
Abstract
We aim to restore the kinematics of the knee in unicompartmental arthroplasty as it was being used by that individual before the arthrosis developed. The knee is used in compression when standing and squatting and in swing phase, where a competent anterior and posterior cruciate ligament complex allows efficient and congruent flexion after toe off, followed by extension leading to heel strike. This combination of ligament tension and joint congruence is the key to a natural and efficient gait at varying speeds and gradients. Following UKA, which restores both stability and congruence, this state can be approached, but it is very hard to achieve following TKA which inevitably involves ACL sacrifice [1].
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


We aim to restore the kinematics of the knee in unicompartmental arthroplasty as it was being used by that individual before the arthrosis developed. The knee is used in compression when standing and squatting and in swing phase, where a competent anterior and posterior cruciate ligament complex allows efficient and congruent flexion after toe off, followed by extension leading to heel strike. This combination of ligament tension and joint congruence is the key to a natural and efficient gait at varying speeds and gradients. Following UKA, which restores both stability and congruence, this state can be approached, but it is very hard to achieve following TKA which inevitably involves ACL sacrifice [1].
However, human gait is not a single phenomenon—the varus knee is part of a human whose whole body movement differs substantially from a human with a valgus knee. Typically, the medial compartment of a varus knee can be considered fairly monodimensionally, in a horizontal coronal axis, while the lateral compartment of a valgus knee needs to rotate around both a coronal and a longitudinal axis. So any partial knee replacement must respect the way in which the knee was used and indeed wore out, correcting slightly, but importantly not trying to ‘restore’ a mechanical alignment that was never there.
1 Indications for Medial UKA (MUKA)
Pain is the dominant indication for MUKA, felt medially or anteromedially. Overloading the medial compartment results in arthrosis in the varus knee, causing painful overload of the bone surfaces. Pain may also be felt laterally, from soft-tissue tension. The pattern of pain is typical of arthrosis—start up pain, stiffness, swelling and loss of function.
The examination findings are also typical, with bone on bone articulation medially or anteromedially. Very strong data exists for the use of MUKA in this condition. Earlier intervention, performing a UKA after meniscal failure but before the onset of established arthrosis is more controversial, with poorer outcomes. The subchondral sclerosis that accompanies established arthrosis is a good substrate for osseomechanical integration of the tibial component. In earlier interventions, before this reactive bone formation is established, there is a higher risk of tibial component loosening or migration. Importantly, there is a stable lateral meniscus. This can be demonstrated, by feeling for any meniscal extrusion on valgus stressing. A stable cruciate complex or central pivot must also be demonstrated using anteroposterior stressing with any varus deformity corrected into neutral.
Medial patella-femoral joint pain can be safely ignored, in a varus knee, as it is relieved by the correction of varus with MUKA [2]. Gross arthrosis of the patella-femoral joint should be addressed separately [3].
Indications for Lateral UKA (LUKA)
Pain is the dominant indication for LUKA, but the lateral compartment is loaded less than the medial compartment in extension, so pain is often less of a feature, with loss of function, and difficulty on stairs being a dominant feature. The pain is felt usually laterally, but often there is tension pain medially. Lateral arthrosis can be felt in the hip area, quite commonly reported either around the greater trochanter or buttock. This completely resolves following LUKA, but of course hip arthrosis can be felt in the knee, so the hip should be X-rayed as well as examined in these circumstances.
The examination findings include a knee that becomes progressively valgus on flexion and easily corrects towards neutral. On stressing the knee in varus, the medial meniscus should not extrude, and the cruciate complex should be stable to anteroposterior stressing. Once again, the patella-femoral joint can be ignored if the symptoms and signs are minor and laterally based [4].
2 Threshold for UKA vs. Osteotomy
Most surgeons would hesitate to proceed to knee arthroplasty in patients who want to run. In those who have bone on bone articulation on either the standing AP or Rosenberg views, in my hands the function of a UKA is more reliable than an HTO, which is borne out by one randomised trial [5] and clinical experience [6].
Threshold for UKA vs. Bi-UKA vs. TKA
In active people, who have medial arthrosis but also have an extruding lateral meniscus, a MUKA alone may not be sufficient. Knees like this may progress on the lateral side especially in the obese and in those who are not obviously varus. Currently a TKA is one option, while the more conservative option of a bi-UKA should be considered if the ACL/PCL complex is intact [7]. This bi-UKA is worth discussing in two groups, the young and active, who are likely to break up a TKA; the old and frail patient is another group for whom a bi-UKA may be attractive, as it is a very small operation, much less likely to result in systemic upset.
Device Choice: Mobile or Fixed
UKA is demonstrated to work very well indeed with either mobile [8] or fixed [9] bearings. Medium-term studies do not show major differences, so the choice will be more related to the surgeon and the patient in their regulatory environment. In my personal practice, I advise mobile bearings for those who are likely to wear out a fixed bearing, on both sides.
Fixation Method
Fixation using cement in partial knee replacement has good long-term outcomes in the fixed bearing devices. Cementless fixation is now well established in the mobile bearing implants [10]. In my personal experience, cementless mobile bearing devices have a very low rate of loosening, so they have significant attraction. The only issue in this regard is that of early periprosthetic fracture.
Anterior Cruciate Deficiency
In older or lower demand patients who have no symptoms of instability, a UKA can also be used in the absence of an ACL [11]. Typically in older patients, stiffness is common, while instability is an unusual symptom. So as long as the knee is left in varus, the lateral compartment is unlikely to deteriorate, and the lack of ACL is seldom a problem.
3 Surgical Planning
Prior to surgery, the very minimum planning needed is an appreciation of the size of device required, confirming that neither the tibial plateau nor femoral condyle is too small or too big for the available device’s range. From plain radiographs, the standing AP, schuss and lateral view will help in appreciating the amount of tibia vara and intra-articular bone loss. The amount of varus needed on the tibial cut can be envisaged and the depth of bone to be resected, to ensure the minimum thickness of bearing can be accommodated, while at the same time ensuring that the prosthesis is sited on the hardest subchondral bone possible.
Posterior slope of the tibial component and flexion of the femoral component can also be planned from the lateral plain radiographs to a significant extent. For smaller people from the subcontinent, in particular, a higher posterior slope is common and worth preserving to ensure even soft tissue tension. An absent or injured ACL may be better managed by reducing the posterior slope—some anterior tibial translation on the lateral view may confirm the clinical impression.
The last element of surgical planning is device specific. Depending on the design characteristics of the interface, varus slope of the tibial component must be matched with coronal plane and axial plane rotation of the femoral component. A spherical femoral component, on a wholly congruent meniscal bearing, will not need any adjustment from neutral, while a cam-type femoral component may need to be rotated in the coronal plane by a few degrees to ensure linear rather than point contact.
All these elements can be better addressed using 3D planning based upon either MRI or CT. The attraction of what appears to be an increase in complexity is that it allows almost all variables to be documented preoperatively, reducing the intraoperative procedure to a checklist, confirming the preoperative measurements. The best example of this is the tibial ‘biscuit’ which can be 3D printed and sterilised. The exact shape and size of the bone resection can then be compared with the plan, confirming that the resection is adequate in all dimensions.
4 Component Alignment
Kinematic alignment (KA) is a personalized technique for implanting knee components. The principles are to anatomically position (true resurfacing) and kinematically align (on the cylindrical femoral axis) the components, in order to restore the native articular surface level and orientation and improve prosthetic interaction (or biomechanics).
Interestingly, the Philippe Cartier’s principles for implanting UKA components were consistent with those promoted by the KA technique but differently formulated (Fig. 18.1). In contrast, the mechanical alignment technique aims to systematically orientate the knee components (standardised implantation), relative to the long bone (femur and tibia) mechanical axes, thus neglecting individual medial knee compartment anatomy but thought to be beneficial for reliable implantation. The non-anatomic mobile bearing UKA Oxford® components have historically been recommended to be mechanically implanted while still reproducing the constitutional limb alignment (or hip-knee-ankle angle). The Oxford® femoral component is therefore oriented in the coronal plane parallel to the femoral mechanical axis; the tibial component is frontally positioned perpendicular to the tibia mechanical axis and with a 7° posterior slope. Personalizing the Oxford® components’ orientation by performing kinematic alignment would reproduce the medial knee compartment anatomy and potentially be clinically advantageous by preserving tibia bone stock and by optimising the interactions between bone and prosthesis (more physiological loading of the supportive bone) and between bearing surfaces. It is therefore the authors’ preference to perform kinematic implantation of UKA, regardless of whether the bearing is fixed or mobile (Fig. 18.2).

Anteroposterior radiographs of a left knee before (a) and after (b) kinematic implantation of a fixed bearing medial UKA. The component alignment aims to reproduce the native orientation of articular surfaces (Image courtesy of Deschamps et al. [15])

Preoperative (a) and postoperative frontal (b) and lateral (c) radiographic views of a left knee implanted with a kinematically aligned mobile bearing Oxford® medial UKA. Intraoperative photos illustrating a good interaction between components in extension (d) and in flexion (e)
5 Technical Considerations
The patient can be set up in either the supine ‘TKA’ position or the ‘dangle’. Both work well. The main reason for supine surgery is to allow conversion to TKA or if the addition of patella-femoral arthroplasty has been planned. The use of a tourniquet is not compulsory and is not needed if cementless fixation is planned but may help if cement is needed. Because the procedure should not last long, a tourniquet has few complications.
6 Medial
Following exposure and thorough clearance of osteophytes in the notch, the knee should extend well. Full flexion may not be possible until posterior osteophytes are removed, but flexion to 110° should now be easy, with gentle flexion beyond gravity alone. With the knee in 30° of flexion and with retractors in situ, there is no tension in the soft tissues, and the surgeon can confirm the amount of material lost to arthrosis. This will confirm the amount of bone that still needs to be resected, to ensure that only the minimum of bone is removed, and the orientation of the bone cut needed to reproduce the ‘Cartier angle’.
Each degree of freedom should be addressed serially.
-
1.
The tibia varus angle: this will have been chosen preoperatively but checked visually. Angle of 3° to 5° for the varus knee and of 1° to 3° for the valgus knee are approximately the respective populations mean values. A neutral or valgus metaphyseal angle is rare, and with UKA, it may increase the risk of tibial subsidence, by cutting into bone in the middle of the tibia that is markedly less stiff than the rest of the bone interface.
-
2.
The posterior slope: this is device and patient specific. The surgeon’s aim is to restore the joint line unless the slope is being reduced to compensate for some cruciate insufficiency.
-
3.
Axial rotation: a precise definition of the front of the knee is hard. The flexion axis of the knee is fairly reliable and should be used for the first cut (sagittal cut).
-
4.
Depth of resection: this should be minimal, based upon the amount of bone damage and the device minimum thickness.
-
5.
Medial translation: the sagittal cut should be far up the tibial spine. This may not be possible without some osteophyte trimming of the condyle and retraction of both fat pad and patella. Some extension of the knee may help at this stage.
The tibial bony ‘biscuit’ is removed and then checked for depth and shape. Based upon its shape, adjustment may be needed. Commonly, the axial rotation may be adjusted, and a more lateral sagittal cut may be performed. The posterior slope should be noted.
The femur is then addressed with the tibial trial prosthesis in place. The knee will by now have a free range of motion between full extension and 100° of flexion. This is needed for femoral preparation. The femoral jigs are placed upon the knee, to ensure that adequate bone is removed in flexion. In medial arthrosis, the flexion gap is always preserved, so it is used as a datum point for ensuring that the flexion axis is restored without tension.
The alignment of the flexion gap is chosen based upon the preoperative analysis and plan including the device choice. Slight coronal plane rotation of the cutting block may be needed, if a fixed bearing device is used, to ensure that the bearing surface is congruent with the tibia. The extension gap is then assessed and compared with the expected gap on the plan. In medial arthrosis, it is always greater than the flexion gap, owing to material loss, while following surgery, the opposite will be the case: the flexion gap will be 1 mm greater than the extension gap, as it is in nature. Once again, subtle rotation and translation of the cutting block may be needed if a fixed bearing device is used, while for a mobile bearing, a neutral alignment is sufficient.
Two common errors occur with femoral block positioning: positioning the femoral block too medially if pushed outwards by a large patella in a large man and failing to flex the knee sufficiently when cutting the flexion gap. Too medial positioning of the femoral component may cause soft tissue impingement, while if the flexion gap is cut at less than 95°, the balance between the flexion and extension gaps will become problematic.
Fine-tuning of the balance between flexion and extension gaps can be achieved in several ways. Ideally, in full extension, the entire knee is snug, with just a single millimetre of play both in varus and valgus. By rocking the knee into valgus and varus, some laxity is felt, even in full extension. It is usually less than 1 mm. When balancing a medial uni, the medial compartment should feel snug in full extension. Checks should be made for any bony impingement in the notch—osteophytes on both tibial and femoral side may cause a block to full pain-free extension. In flexion, there should be no block to further flexion caused by the height of the tibial component. Preoperative analysis and planning will have revealed the presence of posterior osteophytes which may also need to be removed from the femoral condyle to enable full, impingement-free flexion.
7 Lateral
The surgical approach to the lateral compartment is broadly similar to the medial but differs in a few important ways.
After exposure and removal of meniscus anteriorly, a thorough osteophytectomy is performed, ensuring that the notch is clear and that any patella and trochlea osteophytes are also removed, so that full extension and flexion are possible.
The knee is then flexed and placed in ‘figure-of-4’ position. The tibial surface can be seen well in this position, and the tibial cutting block can then be attached. As with the medial side, tibial resection needs to be sufficient to restore the joint line with the minimal thickness of tibial component, to ensure that the strongest subchondral bone is preserved. The bone cut is made at the right orientation for the individual patient, usually in 1° or 2° of varus (mean tibial metaphyseal angle for valgus knees). The tibial ‘biscuit’ is then removed and inspected. On the lateral side, the common error is to leave the sagittal cut too lateral, pushed that way by the patella tendon and fat pad. By leaving the knee in figure of 4, and extending the knee to 45°, the tension is taken off the extensor mechanism, allowing the surgeon to sublux the patella medially and gain sagittal access.
When undertaking lateral UKA, the wear scar is greatest in the flexion facet, while the distal extension facet may still have full-thickness cartilage, so care must be taken to reduce the extension height sufficiently to ensure full extension without any medial tension. When the knee is rocked into varus in flexion, there should be at least 2 mm more gap than in extension, but in addition, at least 1 mm of opening should be possible in full extension, with no conflict between the edges of the components either in deep flexion or extension. With some ranges of devices, a long-standing valgus knee maybe wider than the range, so the sagittal cut may be more lateral, enabling the tibial component to be placed under the femur.
8 Postoperative Care and Outcome Measures
Following conservative arthroplasty of any sort, the postoperative course is not magical: the bone of the tibia, in particular, has to heal, and by leaving the varus knee in slight varus, the load across this interface can be critical. So weight bearing should be gradual and limited by pain. Because the cruciates are intact, joint kinematics are preserved, so the risk of requiring a manipulation under anaesthetic for inadequate range of motion is very small indeed, and no pressure is needed to encourage early range of motion. Physiotherapists will naturally encourage faster rehabilitation, but this is not advisable. The use of a walking aid for the first 3–4 weeks is mandatory.
Metrics of outcome for UKA are quite different from TKA. We recommend two different types of metric: one personal and one physical. The personal metric should revolve around one or two activities that the patient enjoys or used to enjoy. Use these as determinants of outcome. The web-based tool, www.jointpro.co.uk, is a simple way for a surgeon and patient to communicate how well those desired outcomes have been met or exceeded.
The physical dimension can be recorded using a variety of tools. Several pieces of software available for use on smart phones allow monitoring of the time taken for a known circuit, together with top speed, average speed, etc. Alternatively, a treadmill can be used, and measurements of top walking speed, cadence and stride length can be recorded as a measure of progress. Finally, the width of gait, and its consistency, is a sensitive measure, showing the extent to which a patient has returned towards normal. A healthy adult with normal strength and balance has quite a narrow gait, with little variation between steps. With increasing infirmity, the width of the gait increases as does the variability between steps. Preservation of the native joint line and cruciate ligaments enables the patient to retain these normal gait characteristics. This is hard following total joint replacement. These variables are more difficult to record without specialist equipment.
All these physical variables continue to improve postoperatively for at least 12 months, although more than 85% is achieved within 6 months.
9 Complications and Their Management
A well-performed, kinematically aligned UKA will seldom fail, but the ‘reoperation rate’ may well be higher than following total joint replacement for two reasons. First, because the knee feels normal, people do more and so are more prone to further mechanical events, so the lateral meniscus may fail 1 day if someone goes back to the tennis court or the gym. Secondly, it is easy to perform further surgery on a knee with a UKA, so small adjustments are possible. We also now know that they are successful at restoring function, often without the need for a total knee replacement. The last 100 s operations by my group included several causes of second surgery.
9.1 Bearing Wear or Fracture
Should a bearing wear out after more than a decade of high performance life, then this should be considered a success—the patient has clearly been having a great time! In this circumstance, a simple bearing change is all that is needed to restore function, and in all probability, there will be no need for a second bearing change as the patient will be that much older.
9.2 Bearing Dislocation
This is usually the consequence of excessive laxity or technical error. In either event, correct the error and consider revising the tibial component to a fixed bearing. The procedure is easy, and the cost in functional terms and durability is small, while second dislocations are hard to cope with psychologically.
9.3 Progressive Wear on the Contralateral Side
Should this occur within the first 2 years, it suggests that an error in decision-making was made preoperatively, in the diagnosis, or an error was made intraoperatively, by overstuffing the affected compartment. In either event, there are two options to discuss with the patient: immediate exchange to a total knee replacement or the addition of a second UKA. This latter intervention is a much smaller insult and should be considered in the same way as one would address a primary UKA. Most importantly, are the patella-femoral joint and the central pivot healthy? For both the young, and the old and frail, a second UKA is worth considering carefully, once again being sure to leave sufficient laxity in full extension to avoid ACL strain.
9.4 Infection
Deep infection is very rare indeed, presumably because the procedure does not involve extensive dissection and there is a correspondingly smaller surface area available for biofilm to develop. Aggressive early open lavage and exchange of plastic components are recommended. Should this fail, then a single stage or a two stages conversion to a primary TKA have good rationales, with the use of a home-made cement uni making life quite manageable with walking aids during the interim for the two stages.
9.5 Tibial Periprosthetic Fracture
This is more common if a patient has been on bisphosphonates and using cementless tibial components. Risks can be minimised by ensuring that the tibial resection is appropriately varus and that only minimal thickness of tibia is resected. If pain increases during the postoperative period, early repeat X-ray and CT if in any doubt will confirm the diagnosis. A crack, if detected early, can be treated with two screws and no plate at all. If there has been subsidence, then a buttress plate may be needed. If bone grafting and a plate fail, then consider using a custom condylar replacement. This will allow you to preserve the cruciates and the rest of the knee.
9.6 Conversion to TKA
When the rest of the joint has clearly failed, my preference is to use the same arthrotomy for the TKA. I personally use kinematic alignment for the TKA, as it was proven helpful in minimising the need for augments and stems and improved patients clinical scores [12]. The procedure is not difficult, and only two technical tips need to be considered:
Kinematic tibial resection: appropriate varus angle can be measured on pre-UKA radiographs if available or on the opposite knee. Then remove the tibial component with great care, and perform an initial cut removing the implant thickness from the intact side. It may then be necessary to recut, taking 2 mm more, if no bone was removed from the medial side.
Kinematic femoral resection: by maintaining the joint line obliquity of the tibia, femoral alignment will follow kinematic guidelines. Most TKA devices will require further bone resection than the bone implant interface of a UKA, so simply apply the cutting blocks on the knee before taking the femoral component off, and complete as much of the procedure as possible before removing the device very slowly and cautiously.
9.7 Why Not Go Straight for Kinematically Aligned TKA?
While TKA is safe and effective, in older people, UKA has the great advantage of safety: the risk of major complications such as infection or a stroke is halved by undergoing the much smaller intervention of UKA [13]. In younger patients, for whom higher-level function matters a great deal, UKA enables more normal gait at higher speeds and on different gradients, restoring function to a higher level than is possible using TKA [14].
References
Wiik AV, Manning V, Strachan RK, Amis AA, Cobb JP. Unicompartmental knee arthroplasty enables near normal gait at higher speeds, unlike total knee arthroplasty. J Arthroplasty. 2013;28(9 Suppl):176–8.
Beard DJ, Pandit H, Gill HS, Hollinghurst D, Dodd CA, Murray DW. The influence of the presence and severity of pre-existing patellofemoral degenerative changes on the outcome of the Oxford medial unicompartmental knee replacement. J Bone Joint Surg Br. 2007;89(12):1597–601.
Confalonieri N, Manzotti A, Montironi F, Pullen C. Tissue sparing surgery in knee reconstruction: unicompartmental (UKA), patellofemoral (PFA), UKA + PFA, bi-unicompartmental (bi-UKA) arthroplasties. J Orthop Traumatol. 2008;9(3):171–7.
Newman SDS, Altuntas A, Alsop H, Cobb JP. Up to 10 year follow-up of the Oxford domed lateral partial knee replacement from an independent centre. Knee. 2017;24(6):1414–21.
Stukenborg-Colsman C, Wirth CJ, Lazovic D, Wefer A. High tibial osteotomy versus unicompartmental joint replacement in unicompartmental knee joint osteoarthritis: 7–10-year follow-up prospective randomised study. Knee. 2001;8(3):187–94.
Krych AJ, Reardon P, Sousa P, Pareek A, Stuart M, Pagnano M. Unicompartmental knee arthroplasty provides higher activity and durability than valgus-producing proximal tibial osteotomy at 5 to 7 years. J Bone Joint Surg Am. 2017;99(2):113–22.
Confalonieri N, Manzotti A, Cerveri P, De Momi E. Bi-unicompartmental versus total knee arthroplasty: a matched paired study with early clinical results. Arch Orthop Trauma Surg. 2009;129(9):1157–63.
Price AJ, Waite JC, Svard U. Long-term clinical results of the medial Oxford unicompartmental knee arthroplasty. Clin Orthop Relat Res. 2005;(435):171–80.
Steele RG, Hutabarat S, Evans RL, Ackroyd CE, Newman JH. Survivorship of the St Georg Sled medial unicompartmental knee replacement beyond ten years. J Bone Joint Surg Br. 2006;88(9):1164–8.
Liddle AD, Pandit H, O'Brien S, Doran E, Penny ID, Hooper GJ, et al. Cementless fixation in Oxford unicompartmental knee replacement: a multicentre study of 1000 knees. Bone Jt J. 2013;95-B(2):181–7.
Boissonneault A, Pandit H, Pegg E, Jenkins C, Gill HS, Dodd CA, et al. No difference in survivorship after unicompartmental knee arthroplasty with or without an intact anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc. 2013;21(11):2480–6.
Toliopoulos P, LeBlanc MA, Hutt J, Lavigne M, Desmeules F, Vendittoli PA. Anatomic versus mechanically aligned total knee arthroplasty for unicompartmental knee arthroplasty revision. Open Orthop J. 2016;10:357–63.
Liddle AD, Judge A, Pandit H, Murray DW. Adverse outcomes after total and unicompartmental knee replacement in 101,330 matched patients: a study of data from the National Joint Registry for England and Wales. Lancet. 2014;384(9952):1437–45.
Wiik AV, Aqil A, Tankard S, Amis AA, Cobb JP. Downhill walking gait pattern discriminates between types of knee arthroplasty: improved physiological knee functionality in UKA versus TKA. Knee Surg Sports Traumatol Arthrosc. 2015;23(6):1748–55.
Deschamps G, Chol C. Fixed-bearing unicompartmental knee arthroplasty. Patient’s selection and operative technique. Orthop Traumatol Surg Res. 2011;97:648–61.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Case Study
Case Study
Mrs. GS presented as a 53-year-old woman, 30 years after ACL reconstruction following a skiing accident. Successive surgeons had suggested TKA, which she refused completely. GS has been very active in adulthood but now completely unable to play tennis or ski.
On examination, there was a significant varus thrust on weight bearing. The gross varus corrected substantially, with a firm medial end point. With gentle valgus pressure, there was no significant AP laxity.
Radiographs confirmed Ahlback grade V arthrosis, with substantial bone loss medially, extensive osteophytes, and a normal-looking lateral compartment (Fig. 18.3).

Preoperative radiographs of a varus knee in a fit 53-year-old, 30 years post-ACL reconstruction. There is significant bone loss medially, while the lateral joint line is no longer congruent. There is extensive osteophytosis and some anterior translation of the tibia
Preoperative planning confirmed the sizes and positions of the devices and showed the large and posterior wear scar on the tibia. The excessive tibial joint line varus of 11° was planned to be reduced to 5° (Fig. 18.4).


Preoperative plans showing the size and position of the devices chosen. The tibia component was planned with (a) 5° of medial slope and (b) 8° of posterior slope. The femoral component was planned with (c) neutral frontal positioning and (d) 7° of flexion
Intraoperatively, there was still some graft present. After correcting the varus, the knee was quite stable, as predicted preoperatively.
At 2 years post-op, function has improved steadily over a 2-year period, with excellent range of motion and return to skiing and tennis (Fig. 18.5). On examination at 1 year post-op, the knee is stable, with a leg that is still 1° or 2° varus. Post-op X-rays show a varus joint line, with good correction of the deformity, and a congruent lateral compartment (Fig. 18.6).

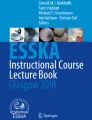
Patient-reported outcome scores from pre-op to 20 months post-op, showing the ceiling effect of the Oxford Knee Score and EQ. 5D, while the functional scores continue to improve beyond 1 year

Radiographs 1-year post-op showing that the knee is better aligned, with persisting varus limb alignment, and the planned joint line obliquity of 5°
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2020 The Author(s)
About this chapter

Cite this chapter
Cobb, J., Rivière, C. (2020). Unicompartmental Knee Arthroplasty. In: Rivière, C., Vendittoli, PA. (eds) Personalized Hip and Knee Joint Replacement. Springer, Cham. https://doi.org/10.1007/978-3-030-24243-5_18
Download citation
DOI: https://doi.org/10.1007/978-3-030-24243-5_18
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-24242-8
Online ISBN: 978-3-030-24243-5
eBook Packages: MedicineMedicine (R0)