
Abstract
Aspiration pneumonia is the leading cause of death among the elderly. Modified-texture foods, i.e., foods with altered consistency, are recommended in order to maintain both normal swallowing and adequate nutrition, which is also expected to reduce aspiration pneumonia, when elderly people are suspected to suffer from disorders of eating and/or swallowing. However, it is reported that overly-restrictive diets have been provided to most residents given modified-texture diets. Furthermore, there is scant empirical evidence of the medical effectiveness of food texture-modification. Little attention has been paid to the effect of the consistency of food substances, as well as the ability of mastication, on general health. Our cross-sectional studies showed that eaters of regular foods have lower incidences of pneumonia and fever, while those eating modified-texture, i.e., softer and finer, foods have higher incidences of pneumonia and fever. In this review, the effects of interventions for prevention of aspiration pneumonia were overviewed then the impact of the consistency of food substances on the health of the elderly and the direction of further research was discussed.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others

Keywords
1 Pneumonia and its Causes in the Elderly
Pneumonia is the leading cause of death among the elderly in many countries including Japan [1, 2]. The overall mortality rate ranges from 20 to 50 %, with a rate as high as 80 % reported in some studies [3–6]. It is also the most serious common infection that occurs in nursing homes, with a high case-fatality rate and considerable mortality among survivors. The reported incidence of nursing home-acquired pneumonia has ranged from 0.3 to 2.5 episodes per 1,000 days of resident care [7, 8]. Pneumonia can be classified in several ways, most commonly by where it was acquired (hospital-acquired, nursing home-acquired and community-acquired pneumonia), but may also be classified by the cause (Bronchiolitis obliterans organizing, eosinophilic, aspiration, Dust pneumonia and so on) or the area of lung that is affected [9]. Among these causes, aspiration is an important pathogenic mechanism for pneumonia among the elderly and the management of patients with pneumonia with aspiration factors is a major medical problem [10].
2 Risk Factor Cause of Aspiration Pneumonia
A large number of studies of the bacteriology of aspiration pneumonia suggest that the combination of colonization of the oropharynx with bacterial pathogens and microaspiration of saliva containing these bacteria may be the most common source of aspiration pneumonia [11–13].
Mylotte [1] reviewed risk factors for pneumonia included poor functional status [14, 15], difficulties swallowing [15, 16], dementia and stroke [17, 18], poor oral hygiene or inadequate oral care [19, 20], presence of a nasogastric tube [14], use of sedatives [21], occurrence of an unusual event defined as confusion, agitation, falls, or wandering [15], chronic lung disease [22], tracheostomy [22], increasing age [16], and male sex [16]. Mitchell et al. [23] showed that advanced age and significant cognitive impairment increased the risk of aspiration. The most common causes of difficulties in swallowing among the elderly are dementia and stroke [24].
Logistic regression analyses identified the significant predictors of aspiration pneumonia. The best predictors, in one or more groups of subjects, were dependency for feeding, dependency for oral care, number of decayed teeth, tube feeding, more than one medical diagnosis, number of medications, and smoking [25]. Aspiration pneumonia is a multifactorial phenomenon and no single predictor can cause this disease. Langmore [19] concluded that dysphagia and aspiration are necessary but not sufficient conditions for development of pneumonia.
3 Interventions Aimed at Preventing Aspiration Pneumonia
3.1 Overview of Interventions
To reduce risk of aspiration pneumonia, several interventions have been tried clinically. However, a systematic review assessed the effectiveness of the following interventions for prevention of aspiration pneumonia in the elderly: compensatory strategy/positioning changes, dietary interventions, pharmacological therapies, oral hygiene and tube feeding, and it concluded that insufficient data exist to determine the efficacy of positioning strategies, modified-texture foods, oral hygiene, feeding tube placement, or delivery of food in preventing aspiration pneumonia [26]. Though meaningful studies have been carried out, it was suggested that larger, high-quality randomized controlled trials (RCTs) on the efficacy of preventive interventions are warranted [26].
Individuals with dementia often present feeding difficulties and are susceptible to aspiration pneumonia. Interventions can include behavioural strategies [27], modification of food consistencies [28], postural manoeuvres (for example, chin tuck) [29], pharmaceutical interventions [30], environmental modification [31] or enteral feeding [32]. Still insufficient data exist to determine the efficacy of those interventions. Popular interventions and studies are described below.
3.2 Oral Hygiene
Aspiration of oropharyngeal flora into the lung is the major route of pathogenesis of aspiration pneumonia [33], and colonization of dental plaque and oral mucosa represents a reservoir of potential pathogens that can reach the lung, so it was hypothesized that poor oral hygiene increases the rate of colonization of dental plaque and oral mucosa to cause aspiration pneumonia [34]. A study carried out in Japanese nursing homes demonstrated that residents randomly selected to follow an intensive oral care regimen had a significantly lower proportion of episodes of pneumonia than did residents following a standard oral care regimen [35]. A systematic review indicates three oral hygiene care intervention studies involving 470 participants resulted in improved oral hygiene in patients and reduced the incidence of pneumonia amongst the intervention group in a stroke ward [36].
3.3 Dietary Intervention
Since modifications in dietary textures and fluid viscosities are common dysphagia interventions, they are also expected to be effective in reducing aspiration pneumonia. Increasing the viscosity of a fluid can lead to a reduced rate of liquid bolus transit and increased sensory awareness [37, 38]. It can also influence opening of the upper oesophageal sphincter [39]. This reduced rate of bolus movement and increase in sensory awareness may enhance the safety and efficiency of swallowing, thus reducing the risk of aspiration or penetration of fluid into the airway. It is believed that increasing the viscosity of the fluid bolus by altering its consistency allows individuals a better opportunity to swallow with a reduced risk of airway compromise.
Similarly, altering the consistency of foods is thought to lead to physiological changes which can reduce an individual’s risk of aspiration. Foods are often modified according to a patient’s oral motor control [20]. Reduced incidence of aspiration pneumonia was noted in a study where the participants were randomized to a soft mechanical diet and thickened liquids [40, 41]. However, it was summarized there is scant empirical evidence of its medical effectiveness by a systematic review [42]. This topic is discussed in later section (Sect. 29.5).
3.4 Swallowing Therapy
Most speech-language therapists have traditionally focused their therapy on teaching swallowing maneuvers, postural changes or instituting dietary alterations, so as to minimize pneumonia by making the swallow more effective. A systematic review of all RCTs with patients recovering from stroke and dysphagia [42] identify two RCTs which assessed the effectiveness of swallowing treatment programmes [43, 44]. Foley et al. [42] concluded that the evidence from these trials is weakened by small sample sizes, the lack of a control group, insufficient statistical comparisons, or inability to achieve clinically significant treatment effects.
3.5 Controlling Gastroesophageal Reflux
Gastroesophageal reflux has been estimated to occur in one-third of the elderly population. Aspiration of material from the stomach can damage the trachea in those with gastroesophageal reflux. Postural changes include the chin tuck position, upright position during and after meals to prevent gastroesophageal reflux, and semirecumbent position in bed. However, few data exist to support any of these strategies [26].
3.6 Improvement of Nutrition
The prevalence of malnutrition has been estimated to be between 40 and 60 % for patients aged 65 and older who are hospitalized in short-term units or convalescence and rehabilitation units and 13–50 % in institutions [45]. Infectious risk is increased in the case of malnutrition [46], and hypoalbuminemia is associated with an increased risk of mortality [17]. Most studies on pneumonia have demonstrated a role of malnutrition in the development of the infection, but the results are somewhat contradictory [47]. Two RCTs evaluate that supplementation may improve survival rate [27, 48]. On the other hand, there was no difference for case fatality, or death or dependency, with fluid supplementation and nutritional supplementation, although nutritional supplementation was associated with reduced pressure sores, increased energy intake and protein intake [49]
3.7 Enteral Tube Feeding
One of the primary reasons given for the use of feeding tubes is to reduce the risk of aspiration among adults with swallowing disturbances. Non-oral feeding is believed to prevent aspiration pneumonia, improve function, promote physical comfort and prolong life. However, the evidence does not support (or refute) these assumptions. Several studies of tube-fed patients who are taking no foods or liquids by mouth have shown that tube feeding is associated with a higher rate of pneumonia than in patients who are eating [19, 50–57].
In one study, aspiration pneumonia was diagnosed in 44 % of the tube-fed patients with acute stroke [58]. Other studies showed incidence of aspiration pneumonia vary from 7 to 62 % in patients fed by feeding tube [59]. Nakajoh et al. [60] found that the incidence of pneumonia was significantly higher in post-stroke patients on oral feeding than in those with nasogastric tubes (NGT) feeding during a one-year follow-up period (54.3 % versus 13.2 %, p < 0.001). As there are some evidence that patients with a very short life expectancy [61, 62], there appears to be a limited role for tube feeding among adults with swallowing disturbances, and some have suggested that their use should be discouraged [50].
3.8 Pharmacologic Therapies
From a systematic review [26], two RCTs were found to address pharmacological interventions. Use of amantadine prevented pneumonia in one trial among nursing home residents [63]. The antithrombotic agent cilostazol prevented aspiration pneumonia in another trial but resulted in excessive bleeding [64]. However the use of these agents (amantadine and cilostazol) for reducing aspiration pneumonia is unlikely to be accepted in practice. Amantadine is known to cause gastrointestinal and neurological side effects, and it has a propensity to interact with psychotropic medications [26]. Treatment with antibiotics can be difficult among the elderly because of an inability to identify the pathogen, altered drug metabolism, and associated medication side effects [65]. The efficacy of pneumococcal vaccine in the elderly population has been the subject of considerable debate as a result of the lack of prospective, RCTs [66, 67]. Despite this limitation, experts recommend vaccination of all elderly people because the vaccine is safe, inexpensive, and cost effective [68, 69].
4 Benefits of Oral Ingestion
As mentioned in the previous paragraph, several studies have shown that a tube feeding is associated with a higher rate of pneumonia than that among patients who are eating [19, 50–57]. Some studies suggest that an enteral tube feeding may actually increase mortality and morbidity, and reduce QOL [70, 71]. It was shown by a study in animal models [72] and in children [73] that a gastrostomy tube placement may reduce lower oesophageal sphincter pressure and increase the risk of gastroesophageal reflux, with a change in the gastroesophageal angle as the suspected mechanism.
A tube feeding may worsen urinary and faecal incontinence, which is associated with an increased risk of pressure ulcers and also increase gastric secretions [74]. A percutaneous endoscopic gastrostomy (PEG) is an invasive surgical procedure with significant risks. Postoperative complications include aspiration pneumonia, oesophageal perforations, migrations of the tube, haemorrhage and wound infections [75]. Moreover, Leibovitz et al. [76] found that there is a high prevalence of oropharyngeal colonisation with gram-negative bacteria in patients with a tube feeding (both NGT and PEG) compared to orally-fed patients.
In addition, there are ethical issues. Low et al. [77] reported that 69 % of respondents would not agree to fed via a tube.
It is recommended that an artificial feeding should only be considered if dysphagia is thought to be a transient phenomenon and should not generally be used in people with severe dementia for whom dysphagia or disinclination to eat is a manifestation of disease severity [78, 79]. As a result of these guidelines, modified consistency food and fluids are used increasingly with people presenting with dysphagia due to dementia.
5 Food Modification and Pneumonia
5.1 Ways of Food Modification
Altering the consistency of foods is thought to lead to physiological changes which can reduce an individual’s risk of aspiration. The consistency of foods can be altered from a regular texture to ‘extensively modified-texture’
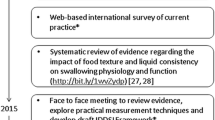
The terminology and definitions of different food and fluid consistencies vary and there is currently no international consensus regarding the terminology that should be used for different consistencies of foods and fluids [80]. For instance, the National Dysphagia Diet is comprised of four levels of food modification with specific food items recommended at each level, namely (1) homogeneous, cohesive, and pudding like, (2) moist, semi-regular, (3) soft-solids, (4) regular [81]. Japan’s Ministry of Health Labor and Welfare sets the following 6 levels. Level 0: Smooth jelly foods without protein, Level 1 Smooth jelly foods with protein, Level 2: Jelly foods with protein, Level 3: Paste containing meat/fish, Level 4: Soft foods, Level 5: Normal diet [80]. However, the International Dysphagia Diet Standardization Initiative (IDDSI) aims to develop global standardized terminology and definitions for modified-texture foods for individuals of all ages with dysphagia, in all care settings and for all cultures by December 2014 [37].
5.2 A Review of Food Modification and Pneumonia
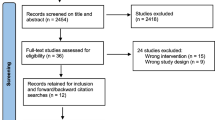
The authors searched MEDLINE, the Cochrane Library and CINAHL, through April 2014, using the key words modification/modified, food/diet, consistency and pneumonia. The authors also hand-searched papers from Dysphagia, Stroke, Physical Medicine and Rehabilitation, Clinical Infectious Diseases, the Journal of the American Geriatric Society and Age and Aging from 1995 to 2014. Reference lists of relevant primary and review articles were searched. Among 59 citations identified, ten articles mentioned the relation between food modification and pneumonia in adults (Table 29.1), while others didn't provide any information about such relations. Of ten studies, five articles were RCTs, two were systematic review, one was quasi-experimental study, and two were just protocols without results.
The benefit of texture-modified foods and/or alteration of fluid viscosity was evaluated in five RCT [40, 84–87] and one quasi-experimental study [82]. Although four [40, 84, 85, 87] of five RCT studies evaluated pneumonia, it was difficult to meta-analyze the overall benefit due to heterogeneity of interventions, timing and duration of therapy and conditions of study population. Sample sizes across studies were small, ranging from 20 [87] to76 [84] and the event rates for pneumonia were low. In one trial [40], the simultaneous manipulation of solid textures and fluid viscosities makes it difficult to establish which component (solid or liquid) was associated with pulmonary benefit. In summary, although modifications in dietary textures and fluid viscosities are common interventions there is scant empirical evidence of their medical effectiveness.
6 Impact of the Consistency of Food Substances on Aspiration Pneumonia
6.1 A Prompt Report from our Study
The importance of oral intake versus enteral tube feeding is widely understood from the physical, mental, social and ethical aspects. It is recognized that oral intake can improve the organic response to stress and thus facilitate the recovery of patients after surgery [88]. Recently, clinicians have been attempting to promote oral intake. However, once oral intake is achieved, less attention has been paid to the consistency of food and to returning from modified-texture foods to regular solid food. It is hypothesized that regular food which requires mastication should promote masticatory function, salivary secretion and lower risk of dental diseases, and consequently promotes nutritional status and development of resistance against infections. Thus, a study considering the relationship between the consistency of food substances and the incidence of pneumonia in elderly people living in a welfare facility was conducted and presented briefly [89].
The subjects were 154 residents (29 males and 125 females; age, mean 87.9 years, range, 69–102 years). The following data were obtained from the facility's records: consistency of food substances, their caloric intake, their general health status (BMI and history of pneumonia), oral health (number of teeth, oral function, dental diseases, and amounts of ten specific microorganisms in the oral cavity). As results, solid food eaters were found to have a lower incidence of pneumonia (11.4 %) than paste food eaters (44.4 %) and those fed liquids through a gastrostomy tube (55.6 %) (χ 2, P < 0.001). This may be because of the higher calorific intake (mean ± SD; 1513.0 ± 135.3 kcal) of regular food eaters compared to paste food eaters (1362.2 ± 178.8 kcal) and those receiving nutrition through a gastrostomy tube (9056.6 ± 176.5 kcal) (ANOVA, P < 0.001). Regular food eaters had better oral function (χ 2, P < 0.001) and fewer microorganisms (ANOVA, P < 0.001). Since this was a cross-sectional study, it was not possible to ascertain causal relationships. However, the results suggest that the consistency of food substances which require mastication has some influence in lowering the incidence of aspiration pneumonia among the elderly.
6.2 Advantage of Mastication of Food
6.2.1 Promoting Physical Activity
Saliva Production
Mastication promotes the production of saliva. Saliva plays a vital role in food oral processing and antimicrobial function [90]. Human saliva consists of electrolytes, mucus, glycoproteins, enzymes, and antibacterial compounds such as secretory IgA and lysozyme [91]. Functions are protection and lubricant (coating oral mucosa to protect from trauma), digestion (moistening foods and helping to create a food bolus, containing enzymes to digest starches and fats), antimicrobial function (a mechanical cleansing action and a specific, e.g., IgA, and a non-specific immunologic action e.g., lysozyme, lactoferrin and myeloperoxidase), pH maintenance (containing various ions which act as a buffer), remineralization of teeth, a taste mediation [91]. Promoting saliva production results in better oral hygiene and improvement of digestions.
Oral Health
Physiologically, oropharyngeal colonization by pathogenic organisms is prevented by the mechanical clearance provided by chewing and swallowing [92].
Helping Enzymes for Digestion
Mastication breaks the food into smaller pieces, increasing efficiency of the digestive enzymes by creating more surface area on food particles for attachment of enzymes.
Oral Function
Using organs, disuse syndromes can be prevented. A physical can prevent disuse syndrome. Physical inactivity predictably leads to deterioration of many body functions. Regular food requires more chewing time than modified-texture foods, thus it is expected to activate related organs. Though there is insufficient evidence concerning the elderly, gum chewing decreases time to flatus and first defecation after surgery [93] and chewing and a fiber rich diet is suggested to help development in children [94].
Cognitive Impairment
Although this theory is not confirmed in humans, the relationship between mastication and cognitive impairment has been studied in various animal models [95, 96]. Three mechanisms explaining these animal studies were proposed to relate to a neurogenesis in the part of the brain that is associated with cognition: an increase in corticosterone and a decrease of hippocampal glucocorticoid associated with stress, a disruption of cholinergic neurotransmitter system associated with learning ability, and spatial memory [97]. In humans, though several studies have been undertaken, there is insufficient substantial evidence to demonstrate the relationship [97].
6.2.2 Better Nutrition
Although it is widely believed that altering the consistency of foods and fluids can help individuals with dementia and swallowing difficulty more safely and more efficiently, the use of modified-texture foods, particularly pureed diets, has been implicated in the high prevalence of undernutrition [98]. There is little clinical evidence to explain how the use of modified-texture foods causes undernutrition, but previous studies have found that modified-texture foods, specifically pureed types, offer poor nutritional value compared with regular foods [99–101]. The modified-texture foods may also lead to dehydration and malnutrition. It can be unpalatable and the choice of food that is recommended may be limited [102, 103]. One study reported that if the consistency of food was changed from paste to soft solid food which requires mastication, people improved through the intervention (n = 13) by gaining weight [104].
6.3 QOL
A result of satisfaction survey among residents in long-term care indicates that food is the topic with the most variability, reflecting not only a high level of interest in this important daily activity, but also a range in satisfactions [105]. They may resist consuming modified texture foods instead of appealing the texture and taste because they are often unappealing in their appearance, texture, and taste [106]. Some studies have shown that patients may be embarrassed eating pureed foods in front of other people, resulting in their social isolations [107]. Niezgoda et al. [108] reported several issues and challenges in relation to modified-texture foods.
6.4 Consideration of Modified-Texture Foods for the Elderly
Assessment of eating ability and adapting modified-texture foods has not been standardized in clinical settings [108]. One study indicated that among nursing home residents, 91 % of nursing home residents with modified-texture foods were placed on overly restrictive diets [109]. Only 5 % of these patients were identified to be on an appropriate diet level matching their swallowing ability and 4 % of patients were placed on diets above their clinically measured swallowing ability. Furthermore, low acceptability and resulting poor adherence to modified-texture food/liquids can contribute to increased risk of inadequate nutrition in elderly patients with dysphagia.
The phenomenon of elderly persons not eating is observed daily in clinical practice. However, assessment of the causes is highly complex and providing proper care is difficult. If caused by dysphasia from stroke or dementia, the risk from diseases and comorbidity should be carefully taken into consideration and provide medical treatment. If caused by poor oral conditions such as losing teeth or edentulism [110, 111], dental treatment should be the first choice. If caused by the physiological changes that occur with aging, such as decreased sense of taste, hunger, and appetite, or fatigue after hospitalization, promoting functions may be taken into consideration to avoid disuse syndromes. Thus, it is important to keep personal history records and watch individuals carefully as well as to carry out further researches which will develop standardized care.
7 What Further Research Needs to be Done?
Review articles referred in this part concluded that there is a clear and pressing need for high-quality research to identify effective treatments. In the hierarchy of research designs [112], ‘high-quality research’ may indicate high-quality RCTs, which are considered to be evidence of the highest grade as “gold standard”. However, is sufficient evidences provided by RCTs for better clinical practice? The demerits of RCTs are well-known, as well as their advantages. Black [113] discussed many limitations and explained the necessity of observational studies. The issues of limitations of external validity is important. The RCTs are designed to maximize their internal validity to produce similar groups by random allocation. Usually, participants have been selected using strict inclusion and exclusion criteria, consequently characteristics of a study population were limited. In addition, other issues include difficulty in studying rare events, ethical problem, narrowing of the studied question, costs and time [113].
Two studies published in The New England Journal of Medicine in 2000 found that observational studies (with either a cohort or a case–control design) do not overestimate the magnitude of the effects of treatment as compared with those in RCTs [114, 115]. In addition, the range of the point estimates for the effect was wider for RCTs than for the observational studies, possibly due to the limitations of external validity.
As to compensate for the RCTs, comparative effectiveness research (CER) is proposed. CER is the direct comparison of existing health care interventions to determine which work best for which patients and which pose the greatest benefits and harms in the real world. Horn and Gassaway [116] extend the concept to develop practice-based evidence for clinical practice improvement (PBE-CPI) study methodology. PBE-CPI incorporates natural variation within data from routine clinical practice to determine what works, for whom, when, and at what costs. It uses the knowledge of front-line caregivers, who develop study questions and define variables as part of a transdisciplinary team. Its comprehensive measurement framework provides a basis for analyses of significant bivariate and multivariate associations between treatments and outcomes, incorporating patient differences, such as severity of illness [116]. PBE-CPI studies can uncover better practices more quickly than RCTs or sophisticated statistical methods, while achieving many of the same advantages [116].
References
Mylotte J. Nursing home-acquired pneumonia. Clin Infect Dis. 2002;35:1205–11.
Nakajima N, Aiba M, Fukuda Y, Boku S, Isonuma H, Tsuda H, Hayashida Y. Nihon Ronen Igakkai Zasshi. 2009;46(1):71–8.
Pugliese G, Lichtenberg DA. Nosocomial bacterial pneumonia: an overview. Am J Infect Control. 1987;15:249–65.
Garibaldi RA, Brodine S, Matsumiya S. Infections among patients in nursing homes: policies, prevalence, and problems. N J Med. 1981;305(13):731–5.
Bryan CS, Reynolds KL. Bacteremic nosocomial pneumonia: analysis of 172 episodes form a single metropolitan area. Am Rev Respir Dis. 1984;129:668–71.
Wenzel RP. Hospital-acquired pneumonia: overview of the current state of the art for prevention and control. J Clin Microbiol Infect Dis. 1989;8:56–60.
Muder RR. Pneumonia in residents of long-term care facilities: epidemiology, etiology, management, and prevention. Am J Med. 1998;105:319–30.
Medina-Walpole AM, Katz PR. Nursing home–acquired pneumonia. J Am Geriatr Soc. 1999;47:1005–15.
Dunn L. Pneumonia: classification, diagnosis and nursing management. Nurs Stand. 2005;19(42):50–4. doi:10.7748/ns2005.06.19.42.50.c3901.
Sun T, Sun L, Wang R, Ren X, Sui DJ, Pu C, Ren Y, Liu Y, Yang Z, Li F. Clinical efficacy and safety of moxifloxacin versus levofloxacin plus metronidazole for community-acquired pneumonia with aspiration factors. Chin Med J. 2014;127(7):1201–5.
Verghese A, Berk SL. Bacterial pneumonia in the elderly. Medicine. 1983;62(5):271–85.
Finegold SM. Aspiration pneumonia. Rev Infect Dis. 1991;13:S737–42.
Terpenning M, Bretz W, Lopatin D, Langmore S, Dominguez B, Loesche W. Bacterial colonization of saliva and plaque in the elderly. Clin Infect Dis. 1993;16:S314–6.
Alvarez S, Shell CG, Woolley TW, Berk SL, Smith JK. Nosocomial infections in long-term care facilities. J Gerontol. 1988;43:M9–17.
Harkness GA, Bentley DW, Roghmann RJ. Risk factors for nosocomial pneumonia in the elderly. Am J Med. 1990;18:457–63.
Loeb M, McGeer A, McArthur M, Walter S, Simor AE. Risk factors for pneumonia and other lower respiratory tract infections in elderly residents of long-term care facilities. Arch Intern Med. 1999;159:2058–64.
Corti MC, Guralnik JM, Salive ME, et al. Serum albumin level and physical disability as predictors of mortality in older persons. JAMA. 1994;272:1036–42.
Naughton BJ, Mylotte JM, Tayara A. Outcome of nursing home–acquired pneumonia: derivation and application of a practical model to predict 30 day mortality. J Am Geriatr Soc. 2000;48:1292–9.
Langmore SE, Terpenning MS, Schork A, Chen Y, Murray JT, Lopatin D, Loesche WJ. Predictors of aspiration pneumonia: how important is dysphagia? Dysphagia. 1998;13(2):69–81.
Garcia JM, Chambers E. Managing dysphagia through diet modifications. Am J Nurs. 2010;110(11):27–33.
Vergis EN, Brennen C, Wagener M, Muder RR. Pneumonia in longterm care: a prospective case–control study of risk factors and impact on survival. Arch Intern Med. 2001;161:2378–81.
Magaziner J, Tenney JH, DeForge B, Hebel JR, Muncie Jr HL, Warren JW. Prevalence and characteristics of nursing home–acquired infections in the aged. J Am Geriatr Soc. 1991;39:1071–8.
Mitchell SL, Kiely DK, Lipsitz LA. The risk factors and impact on survival of feeding tube placement in nursing home residents with severe cognitive impairment. Arch Intern Med. 1997;157:327–32.
Christmas C. Eating and feeding problems, Geriatric review syllabus. 5th ed. New York: Blackwell; 2002. p. 197–202.
Langmore SE, Terpenning MS, Schork A, Chen Y, Murray JT, Lopatin D, Loesche WJ. Predictors of aspiration pneumonia: how important is dysphagia? Dysphagia. 1998;13:69–81.
Loeb MB, Becker M, Eady A, Walker-Dilks C. Interventions to prevent aspiration pneumonia in older adults: a systematic review. J Am Geriatr Soc. 2003;51(7):1018–22.
Bisch EM, Logemann JA, Rademaker AW, Kahrilas PJ, Lazarus CL. Pharyngeal effects of bolus volume, viscosity, and temperature in patients with dysphagia resulting from neurologic impairment and in normal subjects. J Speech Hear Res. 1994;37(5):1041–59.
Logemann JA, Pauloski BR, Rademaker A, Cook B, Graner D, Milianti F, Beery Q, Stein D, Bowman J, Lazarus C, Heiser MA, Baker T. Impact of the diagnostic procedure on outcome measures of swallowing rehabilitation in head and neck cancer patients. Dysphagia. 1992;7:179–86.
Robbins J, Gensler G, Hind J, Logemann J, Lindblad A, Brand D, et al. Comparison of 2 interventions for liquid aspiration on pneumonia incidence a randomized trial. Ann Intern Med. 2008;148(7):509–18.
Wada H, Nakajoh K, Satoh-Nakagawa T, Suzuki T, Ohrui T, Arai H, Sasaki H. Risk factors of aspiration pneumonia in Alzheimer’s disease patients. Gerontology. 2001;47(5):271–6.
Koss E, Gilmore C. Environmental interventions and functional abilities of AD patients. In: Vellas B, Filten J, Frisoni G, editors. Research and practice in Alzheimer’s disease. New York: Springer; 1998. p. 185–91.
Kuo S, Rhodes R, Mitchell S, Mor V, Teno J. Natural history of feeding tube use in nursing home residents with advanced dementia. J Am Med Dir Assoc. 2009;10(4):264–70.
Verghese A, Berk SL. Bacterial pneumonia in the elderly. Medicine. 1983;62:271–85.
Scannapieco FA, Mylotte JM. Relationships between periodontal disease and bacterial pneumonia. J Periodontol. 1996;67:1114–22.
Yoneyama T, Yoshida M, Ohrui T, et al. Oral care reduces pneumonia in older patients in nursing homes. J Am Geriatr Soc. 2002;50:430–3.
Brady M, Furlanetto D, Hunter RV, Lewis S, Milne V. Staff-led interventions for improving oral hygiene in patients following stroke. Cochrane Database Syst Rev. 2006;4, CD003864.
International Dysphagia Diet Standardisation Initiative. International dysphagia diet standardisation initiative. 2012. https://docs.google.com/file/d/0B1gDNrkHwLPcR25qMDJLSjJ3RG8/edit?pli=1. Accessed 2 May 2014.
Troche MS, Sapienza CM, Rosenbek JC. Effects of bolus consistency on timing and safety of swallow in patients with Parkinson’s disease. Dysphagia. 2008;23:26–32.
Bisch EM, Logemann JA, Rademaker AW, Kahrilas PJ, Lazarus CL. Pharyngeal effects of bolus volume, viscosity, and temperature in patients with dysphagia resulting from neurologic impairment and in normal subjects. J Speech Lang Hear Res. 1994;37(5):1041–59.
Groher ME. Bolus management and aspiration pneumonia in patients with pseudobulbular dysphagia. Dysphagia. 1987;1:215–6.
DePippo KL, Holas MA, Reding MJ, et al. Dysphagia therapy following stroke: a controlled trial. Neurology. 1994;44:1655–60.
Foley N, Teasell R, Salter K, Kruger E, Martino R. Dysphagia treatment post stroke: a systematic review of randomised controlled trials. Age Ageing. 2008;37(3):258–64. doi:10.1093/ageing/afn064.
Carnaby G, Hankey GJ, Pizzi J. Behavioural intervention for dysphagia in acute stroke: a randomised controlled trial. Lancet Neurol. 2006;5:31–7.
DePippo KL, Holas MA, Reding MJ, Mandel FS, Lesser ML. Dysphagia therapy following stroke: a controlled trial. Neurology. 1994;44:1655–60.
Constans T, Alix E, Dardaine V. Protein-energy malnutrition. Diagnostic methods and epidemiology. Presse Med. 2000;16:2171–6.
Potter J, Klipstein K, Reilly JJ, et al. The nutritional status and clinical course of acute admissions to a geriatric unit. Age Ageing. 1995;24:131–6.
Rothan-Tondeur M, Meaume S, Girard L, Weill-Engerer S, Lancien E, Abdelmalak S, Rufat P, Le Blanche AF. Risk factors for nosocomial pneumonia in a geriatric hospital: a control–case one-center study. J Am Geriatr Soc. 2003;51(7):997–1001.
Potter JM, Langhorne P, Roberts M. Routine protein energy supplementation in adults: systematic review. BMJ. 1998;317:495–501.
Geeganage C, Beavan J, Ellender S, Bath PM. Interventions for dysphagia and nutritional support in acute and subacute stroke. Cochrane Database Syst Rev. 2012;10:CD000323.
Gillick M. Rethinking the role of tube feeding in patients with advanced dementia. N Engl J Med. 2000;342:206–10.
Sitzmann JV. Nutritional support of the dysphagic patient: methods, risks, and complications of therapy. J Parenter Enteral Nutr. 1990;14(1):60–3.
Johnson ER, McKenzie SW, Sievers A. Aspiration pneumonia in stroke. Arch Phys Med Rehabil. 1993;74:973–6.
Kidd D, Lawson J, Nesbitt R, MacMahon J. The natural history and clinical consequences of aspiration in acute stroke. Q J Med. 1995;88:409–13.
Harkness GA, Bentley DW, Roghmann KJ. Risk factors for nosocomial pneumonia in the elderly. Am J Med. 1990;89:457–63.
Croghan JE, Burke EM, Caplan S, Denman S. Pilot study of 12-month outcomes of nursing home patients with aspiration on videofluoroscopy. Dysphagia. 1994;9:141–6.
Feinberg MJ, Knebl J, Tully J. Prandial aspiration and pneumonia in an elderly population followed over 3 years. Dysphagia. 1996;11:104–9.
Peck A, Cohen C, Mulvihill MN. Long-term enteral feeding of aged demented nursing home patients. J Am Geriatr Soc. 1990;38:1195–8.
Dziewas R, Ritter M, Schilling M, et al. Pneumonia in acute stroke patients fed by nasogastric tube. J Neurol Neurosurg Psychiatry. 2004;75:852–6.
Finucane TE, Bynum JP. Use of tube feeding to prevent aspiration pneumonia. Lancet. 1996;348:1421–4.
Nakajoh K, Nakagawa T, Sekizawa K, et al. Relation between incidence of pneumonia and protective reflexes in post-stroke patients with oral or tube feeding. J Intern Med. 2000;247:39–42.
Wolfsen HC, Kozarek RA, Ball TJ, et al. Long term survival in patients undergoing percutaneous endoscopic gastrosomy and jejunostomy. Am J Gastroenterol. 1990;85:1120–2.
Abuksis G, Mor M, Segal N, Shemesh I, Plout S, Sulkes J, Fraser GM, Niv Y. Percutaneous endoscopic gastrostomy: high mortality rates in hospitalized patients. Am J Gastroenterol. 2000;95(1):128–32.
Nakayama K, Sekizawa K, Sasaki H. ACE inhibitor and swallowing reflex. Chest. 1998;113(5):1425.
Yamaya M, Yanai M, Ohrui T, et al. Antithrombotic therapy for prevention of pneumonia. J Am Geriatr Soc. 2001;49:687–8.
Feinberg MJ, Knebl J, Tully J. Prandial aspiration and pneumonia in an elderly population followed over 3 years. Dysphagia. 1996;11(2):104–9.
Hirschmann JV, Lipsky BA. The pneumococcal vaccine after 15 years of use. Arch Intern Med. 1994;154:373–7.
Fedson DS, Shapiro ED, LaForce FM, et al. Pneumococcal vaccine after 15 years of use: another view. Arch Intern Med. 1994;154:2531–5.
Prevention of pneumococcal disease: recommendations of the Advisory Committee on Immunization Practice (ACIP). MMWR Recomm Rep. 1997;46(RR-8):1–24.
Sisk JE, Moskowitz AJ, Whang W, et al. Cost-effectiveness of vaccination against pneumococcal bacteremia among elderly people. JAMA. 1997;278:1333–9.
Peck A, Cohen CE, Mulvihill MN. Long-term enteral feeding of aged demented nursing home patients. J Am Geriatr Soc. 1990;38(11):1195–8.
Nair S, Hertan H, Pitchumoni CS. Hypoalbuminemia is a poor predictor of survival after percutaneous endoscopic gastrostomy in elderly patients with dementia. Am J Gastroenterol. 2000;95(2):133–6.
Canel DF, Vane DW, Goto S, et al. Reduction of lower esophageal sphincter pressure with Stamm gastrostomy. J Pediatr Surg. 1987;22:54–7.
Grunow JE, Al-Hafidh AS, Tunell WP. Gastroesophageal reflux following percutaneous endoscopic gastronomy in children. J Pediatr Surg. 1989;24:42–5.
Finucane TE, Christmas C, Travis K. Tube feeding in patients with advanced dementia: a review of the evidence. JAMA. 1999;282(14):1365–70.
Candy B, Sampson EL, Jones L. Enteral tube feeding in older people with advanced dementia: findings from a Cochrane systematic review. Int J Palliat Nurs. 2009;15(8):396–404.
Leibovitz A, Plotnikov G, Habot B, et al. Pathogenic colonization of oral flora in frail elderly patients fed by nasogastric tube or percutaneous enterogastric tube. J Gerontol A Biol Sci Med Sci. 2003;58:52–5.
Low JA, Chan DK, Hung WT, Chye R. Treatment of recurrent aspiration pneumonia in end-stage dementia: preferences and choices of a group of elderly nursing home residents. Intern Med J. 2003;33(8):345–9.
National Institute for Health and Excellence. Dementia: supporting people with dementia and their carers in health and social care. London: NICE; 2006.
Royal College of Physicians. Oral feeding difficulties and dilemmas: a guide to practical care towards the end of life, Royal College of Physicians. 2010. http://www.rcplondon.ac.uk/sites/default/files/documents/oral-feeding-difficulties-and-dilemmas.pdf. Accessed 2 May 2014.
Flynn EP, Smith CH, Walsh CD, Walshe M. Modifying the consistency of food and fluids for swallowing difficulties in dementia. Cochrane Database Syst Rev. 2014;4:CD011077.
Teasell R, Foley N, Fisher J, Finestone H. The incidence, management, and complications of dysphagia in patients with medullary strokes admitted to a rehabilitation unit. Dysphagia. 2002;17(2):115–20.
Karagiannis M, Karagiannis TC. Oropharyngeal dysphagia, free water protocol and quality of life: an update from a prospective clinical trial. Hell J Nucl Med. 2014;1:26–9.
Steele CM, Bayley MA, Péladeau-Pigeon M, Stokely SL. Tongue pressure profile training for dysphagia post stroke (TPPT): study protocol for an exploratory randomized controlled trial. Trials. 2013;14:126.
Karagiannis MJ, Chivers L, Karagiannis TC. Effects of oral intake of water in patients with oropharyngeal dysphagia. BMC Geriatr. 2011;1:11–9.
Whelan K. Inadequate fluid intakes in dysphagic acute stroke. Clin Nutr. 2001;20:423–8.
Goulding R, Bakheit AM. Evaluation of the benefits of monitoring fluid thickness in the dietary management of dysphagic stroke patients. Clin Rehabil. 2000;14:119–24.
Garon BR, Engle M, Ormiston C. A randomized control trial to determine the effects of unlimited oral intake of water in patients with identified aspiration. J Neurol Rehabil. 1997;11:139–48.
Brodner G, Van Aken H, Hertle L, Fobker M, Von Eckardstein A, Goeters C, et al. Multimodal perioperative management—combining thoracic epidural analgesia, forced mobilization, and oral nutrition—reduces hormonal and metabolic stress and improves convalescence after major urologic surgery. Anesth Analg. 2001;92(6):1594–600.
Sakashita R, Nishitani M, Ono H, Sato T and Hamada M. Impact of the consistency of food substances on the aspiration pneumonia of residents in welfare facilities for seniors. In: The 5th international symposium for inter oral health science, Sendai. 2014.
Tenovuo J. Antimicrobial function of human saliva–how important is it for oral health? Acta Odontol Scand. 1998;56(5):250–6.
Kaplan MD, Baum BJ. The functions of saliva. Dysphagia. 1993;8(3):225–9.
Palmer LB, Albulak K, Fields S, et al. Oral clearance and pathogenic oropharyngeal colonization in the elderly. Am J Respir Crit Care Med. 2001;164:464–8.
Leier H. Does gum chewing help prevent impaired gastric motility in the postoperative period? J Am Acad Nurse Pract. 2007;19(3):133–6.
Sakashita R, Inoue N, Kamegai T. From milk to solids: a reference standard for the transitional eating process in infants and preschool children in Japan. Eur J Clin Nutr. 2004;58(4):643–53.
Ono Y, Yamamoto T, Kubo KY, et al. Occlusion and brain function: mastication as a prevention of cognitive dysfunction. J Oral Rehabil. 2010;37:624–40.
Weijenberg RAF, Scherder EJA, Lobbezoo F. Mastication for the mind: the relationship between mastication and cognition in ageing and dementia. Neurosci Biobehav Rev. 2011;35:483–97.
Lexomboon D, Trulsson M, Wårdh I, Parker MG. Chewing ability and tooth loss: association with cognitive impairment in an elderly population study. J Am Geriatr Soc. 2012;60(10):1951–6.
Stewart L. Development of the nutrition and swallowing checklist, a screening tool for nutrition risk and swallowing risk in people with intellectual disability. J Intellect Dev Disabil. 2003;28(2):171–87.
Wright L, Cotter D, Hickson M, Frost G. Comparison of energy and protein intakes of older people consuming a texture modified diet with a normal hospital diet. J Hum Nutr Diet. 2005;18(3):213–9.
Dahl WJ, Whiting SJ, Tyler RT. Protein content for pureed diets: implications for planning. Can J Diet Pract Res. 2007;68(2):99–102.
Beck AM, Hansen KS. Meals served in Danish nursing homes and to Meals-On-Wheels clients may not offer nutritionally adequate choices. J Nutr Elder. 2010;29(1):100–9.
Easterling CS, Robbins E. Dementia and dysphagia. Geriatr Nurs. 2008;29(4):275–85.
Ekberg O, Handy S, Woisard V, Wuttge-Hannig A, Ortega P. Social and psychological burden of dysphagia: its impact on diagnosis and treatment. Dysphagia. 2002;17:139–46.
Yamaki N, Shirasaka T, Sato M, Ichimura K. Effects of the introduction of soft food on the nutrition, food intake and swallowing ability of elderly residents of a nursing care home. J Jpn Acad Gerontological Nurs. 2012;17(1):83–90 (in Japanese).
Stodel EJ, Chambers LW. Assessing satisfaction with care in LTC homes: current and best practices. Healthc Manage Forum. 2006;19(3):45–52.
Wright L, Cotter D, Hickson M, Frost G. Comparison of energy and protein intakes of older people consuming a texture modified diet with a normal hospital diet. J Hum Nutr Diet. 2005;18(3):213–9.
Kumlien S, Axelsson K. Stroke patients in nursing homes: eating, feeding, nutrition and related care. J Clin Nurs. 2002;11(4):498–509.
Niezgoda H, Miville A, Chambers LW, Keller HH. Issues and challenges of modified-texture foods in long-term care: a workshop report. Ann Long Term Care. 2012;20(7):22–7.
Groher ME, McKaig TN. Dysphagia and dietary levels in skilled nursing facilities. J Am Geriatr Soc. 1995;43:528–32.
Krall E, Hayes C, et al. How dentition status and masticatory - Function affect nutrient intake. J Am Dent Assoc. 1998;129(9):1261–9.
Sheiham A, Steele JG, et al. The relationship among dental status, nutrient intake, and nutritional status in older people. J Dent Res. 2001;80(2):408–13.
Evidence-Based Medicine Working Group. Evidence-based medicine: a new approach to teaching the practice of medicine. JAMA. 1992;268(17):2420–5.
Black N. Why we need observational studies to evaluate the effectiveness of health care. BMJ. 1996;312(7040):1215–8.
Benson K, Hartz AJ. A comparison of observational studies and randomized, controlled trials. N Engl J Med. 2000;342(25):1878–86.
Concato J, Shah N, Horwitz RI. Randomized, controlled trials, observational studies, and the hierarchy of research designs. N Engl J Med. 2000;342(25):1887–92.
Horn SD, Gassaway J. Practice-based evidence study design for comparative effectiveness research. Med Care. 2007;45(10 Supl 2):S50–7.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is distributed under the terms of the Creative Commons Attribution Noncommercial License, which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Copyright information
© 2015 The Author(s)
About this paper
Cite this paper
Sakashita, R., Takami, M., Ono, H., Nishihira, T., Sato, T., Hamada, M. (2015). Preventing Aspiration Pneumonia Among the Elderly: A Review Focused on the Impact of the Consistency of Food Substances. In: Sasaki, K., Suzuki, O., Takahashi, N. (eds) Interface Oral Health Science 2014. Springer, Tokyo. https://doi.org/10.1007/978-4-431-55192-8_29
Download citation
DOI: https://doi.org/10.1007/978-4-431-55192-8_29
Published:
Publisher Name: Springer, Tokyo
Print ISBN: 978-4-431-55125-6
Online ISBN: 978-4-431-55192-8
eBook Packages: MedicineMedicine (R0)