
Abstract
The descending perineum syndrome represents a complex clinical condition characterized by excessive pelvic floor relaxation occurring during straining or visible already at rest. It is characterized by a varied set of signs and symptoms ranging from obstructed defecation to fecal incontinence, according to the stage of the disorder. Perineal descent is thought to be involved in a vicious cycle that, starting from excessive straining and passing through pelvic floor weakness, leads to exacerbation of rectal anatomical abnormalities, perineal ballooning and worsening of constipation. As a result of this impaired defecation, chronic, excessive and repetitive straining may occur, which over time leads to weakening of the pelvic floor musculature and sagging of the perineum. In the late stage of the disorder, perineal descent tends to be associated with anatomical and functional alterations predisposing to fecal incontinence such as high-grade pelvic organ prolapse and specifically rectal prolapse, increased anorectal angle with decreased levator ani tone, decreased anal resting pressure and amplitude and duration of maximal voluntary contraction, and thinning of the external anal sphincter. The combination of these alterations and their possible association with sphincter defects and advanced age may contribute to cause fecal incontinence in patients with excessive perineal descent.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
The descending perineum syndrome represents a complex clinical condition characterized by excessive pelvic floor relaxation occurring during straining or visible already at rest.
The recognition and definition of this syndrome is quite recent. A perineal bulging on straining was first illustrated by Porter in 1962 [1], whereas perineal descent was first included in the context of a distinct pathological entity by Parks in 1966 who used the definition “descending perineum syndrome” as a descriptive term, since perineal descent clearly represents both the main objective finding and the cause of the symptomatology [2, 3].
This syndrome may be associated with pelvic organ prolapse, rectal intussusception, perineal hernias, solitary rectal ulcer syndrome and pudendal neuropathy and is characterized by various signs and symptoms ranging from obstructed defecation to anal incontinence, according to the stage of the disorder. In particular, it is estimated that perineal descent may be recognizable in 75–84% of constipated patients and in at least 75% of incontinent patients, with an increasing prevalence in women and the elderly [4,5,6,7].
2 Definition and Diagnosis
Although perineal descent may be observed at physical examination in the Sims or lithotomy position and measured in the outpatients’ clinic by the POP-Q system and the St. Mark’s perineometer [8], a more accurate measurement—and consequently the most widely accepted definition of this condition—is based on the resting and straining phases of cinedefecography [5] (Fig. 22.1).

Perineal descent observed at physical examination in the Sims position. At rest (left) and during bearing down (right)
Radiologically, perineal descent is measured along a perpendicular line drawn from the pubococcygeal line (corresponding to levator plane) to the anorectal angle (Fig. 22.2). A >3 cm descent of the anorectal angle from the levator plane at rest and a >3 cm descent of the anorectal angle from the resting position during straining are generally considered pathological values and represent the most common definitions for “fixed” and “dynamic” perineal descent, respectively [9,10,11,12,13].

Resting and straining phases observed at cinedefecography. P pubis, C tip of the coccyx, PL puborectal muscle line, RA rectal axis, ACA anal canal axis, A anorectal angle, PD perineal descent
Alternatively, dynamic magnetic resonance imaging represents an excellent tool for detecting perineal descent and simultaneously depicting the complex anatomy of the pelvic floor, with accurate identification of the supportive elements, the prolapse and the functional abnormalities of pelvic organs. Moreover, compared with cinedefecography, the theoretical disadvantage of the supine position does not seem to significantly affect identification of the dynamic descending perineum [12, 13] (Fig. 22.3).

Resting and straining phases observed with dynamic magnetic resonance imaging. PD perineal descent
3 Pathophysiology
As first described by Parks [1], the descending perineum is thought to be involved in a vicious cycle that, starting from excessive straining and passing through pelvic floor weakness, leads to exacerbation of rectal anatomical abnormalities, perineal ballooning and worsening of constipation. In particular, the event triggering the vicious cycle could be a primary difficult rectal emptying due to still not well-known causes and possibly related to dyssynergic defecation or anatomical rectal abnormalities (e.g., intussusception and/or rectocele) [14]. As a result of this impaired defecation, chronic, excessive and repetitive straining may occur, causing weakening of the pelvic floor musculature and sagging of the perineum over time [1].
Overall, the risk factors for increased perineal descent seem to be related to female gender, pregnancy, vaginal delivery, age, rectocele size, and rectal intussusception [4].
The weakened pelvic anatomical structures involved in perineal descent are several and include the levator ani muscles (that tend to stretch and weaken at the level of the urogenital hiatus and to assume a bowl-like configuration) [15], the complex network of pelvic organ ligaments (that tend to overstretch and weaken) [16] and the muscular fibers of the perineal membrane [17].
In particular, in normal subjects an important role in limiting excessive perineal descent would seem to be played by the functional activity of the superficial and deep transverse perineal muscles. As shown by electrophysiological studies, these muscles, differently from the levator ani, contract during defecation, supporting the perineal floor and protecting the perineum against the high pressure produced by straining, which, if excessive and repetitive, may cause weakness, subluxation, and sagging of the perineal muscles, resulting in perineocele [18, 19]. Moreover, as demonstrated by anatomical studies [17], in the presence of an increased force directed caudally, these muscle fibers become tight and consequently resist further perineal displacement. In the same way, transection of these fibers in the cadaver leaves the rectum exposed and allows the distal rectum to prolapse downward.
In summary, in the presence of risk factors and, likely, congenital predisposition, a chronic and repetitive impaired defecation can cause excessive descent of the perineum. In an early stage, the perineum appears mobile (dynamic), when the normally positioned pelvic floor at rest descends >3 cm during straining and returns to normal position after evacuation. Subsequently, in a later stage, the perineum becomes fixed, when a descent >3 cm occurs already at rest.
The last step of the vicious cycle is represented by the worsening of obstructed defecation and of the initial rectal alteration induced by descending perineum. The interaction between constipation and perineal descent is probably sustained by abdominal straining during defecation. As is known, a satisfactory rectal emptying is finally obtained with simultaneous relaxation of the puborectalis/external sphincter muscles and an increase in intrabdominal pressure induced by abdominal straining. In particular, during this maneuver, flattening of the diaphragm downwards into the abdominal cavity and contraction of the abdominal muscles reduce, in patients without excessive perineal descent, the abdominal cavity volume; this, in consideration of Laplace’s law, contributes to determine the increased abdominal pressure necessary for defecation. In patients with a pathological perineal descent, straining probably can induce a change in shape of the lower abdominal cavity without achieving a reduction of the abdominal volume. Thus, in this condition, the expected increase in intrabdominal and intrarectal pressure, cannot be obtained.
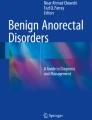
In the late stage of the disorder, mainly when a fixed descending perineum becomes evident due to advanced anatomical derangement of the pelvic floor, the perineal descent tends to be associated with anatomical and functional alterations predisposing to fecal incontinence, such as high-grade pelvic organ prolapse and specifically rectal prolapse, increased anorectal angle with decreased levator ani tone, decreased anal resting pressure and amplitude and duration of maximal voluntary contraction, and thinning of the external anal sphincter [20] (Fig. 22.4). The combination of these alterations, and their possible association with sphincter defects and advanced age may contribute to cause fecal incontinence in patients with a long history of impaired defecation and excessive perineal descent.

Late stage of perineal descent syndrome with multiorgan and multilevel pelvic prolapse observed with dynamic magnetic resonance imaging, at rest (left) and during bearing down (right). SB small bowel, B bladder, V vagina, R rectum, P pubis, C coccyx
According to this multifactorial pathogenesis, the clinical forms of incontinence in this group of patients may be various and include urge incontinence in about 56% of patients, passive incontinence in about 20%, mixed incontinence in about 16% and post-defecatory incontinence in about 4% [20].
A theoretical sequela of perineal descent is pudendal neuropathy since chronic straining may be associated with nerve entrapment and/or stretching, resulting in up to 20% increase in nerve length, sufficient to cause neuropathy [4]. The pudendal nerve injury secondary to pelvic floor descent could lead to sphincter denervation and contribute to the onset of anal incontinence [5]. However, despite these reasonable considerations, the theory of pudendal nerve strain leading to anal incontinence is strongly questioned by the conflicting results in the relationship between increased pudendal nerve motor latency values and increased perineal descent [21, 22].
4 Principles of Treatment
Therapy should be tailored on stage of the disorder, predominant symptoms, coexistence of pelvic organ prolapse and, in the latter case, on which pelvic support structures have primarily failed, according to DeLancey’s levels [16, 17].
In the first stage of the syndrome, conservative measures (high fiber diet, laxatives, suppositories, enema) associated with biofeedback and kinesitherapy have been advocated. In patients nonresponsive to medical treatment, surgery could represent a further therapeutic option.
Surgical treatment should aim to correct the overall pelvic floor alterations, including both rectal and genital prolapse (associated with a deficit of support levels I and II) and perineal descent (associated with a deficit of support level III).
The surgical options for correction of pelvic organ prolapse can be distinguished into suspensive (e.g., pelvic organ prolapse suspension surgery, Dubuisson, ventral rectopexy, colposacropexy), resective (e.g., stapled transanal rectal resection, Delorme, Altemeier), or mixed.
The surgical techniques proposed to correct perineal descent are limited and are mainly represented by levatorplasty, levator plate myorraphy and transverse perineal support [23]. The last of these involves positioning of a mesh implant just above the perineum superficial fascia, sutured to the periosteum membrane of the two branches of the pubis, with the rationale of mimicking the role of superficial transverse perineal muscle and the aim of creating a support element for the pelvic floor. Concerning effectiveness, good preliminary short-term results were reported [23], even if other studies with larger sample size and longer follow-up are needed to confirm these data (Fig. 22.5).

Transverse perineal support procedure. (a) After the finger identification of the ischial tuberosities, the overlying skin is incised for 2 cm on each side. (b) Two stitches in nonabsorbable material and spaced 1 cm apart are affixed bilaterally to the periosteum membrane of the ascending branches of the pubis at the insertion of the superficial transverse perineal muscle. (c) A blunt dissection of the adipose tissue from the perineum superficial fascia, upward to create a tunnel between the two branches of the pubis, is carried out, and forceps are passed through the tunnel. (d) A porcine dermal implant (Permacol-Medtronic; size = 4 × 18 cm), tapered previously in the middle third, is positioned just above the perineum superficial fascia. (e) The implant is sutured to the periosteum membrane and the excess is trimmed away. (f) The skin incisions are eventually sutured
References
Porter NH. A physiological study of the pelvic floor in rectal prolapse. Ann R Coll Surg Engl. 1962;31(6):379–404.
Parks AG, Porter NH, Hardcastle J. The syndrome of the descending perineum. Proc R Soc Med. 1966;59(6):477–82.
Hardcastle JD. The descending perineum syndrome. Practitioner. 1969;203(217):612–9.
Chaudhry Z, Tarnay C. Descending perineum syndrome: a review of the presentation, diagnosis, and management. Int Urogynecol J. 2016;27(8):1149–56.
Timmke AE. Functional anorectal disorders. In: Beck DE, Wexner SD, editors. Fundamentals of anorectal surgery. London: WB Saunders; 1998. p. 90–8.
Read NW, Bannister JJ. Anorectal manometry: techniques in health and anorectal disease. In: Henry MM, Swash M, editors. Coloproctology and pelvic floor. London: Butterworth-Heinemann; 1985. p. 65–87.
Renzi A, Izzo D, Di Sarno G, et al. Cinedefecographic findings in patients with obstructed defecation syndrome. A study in 420 cases. Minerva Chir. 2006;61(6):493–9.
Henry MM, Parks AG, Swash M. The pelvic floor musculature in the descending perineum syndrome. Br J Surg. 1982;69(8):470–2.
Shorvon PJ, McHugh S, Diamant NE, et al. Defecography in normal volunteers: results and implications. Gut. 1989;30(12):1737–49.
Shorvon PJ, Stevenson GW. Defaecography: setting up a service. Br J Hosp Med. 1989;41(5):460–6.
Oettle GJ, Roe AM, Bartolo DC, Mortensen NJ. What is the best way of measuring perineal descent? A comparison of radiographic and clinical methods. Br J Surg. 1985;72(12):999–1001.
Iacobellis F, Reginelli A, Berritto D, et al. Pelvic floor dysfunctions: how to image patients? Jpn J Radiol. 2020;38(1):47–63.
Iacobellis F, Brillantino A, Renzi A, et al. MR imaging in diagnosis of pelvic floor descent: supine versus sitting position. Gastroenterol Res Pract. 2016;2016:6594152. https://doi.org/10.1155/2016/6594152.
Pucciani F. Descending perineum syndrome: new perspectives. Tech Coloproctol. 2015;19(8):443–8.
Singh K, Jakab M, Reid WM, et al. Three-dimensional magnetic resonance imaging assessment of levator ani morphologic features in different grades of prolapse. Am J Obstet Gynecol. 2003;188(4):910–5.
DeLancey JO. Anatomic aspects of vaginal eversion after hysterectomy. Am J Obstet Gynecol. 1992;166(6 Pt 1):1717–24; discussion 1724–8.
DeLancey JO. Structural anatomy of the posterior pelvic compartment as it relates to rectocele. Am J Obstet Gynecol. 1999;180(4):815–23.
Shafik A, Ahmed I, Shafik AA, et al. Surgical anatomy of the perineal muscles and their role in perineal disorders. Anat Sci Int. 2005;80(3):167–71.
Shafik A, Shafik AA, Shafik I, El-Sibai O. Study of the role of the transverse perineal muscles during rectal filling. Int J Colorectal Dis. 2006;21(7):698–704.
Pucciani F. Descending perineum syndrome: pathophysiology of fecal incontinence. Pelviperineology. 2018;37:57–62.
Jones PN, Lubowski DZ, Swash M, Henry MM. Relation between perineal descent and pudendal nerve damage in idiopathic faecal incontinence. Int J Colorectal Dis. 1987;2(2):93–5.
Ho YH, Goh HS. The neurophysiological significance of perineal descent. Int J Colorectal Dis. 1995;10(2):107–11.
Renzi A, Brillantino A, Di Sarno G, et al. Transverse perineal support: a novel surgical treatment for perineal descent in patients with obstructed defecation syndrome. Dis Colon Rectum. 2016;59(6):557–64.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (http://creativecommons.org/licenses/by-nc-nd/4.0/), which permits any noncommercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if you modified the licensed material. You do not have permission under this license to share adapted material derived from this chapter or parts of it.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2023 The Author(s)
About this chapter

Cite this chapter
Renzi, A., Brillantino, A. (2023). Perineal Descent and Incontinence. In: Docimo, L., Brusciano, L. (eds) Anal Incontinence. Updates in Surgery. Springer, Cham. https://doi.org/10.1007/978-3-031-08392-1_22
Download citation
DOI: https://doi.org/10.1007/978-3-031-08392-1_22
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-08391-4
Online ISBN: 978-3-031-08392-1
eBook Packages: MedicineMedicine (R0)