
Abstract
Observation until the development of symptoms, or ‘watch and wait’, has long been a proposed management technique for patients with indolent lymphomas. However, investigators have found that there may be differences in outcomes for various patient groups according to histopathology, clinical features of the disease, biologic factors as yet to be fully recognized, and type of initial therapy offered. Recently, investigators from the UK National Cancer Research Institute reported that progression-free results were significantly improved when asymptomatic patients with indolent follicular lymphomas received initial therapy with single-agent rituximab rather than when they underwent observation alone. These results were further improved when they received maintenance rituximab. Time to chemotherapy was also longer when these patients received initial therapy with rituximab, thereby delaying the need for such treatment. However, overall survival rates for patients who received rituximab as initial therapy were similar to those for patients who underwent initial ‘watch and wait’. Future studies should concentrate on risks of such management, including cost effectiveness of such treatments and development of resistance to subsequent therapies.




Similar content being viewed by others

References
Portlock C, Rosenberg S. No initial therapy for stage III and IV non-Hodgkin’s lymphomas of favorable histologic types. Ann Intern Med 1979; 90: 10–3
Horning S, Rosenberg S. The natural history of initially untreated low-grade non-Hodgkin’s lymphomas. N Engl J Med 1984; 311: 1471–5
Anderson T, DeVita V, Simon R, et al. Malignant lymphoma. II. Prognostic factors and response to treatment of 473 patients at the National Cancer Institute. Cancer 1982; 50: 2708–21
Anderson T, Bender R, Fisher R, et al. Combination chemotherapy in non-Hodgkin’s lymphoma: results of long-term follow-up. Cancer Treat Rep 1977; 61: 1057–66
Rosenberg S. Non-Hodgkin’s lymphoma: selection of treatment on the basis of histologic type. N Engl J Med 1979; 30: 924–8
Glatstein E, Donaldson S, Rosenberg S, et al. Combined modality therapy in malignant lymphomas. Cancer Treat Rep 1977; 61: 1199–207
Soubeyran P, Egbahli H, Trojani F, et al. Is there any place for a wait-and-see policy in stage I0 follicular lymphoma? Astudy of 43 consecutive patientsina single center. Ann Oncol 1996; 7: 713–8
Advani R, Rosenberg S, Horning S. Stage I and II follicular non-Hodgkin’ lymphoma: long-term follow-up of no initial therapy. J Clin Oncol 2004; 22: 1454–9
Gospadarowicz M, Bush R, Brown T, et al. Prognostic factors in nodular lymphomas: a multivariate analysis based on the Princess Margaret Hospital experience. Int J Radiat Oncol Biol Phys 1984; 10: 489–97
Pendlebury S, Awadi M, Askley S, et al. Radiotherapy results in early stage low grade nodal non-Hodgkin’s lymphoma. Radiother Oncol 1985; 36: 167–71
Vaughan Hudson B, Vaughan Hudson G, MacLennan K, et al. Clinical stage I non-Hodgkin’s lymphoma: Long-term follow-up of patients treated by the British National Lymphoma Investigation with radiotherapy alone as initial therapy. Br J Cancer 1994; 69: 1088–93
Denham J, Denham E, Dear K, et al. The follicular non-Hodgkin’s lymphomas — I: the possibility of cure. Eur J Cancer 1996; 32A: 470–9
MacManus M, Hoppe R. Is radiotherapy curative for stage I and IIlow-grade follicular lymphoma? Results of a long-term follow-up study of patients treated at Stanford University. J Clin Oncol 1996; 14: 1282–90
Wilder R, Jones D, Tucker S, et al. Long-term results with radiotherapy for stage I–II follicular lymphomas. Int J Radiat Oncol Biol Phys 2001; 51: 1219–27
Guadagnolo B, Li S, Neuberg D, et al. Long-term outcome and mortality trends in early-stage, grade 1–2 follicular lymphoma treated with radiation therapy. Int J Radiat Oncol Biol Phys 2006; 64: 928–34
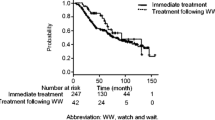
Ardeshna K, Smith P, Norton A, et al. Long-term effect of a watch and wait policy versus immediate systemic treatment for advanced-stage non-Hodgkin lymphoma: a randomized controlled trial. Lancet 2003; 362: 516–22
Brice P, Bastion Y, Lepage E, et al. Comparison in low-tumor-burden follicular lymphomas between an initial no-treatment policy, prednimustine, or interferon alfa: a randomized study from the Groupe d’Etude des Lymphomes Folliculaires. J Clin Oncol 1997; 15: 1110–7
Coiffier B, Bastion Y, Berger F, et al. Prognostic factors in follicular lymphoma. Semin Oncol 1993; 86: 1460–3
Young R, Longo D, Glatstein E, et al. The treatment of indolent lymphomas: watchful waiting v aggressive combined modality. Semin Hematol 1988; 25 Suppl. 2: 11–6
Ardeshna K, Smith P, Qian W, et al. An intergroup randomized trial of rituximab versus a watch and wait strategy in patients with stage II, III, IV, asymptomatic, non-bulky follicular lymphoma (grades 1, 2, and 3a): a preliminary analysis [abstract no.6]. Blood 2010; 116: 5
Ardeshna K, Qian W, Stephens R, et al. Preliminary results of quality of life (QoL) analyses from the intergroup phase III randomised trial of rituximab vs a watch and wait approach in patients with advanced stage, asymptomatic, non-bulky follicular lymphoma [abstract no. 019]. Ann Oncol 2011; 22 Suppl. 4: iv88
Hainsworth J, Litchy S, Shaffer D, et al. Maximizing therapeutic benefit of rituximab: maintenance therapy versus re-treatment at progression in patients with indolent non Hodgkin’s lymphoma — a randomized phase II trial of the Minnie Pearl Cancer Research Network. J Clin Oncol 2005; 23: 1088–95
Martinelli G, Schmitz S, Utiger U, et al. Long-term follow-up of patients with follicular lymphoma receiving single-agent rituximab at two different schedules in trial SAKK 35/98. J Clin Oncol 2010; 28: 4480–4
Gordon L, Grow W, Pusateri A, et al. Phase II trial of individualized rituximab dosing for patients with CD20-positive lymphoproliferative disorders. J Clin Oncol 2005; 23: 1096–102
Kahl B, Hong F, Williams M, et al. Results of Eastern Cooperative Oncology Group protocol E4402 (RESORT): a randomized phase III study comparing two different rituximab dosing strategies for low tumor burden follicular lymphoma (late-breaking abstract). Proceedings of the American Society of Hematology, Plenary Session; 2011 Dec 6; San Diego (CA)
Taverna C, Bassi S, Hitz F, et al. Rituximab treatment for a maximum of 5 years in follicular lymphoma: safety analysis of the randomized SAKK 35/03 [abstract no. 1802]. Blood 2010; 116: 752
Berinstein N, Grillo-Lopez A, White C, et al. Association of serum rituximab (IDEC-C2B8) concentration and anti-tumor response in the treatment of low-grade or follicular non-Hodgkin’s lymphoma. Ann Oncol 1998; 9: 995–1001
Pettengell E, Schmitz N, Gisselbrecht C, et al. Randomized study of rituximab in patients with relapsed or resistant follicular lymphoma prior to high-dose therapy as in vivo purging and to maintain remission following high-dose therapy [abstract no. 8005]. J Clin Oncol 2010; 28 Suppl. 15s: 574s
Foa R, Di Rocco A, van Hazel G, et al. Maintenance rituximab every 2 months for 2 years is effective and well tolerated in patients with follicular lymphoma with both standard and rapid infusion: updated results from the phase IIIb MAXIMA study [abstract no. 3945]. Blood 2010; 116: 1608
Hochster H, Weller E, Gascoyne R, et al. Maintenance rituximab after cyclophosphamide, vincristine, and prednisone prolongs progression-free survival inadvanced indolent lymphoma: results of the randomized phase III ECOG1496 study. J Clin Oncol 2009; 27: 1607–14
van Oers M, Van Glabbeke M, Giurgeo L, et al. Rituximab maintenance treatment of relapsed/resistant follicular non-Hodgkin’s lymphoma: longterm outcome of the EORTC 20981 phase III randomized intergroup study. J Clin Oncol 2010; 28: 2853–8
Salles G, Seymour J, Offner F, et al. Rituximab maintenance for 2 years in patients with high tumour burden follicular lymphoma responding to rituximab plus chemotherapy (PRIMA): a phase 3, randomized controlled trial. Lancet 2011; 377: 42–51
Solal-Celigny P, Lepage E, Brousse N, et al. Recombinant interferon alfa-2b combined with a regimen containing doxorubicin in patients with advanced follicular lymphoma. New Engl J Med 1993; 329: 1608–14
Steward W, Crowther D, McWilliam L, et al. Maintenance chlorambucil after CVP in the management of advanced stage, low-grade histologic type non-Hodgkin’s lymphoma. Cancer 1988; 61: 441–7
Romaguera J, McLaughlin P, North L, et al. Multivariate analysis of prognostic factors in stage IV follicular low-grade lymphoma. Cancer 1991; 61: 441–7
Soubeyran P, Eghbali H, Bonichon F, et al. Low-grade follicular lymphomas: analysisof prognosis ina series of 281 patients. Eur J Cancer 1991; 27: 1606–13
Bastion Y, Berger F, Bryon P, et al. Follicular lymphomas: assessment of prognostic factors in 127 patients followed for 10 years. Ann Oncol 1991; 2 Suppl. 2: 123–34
Litam P, Swan F, Cabanillas F, et al. Prognostic value of serum beta-2 microglobulin in low-grade lymphoma. Am J Med 1991; 114: 855–60
Leonard R, Hayward R, Prescott R, et al. The identification of discrete prognostic groups in low-grade non-Hodgkin’s lymphoma: The Scotland and Newcastle Lymphoma Group Therapy Working Party. Ann Oncol 1992; 2: 655–62
Horning S. Natural history of and therapy for the indolent non-Hodgkin’ lymphomas. Semin Oncol 1993; 20: 75–80
Cameron D, Leonard R, Mao J, et al. Identification of prognostic groups in follicular lymphoma. Leuk Lymphoma 1993; 10: 89–99
Gospodarowicz M, Bush R, Brown T, et al. Prognostic factors in nodular lymphomas: a multivariate analysis based on the Princess Margaret Hospital experience. Int J Radiat Oncol Biol Phys 1994; 10: 489–92
Denham J, Denham E, Dear K, et al. The follicular non-Hodgkin’s lymphomas, II. Prognostic factors: what do they mean? Eur J Cancer 1996; 32A: 480–90
Decaudin D, Lepage E, Brousse N, et al. Low-grade stage III–IV follicular lymphoma: multivariate analysis of prognostic factors in 484 patients. A study of the Groupe d’Etude des Lymphomes de l’Adulte. J Clin Oncol 1999; 17: 2499–505
Federico M, Vitolo U, Zinzani P, et al. Prognosis of follicular lymphoma: a predictive model based on a retrospective analysisof 987 cases. Blood 2000; 95: 783–9
Maartense E, Le Cessie S, Kluin-Nelemans H, et al. Age-related differences among patients with follicular lymphoma and the importance of prognostic scoring systems: analysis from a population-based non-Hodgkin’s lymphoma registry. Ann Oncol 2002; 13: 1275–84
Lopez-Guillermo A, Monserrat E, Bosch F, et al. Applicability of the International Prognostic Index for aggressive lymphomas to patients with low-grade lymphoma. J Clin Oncol 1994; 12: 1343–6
Aviles A. The International Index is not useful in the classification of low-grade lymphoma. J Clin Oncol 1994; 12: 2766–70
Bastion U, Coiffier B. Is the International Prognostic Index for aggressive lymphoma patients useful for follicular patients? J Clin Oncol 1994; 12: 1340–2
Hermans J, Krol A, van Groningen K, et al. International Prognostic Index for aggressive non-Hodgkin’s lymphoma is valid for all malignancy grades. Blood 1995; 86: 1460–3
Foussard C, Desablens B, Sensebe L, et al. Is the International Prognostic Index for aggressive lymphomas useful for low-grade lymphoma patients? Applicability to stage III–IV patients. Ann Oncol 1997; 8 Suppl. 1: S49–52
Solal-Celigny P, Roy P, Colombat P, et al. Follicular Lymphoma International Prognostic Index. Blood 2004; 104: 1258–65
Formica V, Norman A, Cunningham D, et al. Utility of the Follicular Lymphoma International Prognostic Index and the International Prognostic Index in assessing prognosis and predicting first-line treatment efficacy in follicular lymphoma patients. Acta Haematol 2009; 122: 193–9
Buske C, Hoster E, Dreyling M, et al. The Follicular Lymphoma International Prognostic Index (FLIPI) separates high-risk from intermediate- or low-risk patients with advanced-stage follicular lymphoma treated with rituximab and the combination of cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) with respect to treatment outcome. Blood 2006; 108: 1504–8
Federico M, Bellei M, Marcheselli L, et al. Follicular Lymphoma International Prognostic Index 2: A new prognostic index for follicular lymphoma developed by the International Follicular Lymphoma Prognostic Factor project. J Clin Oncol 2009; 27: 4555–62
Terol M, Teruel A, Amat P, et al. The FLIPI2 score predicts progression-free survival (PFS) and overall survival (OS) in an independent series of follicular lymphoma: a single institution experience [abstract no. 3128]. Blood 2010; 116: 1288
Numata A, Fujimaki K, Tomita N, et al. Retrospective study of the utility of Follicular Lymphoma International Prognostic Index (FLIPI) and FLIPI2 in patients with follicular lymphoma uniformly treated with rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone [abstract no. 3100]. Blood 2010; 116: 1278
Rummel M. Reassessing the standard of care in indolent lymphoma: a clinical update to improve clinical practice. J Natl Compr Canc Netw 2010; 8: S1–S14
Perea G, Altes A, Montoto S, et al. Prognostic indices in follicular lymphoma: a comparison of different prognostic scoring systems. Ann Oncol 2005; 16: 1508–13
Gine E, Montoto S, Bosch F, et al. The Follicular Lymphoma International Prognostic Index (FLIPI) and the histological subtype are the most important factors to predict histological transformation in follicular lymphoma. Ann Oncol 2006; 17: 1539–45
Friedberg J, Taylor M, Cerhan J, et al. Follicular lymphoma in the United States: first report of the National LymphoCare Study. J Clin Oncol 2009; 27: 1202–8
Gallagher C, Gregory W, Jones A, et al. Follicular lymphomas: prognostic factors for response and survival. J Clin Oncol 1986; 4: 1470–80
Shustik J, Quinn M, Connors J, et al. Follicular non-Hodgkin lymphoma grades 3A and 3B have a similar outcome and appear incurable with anthracycline-based therapy. Ann Oncol 2011; 22: 1164–9
Hans C, Weisenburger D, Vose J, et al. A significant diffuse component predicts for inferior survival in grade 3 follicular lymphoma, but cytologic subtypes do not predict survival. Blood 2003; 101: 2363–7
Ganti A, Weisenburger D, Smith L, et al. Patients with grade 3 follicular lymphoma have prolonged relapse-free survival following anthracycline-based chemotherapy: The Nebraska Lymphoma Study Group Experience. Ann Oncol 2006; 17: 920–7
Bartlett N, Rizeq M, Dorfman R, et al. Follicular large-cell lymphoma: intermediate or low-grade? J Clin Oncol 1994; 12: 1349–57
Rodriguez J, McLaughlin P, Hagemeister F, et al. Follicular large cell lymphoma: an aggressive lymphoma that often presents with favorable prognostic features. Blood 1999; 93: 2002–7
Wendum D, Sebban C, Gaulard P, et al. Follicular large-cell lymphoma treated with intensive chemotherapy: an analysis of 89 cases included in the LNH87 trial and comparison with the outcome of diffuse large B-cell lymphoma. J Clin Oncol 1997; 15: 1654–63
Bierman P. Natural history of follicular grade 3 non-Hodgkin’s lymphoma. Curr Opin Oncol 2007; 19: 433–7
Chau I, Jones R, Cunningham D, et al. Outcome of follicular lymphoma grade 3: is anthracycline necessary as front-line therapy? Br J Cancer 2003; 89: 36–42
Miller T, Grogan T, Dahlberg S, et al. Prognostic significance of the Ki-67-associated proliferative antigen in aggressive non-Hodgkin’s lymphomas: a prospective Southwest Oncology Group trial. Blood 1994; 83: 1460–6
Frost M, Newell J, Lones M, et al. Comparative immunohistochemical analysis of pediatric Burkitt lymphoma and diffuse large B-cell lymphoma. Am J Clin Pathol 2004; 121: 384–90
Thorns C, Kalies K, Fischer U, et al. Significant high expression of CD23 in follicular lymphoma of the inguinal region. Histopathology 2007; 50: 716–9
Naresh K. MUM1 expression dichotomizes follicular lymphoma into predominantly, MUM1-negative low-grade and MUM1-positive high-grade subtypes. Haematologica 2007; 92: 267–8
Llanos M, Alvarez-Arguelles H, Aleman R, et al. Prognostic significance of Ki-67 nuclear proliferative antigen, bcl-2 protein, and p53 expression in follicular and diffuse large B-cell lymphoma. Med Oncol 2001; 18: 15–22
Broyde A, Boycov O, Strenov Y, et al. Role and prognostic significance of the Ki-67 index in non-Hodgkin’s lymphoma. Am J Hemotol 2009; 84: 338–43
Salto B, Shiozawa E, Yamochi-Onizuka T, et al. Efficacy of rituximab plus chemotherapy in follicular lymphoma depends on Ki-67 expression. Pathol Int 2004; 54: 667–74
Wang S, Wang L, Hochberg E, et al. Low histologic grade follicular lymphoma with high proliferation index: morphologic and clinical features. Am J Surg Pathol 2005; 29: 1490–6
Glas A, Kersten M, Delahaye L, et al. Gene expression profiling in follicular lymphoma to assess clinical aggressiveness and to guide the choice of treatment. Blood 2005; 105: 301–7
Michaels J, Foria V, Mead B, et al. Immunohistochemical analysis of the antiapoptotic Mcl-1 and Bcl-2 proteins in follicular lymphoma. Br J Haematol 2006; 132: 743–6
Zhao W, Daneshpouy M, Mounier N, et al. Prognostic significance of bcl-cL gene expression and apoptotic cell counts in follicular lymphoma. Blood 2004; 103: 695–7
Gulmann C, Espina V, Petricoin E, et al. Proteomic analysis of apoptotic pathways reveals prognostic factors infollicular lymphoma. Clin Cancer Res 2005; 11: 5847–55
Torlakovic E, Bilalovic N, Golouh R, et al. Prognostic significance of PU.1 in follicular lymphoma. J Pathol 2006; 209: 352–9
O’Shea D, O’Riain C, Taylor C, et al. The presence of TP53 mutation at diagnosis of follicular lymphoma identifies a high-risk group of patients with shortened time to disease progression and poorer overall survival. Blood 2008; 112: 3126–9
Bjorck E, Ek S, Landgren O, et al. High expression of cyclin B1 predicts a favorable outcome in patients with follicular lymphoma. Blood 2005; 105: 2908–15
Krishnadasan R, Bifulco C, Kim J, et al. Overexpression of SOCS3 is associated with decreased survival in a cohort of patients with de novo follicular lymphoma. Brit J Haematol 2006; 135: 72–5
Koster A, van Krieken J, Mackenzie M, et al. Increased vascularization predicts favorable outcome in follicular lymphoma. Clin Cancer Res 2005; 11: 154–61
Farinha P, Masouldi H, Skinnider B, et al. Analysis of multiple biomarkers shows that lymphoma-associated macrophage (LAM) content is an independent predictor of survival in follicular lymphoma (FL). Blood 2005; 106: 2169–74
Canioni D, Salles G, Mounier N, et al. High numbers of tumor-associated macrophages have an adverse prognostic value that can be circumvented by rituximab in patients with follicular lymphoma enrolled onto the GELA-GOELAMS FL-2000 trial. J Clin Oncol 2008; 26: 440–6
Wahlin B, Aggarwal M, Montes-Moreno S, et al. A unifying microenvironment model in follicular lymphoma: outcome is predicted by programmed death-1-positive, regulatory, cytotoxic, and helper T cells and macrophages. Clin Cancer Res 2010; 16: 637–50
Dave S, Wright G, Tan B, et al. Prediction of survival in follicular lymphoma based on molecular features of tumor-infiltrating immune cells. N Engl J Med 2004; 351: 2159–69
Sakhinia E, Glennie C, Hoyland J, et al. Clinical quantitation of diagnostic and predictive gene expression levels in follicular and diffuse large B-cell lymphoma by RT-PCR gene expression profiling. Blood 2007; 109: 3922–8
Glas A, Knoops L, Delahaye L, et al. Gene-expression and immuno-histochemical study of specific T-cell subsets and accessory cell types in the transformation and prognosisoffollicular lymphoma. JClin Oncol 2007; 25: 390–8
Alvaro T, Lejeune M, Camacho F, et al. The presence of STAT1-positive tumor-associated macrophages and their relation to outcome in patients with follicular lymphoma. Haematologica 2006; 91: 1605–12
Taskinen M, Karjalainen-Lindsberg M, Nyman H, et al. A high tumor-associated macrophage content predicts favorable outcome in follicular lymphoma patients treated with rituximab and cyclophosphamide-doxorubicin-vincristine-prednisone. Clin Cancer Res 2007; 13: 5784–9
Alvaro T, Lejeune M, Salvado M, et al. Immunohistochemical patterns of reactive microenvironment are associated with clinicobiologic behavior in follicular lymphoma patients. J Clin Oncol 2006; 24: 5350–7
Farinha P, Campo E, Banham A, et al. The architectural pattern of FOXP3+ T cells is an independent predictor of survival in patients with follicular lymphoma (FL) [abstract]. Mod Pathol 2006; 19: 1043a
Farinha P, Han J, Al-Tourah A, et al. The tumor microenvironment measured by flow cytometry predicts overall survival and transformation risk in follicular lymphoma [abstract no. 2406]. Blood 2006; 108
Ai W, Czerwinski D, Horning S, et al. Tumor-infiltrating T cells are not predictive of clinical outcome in follicular lymphoma [abstract no. 824]. Blood 2006; 108
Lee A, Clear A, Calaminici M, et al. Number of CD 4+ cells and location of forkhead box protein P3-positive cells in diagnostic follicular lymphoma tissue microarrays correlates with outcome. J Clin Oncol 2006; 24: 5052–9
Carreras J, Lopez-Guillermo A, Fox B, et al. High numbers of tumorinfiltrating FOXP-3 regulatory T cells are associated with improved survival in follicular lymphoma. Blood 2006; 108: 2957–64
Strickler J, Copenhaver C, Rojas V, et al. Comparison of host cell infiltrates: in patients with follicular lymphoma with and without spontaneous regression. Am J Clin Pathol 1988; 90: 257–61
Acknowledgements
No sources of funding were used to prepare this manuscript. The authors have no conflicts of interest that are directly relevant to the content of this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hagemeister, F.B. ‘Watch and Wait’ as Initial Management for Patients with Follicular Lymphomas. BioDrugs 26, 363–376 (2012). https://doi.org/10.1007/BF03261894
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03261894