves patient outcomes in laparoscopic inguinal hernia repair: a randomized controlled trial. Ann Surg 254:502–511
Moorthy K, Munz Y, Undre S, Darzi A (2004) Objective evaluation of the effect of noise on the performance of a complex laparoscopic task. Surgery 136:25–31
Conrad C, Konuk Y, Werner P, Cao CG, Warshaw A, Rattner D, Jones DB, Gee D (2010) The effect of defined auditory conditions versus mental loading on the laparoscopic motor skill performance of experts. Surg Endosc 24:1347–1352
Conrad C, Konuk Y, Werner PD, Cao CG, Warshaw AL, Rattner DW, Stangenberg L, Ott HC, Jones DB, Miller DL, Gee DW (2012) A quality improvement study on avoidable stressors and countermeasures affecting surgical motor performance and learning. Ann Surg 255:1190–1194
Kyrillos R, Caissie M (2017) Effect of music on surgical skill during simulated intraocular surgery. Can J Ophthalmol 52:538–542
Lies SR, Zhang AY (2015) Prospective randomized study of the effect of music on the efficiency of surgical closures. Aesthet Surg J 35:858–863
Miskovic D, Rosenthal R, Zingg U, Oertli D, Metzger U, Jancke L (2008) Randomized controlled trial investigating the effect of music on the virtual reality laparoscopic learning performance of novice surgeons. Surg Endosc 22:2416–2420
Shakir A, Chattopadhyay A, Paek LS, McGoldrick RB, Chetta MD, Hui K, Lee GK (2017) The effects of music on microsurgical technique and performance: a motion analysis study. Ann Plast Surg 78:S243–S247
Siu KC, Suh IH, Mukherjee M, Oleynikov D, Stergiou N (2010) The effect of music on robot-assisted laparoscopic surgical performance. Surg Innov 17:306–311
Wiseman MC (2013) The Mozart effect on task performance in a laparoscopic surgical simulator. Surg Innov 20:444–453
Katz JD (2014) Noise in the operating room. Anesthesiology 121:894–898
Hawksworth C, Asbury AJ, Millar K (1997) Music in theatre: not so harmonious. A survey of attitudes to music played in the operating theatre. Anaesthesia 52:79–83
Weldon SM, Korkiakangas T, Bezemer J, Kneebone R (2015) Music and communication in the operating theatre. J Adv Nurs 71:2763–2774
Yurko YY, Scerbo MW, Prabhu AS, Acker CE, Stefanidis D (2010) Higher mental workload is associated with poorer laparoscopic performance as measured by the NASA-TLX tool. Simul Healthc 5:267–271
Oomens P, Fu VX, Kleinrensink VEE, Kleinrensink GJ, Jeekel J (2020) The effects of preferred music on laparoscopic surgical performance: a randomized crossover study. World J Surg. https://doi.org/10.1007/s00268-020-05523-0
Gallagher AG, McClure N, McGuigan J, Ritchie K, Sheehy NP (1998) An ergonomic analysis of the fulcrum effect in the acquisition of endoscopic skills. Endoscopy 30:617–620
The American Board of Surgery. ABS to require ACLS, ATLS and FLS for general surgery certification. August 15, 2008. https://www.absurgery.org/default.jsp?news_newreqs. Accessed 26 March 2020
Zendejas B, Brydges R, Hamstra SJ, Cook DA (2013) State of the evidence on simulation-based training for laparoscopic surgery: a systematic review. Ann Surg 257:586–593
Dwan K, Li T, Altman DG, Elbourne D (2019) CONSORT 2010 statement: extension to randomised crossover trials. BMJ 366:l4378
Fundamentals of Laparoscopic Surgery (FLS). www.flsprogram.org. Accessed 23 March 2020.
Schonfelder M, Hinterseher G, Peter P, Spitzenpfeil P (2011) Scientific comparison of different online heart rate monitoring systems. Int J Telemed Appl 2011:631848
Wilson MR, Poolton JM, Malhotra N, Ngo K, Bright E, Masters RS (2011) Development and validation of a surgical workload measure: the surgery task load index (SURG-TLX). World J Surg 35:1961–1969
Pecchia L, Castaldo R, Montesinos L, Melillo P (2018) Are ultra-short heart rate variability features good surrogates of short-term ones? State-of-the-art review and recommendations. Healthc Technol Lett 5:94–100
Grantcharov PD, Boillat T, Elkabany S, Wac K, Rivas H (2019) Acute mental stress and surgical performance. BJS Open 3:119–125
Lim S, Ghosh S, Niklewski P, Roy S (2017) Laparoscopic suturing as a barrier to broader adoption of laparoscopic surgery. JSLS 21:1–7
Dehabadi M, Fernando B, Berlingieri P (2014) The use of simulation in the acquisition of laparoscopic suturing skills. Int J Surg 12:258–268
Ahmad M (2017) Role of music in operating room. J Anesth Crit Care Open Access 7(5):00279
Narayanan A, Gray AR (2018) First, do no harmony: an examination of attitudes to music played in operating theatres. New Zealand Med J 131:68–74
Ullmann Y, Fodor L, Schwarzberg I, Carmi N, Ullmann A, Ramon Y (2008) The sounds of music in the operating room. Injury 39:592–597
Carswell CM, Clarke D, Seales WB (2005) Assessing mental workload during laparoscopic surgery. Surg Innov 12:80–90
Arora S, Sevdalis N, Nestel D, Woloshynowych M, Darzi A, Kneebone R (2010) The impact of stress on surgical performance: a systematic review of the literature. Surgery 147:318–330
Moorthy K, Munz Y, Dosis A, Bann S, Darzi A (2003) The effect of stress-inducing conditions on the performance of a laparoscopic task. Surg Endosc 17:1481–1484
Makama JG, Ameh EA, Eguma SA (2010) Music in the operating theatre: opinions of staff and patients of a Nigerian teaching hospital. Afr Health Sci 10:386–389
George S, Ahmed S, Mammen KJ, John GM (2011) Influence of music on operation theatre staff. J Anaesthesiol Clin Pharmacol 27:354–357
Abdelrahman AM, Bingener J, Yu D, Lowndes BR, Mohamed A, McConico AL, Hallbeck MS (2016) Impact of single-incision laparoscopic cholecystectomy (SILC) versus conventional laparoscopic cholecystectomy (CLC) procedures on surgeon stress and workload: a randomized controlled trial. Surg Endosc 30:1205–1211
The AF, Reijmerink I, van der Laan M, Cnossen F (2020) Heart rate variability as a measure of mental stress in surgery: a systematic review. Int Arch Occup Environ Health
Hedayat AS, Stufken J (2003) Optimal and efficient crossover designs under different assumptions about the carryover effects. J Biopharm Stat 13:519–528
Rosser JC, Rosser LE, Savalgi RS (1997) Skill acquisition and assessment for laparoscopic surgery. Arch Surg 132:200–204
Kothari SN, Kaplan BJ, DeMaria EJ, Broderick TJ, Merrell RC (2002) Training in laparoscopic suturing skills using a new computer-based virtual reality simulator (MIST-VR) provides results comparable to those with an established pelvic trainer system. J Laparoendosc Adv Surg Tech A 12:167–173
Keller S, Tschan F, Semmer NK, Holzer E, Candinas D, Brink M, Beldi G (2018) Noise in the operating room distracts members of the surgical team. An Observational Study. World J Surg 42:3880–3887
Enser M, Moriceau J, Abily J, Damm C, Occhiali E, Besnier E, Clavier T, Lefevre-Scelles A, Dureuil B, Compère V (2017) Background noise lowers the performance of anaesthesiology residents' clinical reasoning when measured by script concordance. Eur J Anaesthesiol 34:464–470
Gawande AA, Zinner MJ, Studdert DM, Brennan TA (2003) Analysis of errors reported by surgeons at three teaching hospitals. Surgery 133:614–621
Cheriyan S, Mowery H, Ruckle D, Keheila M, Myklak K, Alysouf M, Atiga C, Khuri J, Khater N, Faaborg D, Ruckle HC, Baldwin DD, Baldwin DD (2016) The impact of operating room noise upon communication during percutaneous nephrostolithotomy. J Endourol 30:1062–1066
Way TJ, Long A, Weihing J, Ritchie R, Jones R, Bush M, Shinn JB (2013) Effect of noise on auditory processing in the operating room. J Am Coll Surg 216:933–938
Acknowledgements
The authors would like to thank Biocheck for providing the equipment and software to assess heart rate and HRV.
Funding
No external funding was received for this study. Equipment and software to analyze heart rate variability was kindly provided by BioCheck, which had no role in study design, data analysis, data interpretation, or manuscript drafting.
Author information
Authors and Affiliations
Contributions
VF, PO, and VK made substantial contributions to conception and design of the study. KS, WB, and PW carried out the experiment for the acquisition of data. VF, PO, and KS made substantial contributions to overall data analysis. VK processed the motion data for analyzation. WB focused primarily on motion analysis and PW on mental workload and heart rate variability analysis. VF, PO, JL, GK, and JJ interpreted the data. VF primarily drafted the manuscript, with substantial contribution by PO, VK, KS, WB, and PW, while JL, GK, and JJ critically revised it for important intellectual content. All authors gave final approval of the version to be published.
Corresponding author
Ethics declarations
Disclosures
V.X. Fu, MD, P. Oomens, MD, V.E.E. Kleinrensink, MSc, K.J. Sleurink, MSc, W.M. Borst, BSc, P.E. Wessels, BSc, Prof. J.F. Lange, MD, PhD, Prof. G.J. Kleinrensink, PhD, and Prof. J. Jeekel, MD, PhD have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
464_2020_7987_MOESM1_ESM.tif
Supplementary file1 Appendix A. Music genres Figure summarizing the music genre chosen for the experiment by the 97 participants (left bar), as well as the preferred genre while studying by 68 participants who like to listen to music while studying (right bar). Data presented are absolute numbers. (TIF 603 kb)
464_2020_7987_MOESM2_ESM.tif
Supplementary file2 Appendix B. Mental workload Effect of participant-selected music and operation room noise on mental workload (Surgery Task Load Index (Surg-TLX)) during laparoscopic task performance. Data is presented as median and interquartile range. Of the three paired bars of the total weighted SURG-TLX and its workload dimensions, the left bar reflects absolute score during participant-selected music exposure, the middle bar during operation room noise exposure, and the right bar the within subject difference. All were statistically significant in favor of music (p<0.05, marked with *), except the dimension task complexity. (TIF 238 kb)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Fu, V.X., Oomens, P., Kleinrensink, V.E.E. et al. The effect of preferred music on mental workload and laparoscopic surgical performance in a simulated setting (OPTIMISE): a randomized controlled crossover study. Surg Endosc 35, 5051–5061 (2021). https://doi.org/10.1007/s00464-020-07987-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-020-07987-6