
Abstract
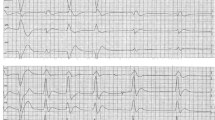
Sudden cardiac death in the absence of apparent structural heart disease is an uncommon phenomenon. The majority of these patients do not have ‘normal’ hearts and specific diagnostic tools are required to identify structural or functional abnormalities. We describe the history of a 50-yearold man who survived ventricular fibrillation. Clinical investigation, including a coronary angiography and electrophysiological study, appeared to be normal. An implantable cardioverter defibrillator was inserted. Follow-up Holter monitoring was performed after a recurrent episode of ventricular tachycardia. It demonstrated transient ST-segment elevation. An acetylcholine provocation test was subsequently carried out. Reversible coronary spasm of the left descending coronary artery was found, during which a diagonal branch was occluded. It may be concluded that coronary spasm provocation is of value in the routine diagnostic work-up of patients surviving sudden cardiac death without apparent heart disease. (Neth Heart J 2008;16:239-41.)



Similar content being viewed by others
References
Task Force on Sudden Cardiac Death of the European Society of Cardiology. Eur Heart J 2001;22:1374-450.
Survivors of out-of-hospital cardiac arrest with apparently normal heart. Need for definition and standardized clinical evaluation. Consensus Statement of the Joint Steering Committees of the Unexplained Cardiac Arrest Registry of Europe and of the Idiopathic Ventricular Fibrillation Registry of the United States. Circulation 1997;95:265-72.
Wever EF, Robles de Medina EO. Sudden death in patients without structural heart disease. J Am Coll Cardiol 2004;43:1137-44.
Peeters HA, Sippens Groenewegen A, Wever EF, Ramanna H, Linnenbank AC, Potse M, et al. Clinical application of an integrated 3-phase mapping technique for localization of the site of origin of idiopathic ventricular tachycardia. Circulation 1999;99:1300-11.
Peters RHJ, Wever EFD, Hauer RNW, Robles de Medina EO. Low prevalence of coronary artery spasm in patients with normal coronary angiograms and unexplained ventricular fibrillation. Eur Heart J 1998;19:1070-4.
Prinzmetal M, Kennamer R, Merliss R, et al. Angina pectoris. I. A variant form of angina pectoris; preliminary report. Am J Med 1959;27:375.
Sueda S, Kohno H, Fukuda H, Ochi H, Kawada H, Hayashi Y, et al. Clinical impact of selective spasm provocation tests: comparisons beween acetylcholine and ergonovine in 1508 examinations. Coron Artery Dis 2004;15:491-7.
Takahashi M, Ikeda U, Sekiguchi H, Fujikawa H, Shimada K, Ri T. Guide wire-induced coronary artery spasm during percutaneous transluminal coronary angioplasty. A case report. Angiology 1996; 47:305-9.
Yamada T, Okamoto M, Sueda T, Hashimoto M, Matsuura H, Kajiyama G. Ergonovine-induced alterations in coronary flow velocity preceding onset of occlusive spasm in patients without significant coronary artery stenoses. Am J Cardiol 1998;81:688-93.
Sueda S, Kohno H, Fukuda H, Uraoka T. Did the widespread use of long-acting calcium antagonists decrease the occurrence of variant angina? Chest 2003;124:2074-8.
Verma S, Anderson T. Fundamentals of endothelial function for the clinical cardiologist. Circulation 2002;105:546-9.
Jeong M, Park J, Rhew J, et al. Successful management of intractable coronary spasm with a coronary stent. Jpn Circ J 2000;64:897.
Author information
Authors and Affiliations
Corresponding author
Additional information
Department of Cardiology, Tergooi Hospitals, location Blaricum, the Netherlands
Department of cardiology, Academic Medical Center, Amsterdam, the Netherlands
Department of Cardiology, Amphia Hospital, Breda, the Netherlands
R.J. Walhout Department of Cardiology, Tergooi Hospitals, location Blaricum, PO Box 900, 1250 CA Laren, the Netherlands
Rights and permissions
About this article
Cite this article
Walhout, R.J., de Winter, R.J., Simmers, T.A. et al. Aborted sudden cardiac death in a 52-yearold man without structural heart disease. NHJL 16, 239–241 (2008). https://doi.org/10.1007/BF03086153
Issue Date:
DOI: https://doi.org/10.1007/BF03086153