
Abstract
Objective: To determine: 1) whether a simple clinical prediction rule could identify emergency department patients with ureteral calculi; 2) whether the kidney, ureter, and bladder (KUB) radiograph provides diagnostic information beyond that obtained from the history and physical examination; and 3) whether ureteral calculi can be diagnosed accurately in the emergency department without emergency excretory urography, commonly known as intravenous pyelography (IVP).
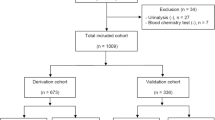
Patients: Two hundred three patients who underwent emergency KUB and IVP studies for nontraumatic abdominal or flank pain (derivation group) were retrospectively identified from radiology department records; 72 patients were prospectively evaluated in the emergency department for suspected ureteral stones (validation group).
Measurements: Clinical information included age, gender, characteristics of pain, associated symptoms, presence of fever, history of ureteral calculi, whether a stone was passed, and results of urinalysis and KUB and IVP studies. All KUB and IVP radiographs were independently reviewed by a radiologist blinded to the patient’s clinical information and urinalysis results.
Design: Stepwise linear discriminant analysis was used to derive a four-item prediction rule from the derivation group and the validation group; the areas under the receiver operating characteristic (ROC) curves and the misclassification rates were compared.
Results: The four-item rule (acute onset, flank pain, hematuria, and positive KUB radiograph) correctly classified 83% of patients in the derivation group and 90% in the validation group. The four-item rule had an ROC area of 0.86 in the derivation group and 0.89 in the validation group. The KUB radiograph significantly improved the discriminant ability of the two history items and the urinalysis result. Thirty-three percent of patients were identified to be in a subset with a 96% probability of having a stone.
Conclusion: These findings, which should be confirmed in another emergency department, suggest that subsets of patients with suspected ureteral calculi may be managed without emergency IVP; this approach thereby reduces the time a patient spends in the emergency department, radiation exposure, expense, and morbidity.
Similar content being viewed by others


References
Johnson CM, Wilson DM, O’Fallon WM, Malek RS, Kurland LT. Renal stone epidemiology: a 25-year study in Rochester, Minnesota. Kidney Int. 1979;16:624–31.
Sierakowski R, Finlayson B, Landes RR, Finlayson CD, Sierakowski N. The frequency of urolithiasis in hospital discharge diagnoses in the United States. Invest Urol. 1978;15:438–41.
Stewart C. Nephrolithiasis. Emerg Med Clin North Am. 1988;6:617–30.
Brown DC. Kidney stones: current issues in diagnosis and therapy. Postgrad Med. 1982;72(Dec):124–33.
Zangerle KF, Iserson KV, Bjelland JC, Criss E. Usefulness of abdominal flat plate radiographs in patients with suspected ureteral calculi. Ann Emerg Med. 1985;14:316–9.
Coe FL. Clinical stone disease. Contemp Issues Nephrol. 1980;5:1–12.
Garrick RE, Goldfarb S. Approach to the patient with renal lithiasis. In: Kelley WN, DeVita VT Jr, DuPont HL, et al. (eds). Textbook of internal medicine. Philadelphia: J. B. Lippincott, 1989;871–5.
O’Brien WM, Rotolo JE, Pahira JJ. New approaches in the treatment of renal calculi. Am Fam Physician. 1987;36(Nov):181–94.
Drach GW. Urinary lithiasis. In: Walsh PC, Gittes RF, Perlmutter AD, Stamey TA (eds). Vol. 1. Campbell’s urology. 5th edition. Philadelphia: W. B. Saunders, 1986;1094–190.
Sandler CM, Burke JT. Radiology of the urinary system in the emergency department. Emerg Med Clin North Am. 1985;3:507–24.
Thornbury JR, Parker TW. Ureteral calculi. Semin Roentgenol. 1982;17:133–9.
Singh EO, Malek RS. Calculus disease in the upper urinary tract. Semin Roentgenol. 1982;17:113–32.
Spirnak JP, Resnick MI. Urinary stones. Prim Care. 1985;12:735–59.
Roth CS, Bowyer BA, Berquist TH. Utility of the plain abdominal radiograph for diagnosing ureteral calculi. Ann Emerg Med. 1985;14:311–5.
Rhea JT, DeLuca SA, Toombs BD. Evaluation of a sequence of diagnostic tests using the workup of a ureteral stone as a model. Med Care. 1982;20:843–8.
Court-Brown CM. Diagnosis of renal colic in the casualty department. Practitioner. 1979;222:387–9.
Griner PF, Mayewski RJ, Mushlin AI, Greenland P. Selection and interpretation of diagnostic tests and procedures: principles and applications. Ann Intern Med. 1981;94:553–600.
Kleinbaum DG, Kupper LL, Morgenstern H. Epidemiologic research: principles and quantitative methods. Belmont, CA: Life-time Learning Publications, 1982.
Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology. 1982;143:29–36.
Mutgi A, Williams JW, Nettleman M. Renal colic: utility of the plain abdominal roentgenogram. Arch Intern Med. 1991;151:1589–92.
Van Arsdalen KN, Banner MP, Pollack HM. Radiographic imaging and urologic decision making in the management of renal and ureteral calculi. Urol Clin North Am. 1990;17:171–90.
Wasson JH, Sox HC, Neff RK, Goldman L. Clinical prediction rules: applications and methodological standards. N Engl J Med. 1985;313:793–9.
Author information
Authors and Affiliations
Additional information
Received from the Division of Area Medicine and the Department of Health Sciences Research, Mayo Clinic and Mayo Foundation, Rochester, Minnesota, and the Department of Diagnostic Radiology, Mayo Clinic Jacksonville, Jacksonville, Florida.
Rights and permissions
About this article
Cite this article
Elton, T.J., Roth, C.S., Berquist, T.H. et al. A clinical prediction rule for the diagnosis of ureteral calculi in emergency departments. J Gen Intern Med 8, 57–62 (1993). https://doi.org/10.1007/BF02599984
Issue Date:
DOI: https://doi.org/10.1007/BF02599984