
Abstract
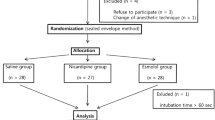
The purpose of this double-blind randomized work was to study the effect of alfentanil and esmolol and their half-dose combination on the increases of heart rate and arterial pressure and on the prolongation of the QTc interval of the ECG occurring during anaesthetic induction. Sixty ASA class I– II patients with mean age ranging from 26 to 32 yr among the groups. Patients were allocated to one of four equal groups to receive saline, esmolol 2 mg · kg− 1, alfentanil 0.03 mg · kg− 1 and alfentanil 0.015 mg · kg− 1 + esmolol 1 mg · kg− 1. Anaesthesia was induced with thiopentone. Succinylcholine was used to facilitate tracheal intubation. Haemodynamic variables were measured non-invasively and the QTc interval with the aid of a microcomputer. Comparisons between the groups were performed using two-way analysis of variance with repeated measures. Both alfentanil and alfentanil-esmolol prevented the increase of heart rate and arterial pressure caused by intubation whereas esmolol prevented only the increase of the heart rate. None of the treatments prevented prolongation of the QTc interval after intubation and only alfentanil prevented that after succinylcholine. The present results suggest that in the prevention of the haemodynamic responses to tracheal intubation, the half-dose combination of alfentanil and esmolol is as effective as alfentanil and superior to esmolol. The combination is preferable to relatively large doses of either drug in circumstances where side effects, such as respiratory depression due to alfentanil or bradycardia due to both drugs should be minimized.
Résumé
Ce travail randomisé en double-aveugle avail pour but l’étude des effets de l’association de l’alfentanil avec l’esmolol à demidoses sur l’augmentation de la fréquence cardiaque et de la pression artérielle, et sur la prolongation de l’intervalle QTc de l’ECG pendant l’induction de l’anesthésie. Soixante patients ASA I et II dont la moyenne d’âge variait entre 25 et 32 ans ont fait partie de l’étude. Ces patients ont été répartis en quatre groupes pour recevoir respectivement: du soluté physiologique, de l’esmolol 2 mg · kg− 1, de l’alfentanil 0,03 mg · kg− 1, et de l’alfentanil 0,015 mg · kg− 1 + esmolol 1 mg · kg− 1. L’anesthésie a été induite au thiopentone. La succinylcholine a été utilisée pour l’intubation. Les paramètres hémodynamiques ont été enregistrés par voie non effractive et l’intervalle QTc grâce à un microordinateur. Les comparaisons ont été établies sur des mesures répétées par analyse de variance. L’alfentanil et l’alfentanil + esmolol ont empêché l’augmentation de la fréquence cardiaque et de la pression artérielle causée par l’intubation alors que l’esmolol n’a été efficace sur l’augmentation de la fréquence cardiaque. Aucun des traitements n’a été efficace pour la prévention de la prolongation de l’intervalle QTc après l’intubation et seul l’alfentanil l’a été après la succinylcholine. Ces résultats suggèrent que pour prévenir les effets hémodynamiques de l’intubation, une demidose d’esmolol avec alfentanil est aussi efficace que l’alfentanil et supérieure à l’esmolol. Cette association est préférable à des doses relativement plus fortes de chacune des drogues dans les circonstances au cours desquelles les effets secondaires comme la dépression respiratoire due à l’alfentanil ou la bradycardie due awe deux drogues doivent être réduites au minimum.
Article PDF
Similar content being viewed by others


References
Black TE, Kay B, Healy TEJ. Reducing the haemodynamic responses to laryngoscopy and intubation. A comparison of alfentanil with fentanyl. Anaesthesia 1984; 39: 883–7.
Saarnivaara L, Klemola U-M. Alfentanil as an adjuvant of balanced anaesthesia for tonsillectomy in adults. Acta Anaesthesiol Scand 1987; 31: 1–6.
Martineau RJ, Tousignant CP, Miller DR, Hull KA. Alfentanil controls the haemodynamic response during rapid-sequence induction of anaesthesia. Can J Anaesth 1990; 37: 755–61.
Scott JC, Ponganis KV, Stanski DR. EEG quantitation of narcotic effect: the comparative pharmacodynamics of fentanyl and alfentanil. Anesthesiology 1985; 62: 234–41.
Bovill JG, Sebel PS, Blackburn CL, Heykants J. The pharmacokinetics of alfentanil (R30209): a new opioid analgesic. Anesthesiology 1982; 57: 439–43.
Camu F, Gepts E, Rucquoi M, Heykants J. Pharmacokinetics of alfentanil in man. Anesth Analg 1982; 61: 657–61.
Miller DR, Martineau RJ, Wynands JE, Hill J. Bolus administration of esmolol for controlling the haemodynamic response to tracheal intubation: the Canadian multicentre trial. Can J Anaesth 1991; 38: 849–58.
Sheppard S, Eagle CJ, Strunin L. A bolus dose of esmolol attenuates tachycardia and hypertension after tracheal intubation. Can J Anaesth 1990; 37: 202–5.
Liu PL, Gatt S, Gugino LD, Mallampati SR, Covino BG. Esmolol for control of increases in heart rate and blood pressure during tracheal intubation after thiopentone and succinylcholine. Can Anaesth Soc J 1986; 33: 556–62.
Oxorn D, Knox JWD, Hill J. Bolus doses of esmolol for the prevention of perioperative hypertension and tachycardia. Can J Anaesth 1990; 37: 206–9.
Knox JWD, Oxorn DC. Esmolol is efficient in controlling post-intubation tachycardia and hypertension. Can J Anaesth 1989; 36: S165–6.
Bazett HC. An analyis of the time relations of the electrocardiogram. Heart 1920; 7: 353–70.
Statistica. StatSoft 1991. Tulsa.
Chung KS, Sinatra RS, Halevy JD, Paige D, Silverman DG. A comparison of fentanyl, esmolol, and their combination for blunting the haemodynamic responses during rapid-sequence induction. Can J Anaesth 1992; 39: 774–9.
Saarnivaara L, Lindgren L. Prolongation of the QT interval during induction of anaesthesia. Acta Anaesthesiol Scand 1983; 27: 126–30.
Saarnivaara L, Lindgren L, Hynynen M. Effects of practolol and metoprolol on QT interval, heart rate and arterial pressure during induction of anaesthesia. Acta Anaesthesiol Scand 1984; 28: 644–8.
Saarnivaara L, Klemola U-M, Lindgen L, Rautiainen P, Suvanto A. QT interval of the ECG, heart rate and arterial pressure using propofol, methohexital or midazolam for induction of anaesthesia. Acta Anaesthesiol Scand 1990; 34: 276–81.
Saarnivaara L, Hiller A, Oikkonen M. QT interval, heart rate and arterial pressure using propofol, thiopentone or methohexital for induction of anaesthesia in children. Acta Anaesthesiol Scand 1993; 37: 419–23.
Greenspan AM, Spielman SR, Horowitz LN, Senior S, Steck J, Laddu A. Electrophysiology of esmolol. Am J Cardiol 1985; 56: 19F-26E
Pala AM, Ricciardelli D, Sanna A, Vinattieri MA. The effect of beta blockers on the QT interval: possible role of mechanisms other than beta block (Italian). Minerva Med 1989; 80: 1283–7.
Dumoulin P, Weissenburger J, Poirier JM, et al. Electrophysiological effects of intravenous sotalol. Relation with plasma levels (French). Arch Mal Coeur Vaiss 1985; 78: 562–8.
Lindgren L, Rautiainen P, Klemola U-M, Saarnivaara L. Haemodynamic responses and prolongation of QT interval of ECG after suxamethonium-facilitated intubation during anaesthetic induction in children: a dose-related attenuation by alfentanil. Acta Anaesthesiol Scand 1991; 35: 355–8.
Scheinin B, Scheinin M, Vuorinen J, Lindgren L. Alfentanil obtunds the cardiovascular and sympathoadrenal responses to suxamethonium-facilitated laryngoscopy and intubation. Br J Anaesth 1989; 62: 385–92.
Forbes RB, Morton GH. Ventricular fibrillation in a patient with unsuspected mitral valve prolapse and prolonged Q-T interval. Can Anaesth Soc J 1979; 26: 424–7.
Medak R, Benumof JL. Perioperative management of the prolonged Q-T interval syndrome. Br J Anaesth 1983; 55: 361–4.
Schwartz PJ, Wblf S. QT interval prolongation as predictor of sudden death in patients with myocardial infarction. Circulation 1978; 57: 1074–7.
Saarnivaara L, Klemola U-M, Lindgren L. QT interval of the ECG, heart rate and arterial pressure using five nondepolarizing muscle relaxants for intubation. Acta Anaesthesiol Scand 1988; 32: 623–8.
Lindgren L, Saarnivaara L. Cardiovascular responses to enflurane induction followed by suxamethonium in children. Br J Anaesth 1983; 55: 269–73.
Lindgren L, Saarnivaara L. Cardiovascular responses to tracheal intubation in small children. Br J Anaesth 1985; 57: 1183–7.
Miller D, Martineau R. Esmolol for control of haemodynamic responses during anaesthetic induction. Can J Anaesth 1989; 36: S164–5.
Lemmens H, Bovill J, Hennis PJ, Burm AGL. Age has no effect on the pharmacodynamics of alfentanil. Anesth Analg 1988; 67: 956–60.
Kirby IJ, Northwood D, Dodson ME. Modification by alfentanil of the haemodynamic response to tracheal intubation in elderly patients. Br J Anaesth 1988; 60: 384–7.
Reid C, Crosby E, Reid D. Sinus arrest following administration of alfentanil (Letter). Can J Anaesth 1991; 38: 540–1.
Scamman F, Ghoneim M, Korttila K. Ventilatory and mental effects of alfentanil and fentanyl. Acta Anaesthesiol Scand 1984; 28: 63–7.
Patrick M, Eager BM, Toft DF, Sebel PS. Alfentanilsupplemented anaesthesia for short procedures. A double-blind comparison with fentanyl. Br J Anaesth 1984; 56: 861–6.
Dimick I, Lingham R, Narang J, Sampson I, Shiang H. Esmolol prevents and suppresses arrhythmias during halothane anaesthesia in dogs. Can J Anaesth 1992: 39: 83–6.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Korpinen, R., Saarnivaara, L., Siren, K. et al. Modification of the haemodynamic responses to induction of anaesthesia and tracheal intubation with alfentanil, esmolol and their combination. Can J Anaesth 42, 298–304 (1995). https://doi.org/10.1007/BF03010706
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03010706