
Abstract
Background
Adrenocortical carcinoma synthesizing solely mineralocorticoids is an unusual disorder which has only been reported in literature in 22 other patients.
Methods
This case report describes a patient presenting with hypokalaemia, hypertension, metabolic acidosis and a left adrenal tumor. Extensive laboratory testing allowed the diagnosis of pure primary hyperaldosteronism without secretion of other steroids.
Results
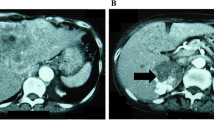
The treatment of choice after establishing the diagnosis biochemically is to remove the tumor surgically. Histologically the lesion within the left adrenal was classified as a benign adrenocortical adenoma. After recurrence of, disease 6 months postoperatively, a widespread retroperitoneal tumor was en bloc resected and malignancy was confirmed by the histological features. When extended total histological examination of the first tumor was performed, capsular invasion was detected in one slice and the diagnosis of adrenocortical cancer was established retrospectively not only on the basis of clinical behavior. Despite precise surgical treatment of the recurrence and chemotherapy, the patient died 14 months after the diagnosis of primary hyperaldosteronism.
Conclusions
Close biochemical and clinical follow-up examinations are necessary in each patient with hormonlly active tumors. Sometimes only the postoperative course discriminates benign and malignant lesions.
Zusammenfassung
Grundlagen
Adrenokortikale Karzinome mit alleiniger Sekretion von Mineralokortikoiden sind sehr selten. In der Literatur finden sich nur 22 gut dokumentierte Fälle.
Methodik
Diese Kasuistik beschreibt einen Patienten mit Hypokaliämie, Hypertonie, metabolischer Azidose und mit einem linksseitigen Nebennierentumor. Die genaue laborchemische Untersuchung erbrachte die ausschließliche Sekretion von Aldosteron.
Ergebnisse
Nach Sicherung der biochemischen Diagnose erfolgte als Behandlung der Wahl die chirurgische Entfernung des Tumors. Die histologische Untersuchung der Nebenniere erbrachte zunächst ein gutartiges Nebennierenrindenadenom. 6 Monate später wurde klinisch und biochemisch ein Tumorrezidiv beobachtet. Es erfolgte en bloc die Exstirpation eines großen, malignen, retroperitonealen Tumors. Nun erfolgte retrospektive die neuerliche histologische Aufarbeitung des ersten Präparats. In einem Schnitt fand sich eine Kapselinvasion als Zeichen eines adrenokortikalen Karzinoms. Trotz erweiterter chirurgischer Resektion und Chemotherapie starb der Patient 14 Monate nach Erstdiagnose des priären Hyperaldosteronismus.
Schlußfolgerungen
Engmaschige biochemische und klinische postoperative Untersuchungen sind bei allen endokrinen Tumoren durchzuführen. Vielfach ermöglicht erst der postoperative Verlauf die Unterscheidung zwischen gut- und bösartigen Tumoren.
Similar content being viewed by others


References
Conn JW: Primary aldosteronism: a new clinical syndrome. J Lab Clin Med 1955;45:661–664.
Litynski M: Nadcisniene tetnice wywolane guzarni korowo-nad-nerczowymi. Pol Tyg Lek 1953;8:204–208.
Richie JP, Gittes RF: Carcinoma of the adrenal cortex. Cancer 1980;45:1957–1964.
King DR, Lack EE: Adrenal cortical carcinoma: A clinical and pathologic study of 49 cases. Cancer 1979;44:239–244.
Mostofi FK, Davis CJ jr: Pathology of urologic cancer, in Javadpour N (ed): Principles and management of urologic cancer. Baltimore, Williams & Wilkins, 1979, p 56.
Young WR jr, Klee GG: Primary aldosteronism: Diagnostic evaluation. Endocrinol Metab Clin North Am 1988;17:367–372.
Farge D, Chatellier G, Pagny JY, Jeunemaitre X, Plouin PF, Corvol P: Isolated clinical syndrome of primary aldosteroniss in four patients with adrenocortical carcinoma. Am J Med 1987;83:635–640.
Slee PHThJ, Schaberg A, van Brummelen P: Carcinoma of the adrenal cortex causing primary hyperaldosteronism. Cancer 1983;51:2341–2345.
Tenschert W, Maurer R, Vetter KH, Vetter W: Primary aldosteronism by carcinoma of the adrenal cortex. Klin Wschr 1987;65:428–432.
Scott HW jr, Sussman CR, Page DL, Thompson N, Gross MD, Lloyd R: Primary hyperaldosteronism caused by adrenocortical. World J Surg 1986;10:646–653.
Fraser AG, Croxson MS, Espiner EA, Synek B: Adrenocortical carcinoma presenting as primary aldosteronism in a young man. Aust N Z J Med 1987;17:60–62.
Greathouse DJ, McDermott MT, Kidd GS, Hofeldt FD: Pure primary hyperaldosteronism due to adrenal carcinoma. Am J Med 1984;76:1132–1136.
Sakashita S, Kashiwagi A, Maru A, Ito Y, Chiba H, Kurosawa S, Inoue K, Koyanagi: Primary aldosteronism due to adrenal cortical carcinoma. J Urol 1984;132:959–961.
Filipecki S, Feltynowski T, Poplawska W, Lapinska K, Krus S, Wocial B, Januszewicz W: Carcinoma of the adrenal cortex with hyperaldosteronism. J Clin Endocrinol Metab 1972;35:225–229.
Hutter AM, Kayhoe DE: Adrenal cortical carcinoma. Am J Med 1966;41:572–580.
Luton JP, Cerdas S, Billaud L, Thomas G, Guilhaume B, Bertagna X, Laudat MH, Louvel A, Chapius Y, Blondeau P, Bonnin A, Bricaire H: Clinical features of adrenocortical carcinoma, prognostic factores, and the effect of mitotane therapy. N Engl J Med 1990;322:1195–1201.
Cohn K, Gottesmann L, Brennan MF: Adrenocortical carcinoma. Surgery 1986;100:1170–1177.
Goebel R, Weiss P: Nebennierenrindencarcinom mit multipler Steroidsekretion. Therapiew Österr 1987;4:395–398.
Brooks RV, McSwiney RR, Prunty FT, Wood FR: Potassium deficiency of renal and adrenal origin. Am J Med 1957;23:391.
Alterman SL, Dominguez C, Lopez-Gomez A, Lieber AL: Primary adrenocortical carcinoma causing aldosteronism. Cancer 1969;24:602–609.
Arteaga E, Biglieri EG, Kater CE, Lopez JM, Schambelan M: Aldosterone-producing adrenocortical carcinoma. Ann Intern Med 1984;101:316–321.
Crane MG, Harris JJ, Herber R: Primary aldosteronism due to an adrenal carcinoma. Ann Intern Med 1965;63:494–503.
Foye LV jr, Feichtmeir TV: Adrenal cortical carcinoma producing solely mineralocorticoid effect. Am J Med 1955;19:966–975.
Stone NN, Janoski A, Muakkassa W, Shpritz L: Mineralocorticoid excess secondary to adrenal cortical carcinoma. J Urol 1984;132:962–965.
Brooks RV, Felix-Davies D, Radcliffe Lee M, Robertson PW: Hyperaldosteronism from adrenal carcinoma. Br Med J 1972;1:220–221.
Grim CE, Ganguly A, Yum MN, Donohue JP, Weinberger MH: Hyperaldosteronism due to unsuspected adrenal carcinoma: discovery during investigation of hypertension in a young woman. J Urol 1980;126:783–786.
Arteaga E, Klein R, Biglieri E: Use of the saline infusion test to diagnose the cause of primary aldosteronism. Am J Med 1985;79:722–727.
Didolkar MS, Bescher RA, Elias EG, Moore RH: Natural history of adrenal cortical carcinoma. Cancer 1981;47:2153–2161.
Hough AJ, Hollifield JW, Page DL, Hartmann WH: Prognostic factors in adrenal cortical tumors. Am J Clin Pathol 1979;72:390–399.
Dohm G: Die Nebennierenrinde, in Doerr W, Seifert G (eds): Spezielle Pathologische Anatomie. Bd 14/12 Pathologie der endokrinen Organe. Berlin-Heidelberg-New York, Springer, 1981, pp 927–943.
Mac Farlane DA: Cancer of the adrenal cortex: The natural history, prognosis and treatment in a study of fifty-five cases. Ann R Coll Surg Engl 1958;23:155–186.
King DR and Lack EE: Adrenal cortical carcinoma. A clinical and pathologic study of 49 cases. Cancer 1979;44:239–244.
Brennan MF: Cancer of the endocrine system, in DeVita V, Hellman S, Rosenberg S (eds): Cancer: Principles and practice of oncology. 2nd ed. Philadelphia, Lippincott, 1985, pp 198–199.
Henley DJ, van Heerden JA, Grant CS, Carney JA, Carpenter PC: Adrenal cortical carcinoma—a continuing challenge. Surgery 1983;94:926–931.
Huk I, Niederle B, Roka R, Funovics J: Intraarterielle Chemotherapie—eine Alternative beim Karzinoid mit Lebermetastasen. Acta Chir Austriaca 1988;20:42–43.
van Slooten H, van Oosterom AT: CAP (cyclophosphamide, doxorubicin, and cisplatin) regimen in adrenocotical carcinoma. Cancer Treat Rep 1983;67: 513–514.
Boven E, Vermorken J, van Slooten H, Pinedo H: Complete response of metastasized adrenal cortical carcinoma with o.p'DDD. Cancer 1984;53:26–29.
Zielinski CC, Schernthaner G: Chemotherapie bei malignen Nebennierentumoren. Acta Med Austriaca 1988;14:120–122.
Schteingardt DE, Motazedi A, Noonan RA: Treatment of adrenal carcinomas. Arch Surg 1982;117:1142.
Erikson B, Öberg K, Curtstedt T, Hemmingsson A, Johansson H, Lind G, Lindgren PG, Thuomas KA, Wilander E, Akerström G: Treatment of hormone-producing adrenocortical cancer with o.p'DDD and streptocozin. Cancer 1987;59:1398–1403.
Dorfinger K, Niederle B, Vierhapper H, Wilfing A, Czernin S, Nowotny P, Waldhäusl W, Grubeck-Loebenstein B: Suramin and the human adrenocortex: results of experimental and clinical studies. Surgery 1991;110:1100–1105.
Vierhapper H, Nowotny P, Mostbeck G, Waldhäusl W: Effect of suramin in adrenocortical carcinoma. Lancet 1989;1:1207–1208.
Allolio B, Jarusch-Hancke C, Reincke M, Arlt U, Winkelmann W: Behandlung des metastasierenden Nebennierencarcinoms mit Suramin. Dtsch Med Wschr 1990;114:381–384.
Decker RA, Elson P, Hogan TF, Citrin DL, Westring DW, Bancrjee TK, Gilchrist KW, Horton J: Eastern Cooperative Oncology Study 1987: Mitotane and adriamycin in patients with advanced adrenal cancer. Surgery 1991;110:1006–1013.
Hosaka Y, Rainwater LM, Grant CS, Young WF, Farrow GM, van Heerden JA, Lieber MM: Adrenocortical carcinoma: Nuclear deoxyrybonucleic acid ploid studied by flow cytometry. Surgery 1987;102:1027–1033.
Icard P, Chapuis Y, Andreassian B, Bernard A, Proye C: Adrenocortical carcinoma in surgically treated patients: A retrospective study on 156 cases by the French Association of Endocrine Surgery. Surgery 1992;112:972–980.
Bijl M, Bakker AJ, Leemhuis MP: Mineralocorticoid excess due to precursors only in a patient with adrenal cortical carcinoma. Neth J Med 1992;41:280–283.
Pommier RF, Brennan MF: An eleven-year experience with adrenocortical carcinoma. Surgery 1992;112:963–971.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Ludvik, B., Niederle, B., Roka, R. et al. Isolated primary aldosteronism in adrenocortical carcinoma: A case report and review of literature. Acta Chir Austriaca 25, 212–216 (1993). https://doi.org/10.1007/BF02602106
Issue Date:
DOI: https://doi.org/10.1007/BF02602106