
Abstract
Respiratory infections are the most frequent cause of athletes’ visits in medical practices. Simultaneously, contradictory beliefs are generally held regarding influence of repeated exercise on immunity reflected in susceptibility to infections. Many tend to claim that exercise weakens the immunity and renders regular exercisers more prone to develop airway infections. On the other hand, voices are heard in favor of the possible beneficial influence of regular exercise on immune system efficiency. This chapter focuses on the associations of various kinds of exercise with respiratory infection susceptibility. Influence of exercise, in particular associated with competitive performance, on selected innate and acquired immune response mechanisms is also addressed.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others

Keywords
1 General Overview
Some scientific evidence suggests that acute bouts of exercise are followed with period of increased susceptibility to respiratory infections [1,2,3,4]. Approximately, a twofold increase in prevalence of upper respiratory tract infection (URTI) symptoms after long-distance run is observed, as compared with non-runner counterparts from control groups [3, 5]. On the other hand, regular moderate physical activity is believed to contribute to greater resistance to respiratory infections. Regular exercise at moderate level is associated with reduced incidence of URTI episodes and lower intensity of infectious symptoms [6, 7]. This phenomenon has been graphically depicted as the so-called J-shaped curve which clearly shows that both sedentary lifestyle and excessive strenuous exercise constitute risk factors for increased susceptibility to respiratory infections [1] (Fig. 9.1).

“J”-shaped model of relationship between varying amounts of exercise and risk of URTI. This model suggests that moderate exercise may lower risk of respiratory infection while excessive amounts may increase the risk. Source: Nieman D. Exercise, upper respiratory tract infection, and the immune system. Med Sci Sports Exerc 1994; 26 (2): 128–39. Ref. [1]
Some reports from studies in professional athletes suggest, however, that regular high-level exercise tends to be protective with regard to URTI symptoms [8, 9]. These data may seem to question the “J-curve” model, but it is hypothesized that presence of other, not yet identified, genetic or behavioral factors might influence one’s susceptibility to infection in a high-level exercise context [10]. This modified model has been nicknamed “S-curve” [9]. One possible explanation for lower infection rate in top-level exercisers is the fact that subjects engaging in regular exercise of high intensity are predominantly those with perfect physical stamina and perfect immune health status that enable them to resist infections and carry on with training, thus permitting their inclusion to “elite” group on the basis of their achievements.
URTI usually resolve in a few days. The “check-neck rule” is commonly applied to decide whether the athletes should be stopped from training and competition (no stop for symptoms above the neck, stop in case of cough, fever, etc.). Sore throat, a frequent symptom of URTI, should alert to exclude mononucleosis and potential myocardial complications of β-hemolytic streptococci.
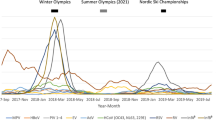
Competitive athletes frequently report URTI symptoms, but their infectious etiology cannot be confirmed in a considerable proportion of cases. Both viruses (rhinovirus, particularly in spring, influenza and parainfluenza virus, adenovirus and coronavirus) and bacteria (streptococci, staphylococci) are claimed to be involved in causing URTI in athletes, although data from large systematic studies including the isolation and identification of the responsible agents are still very limited (Table 9.1). Spence and colleagues have analyzed 37 infectious episodes in 28 competitive and noncompetitive athletes [11]. In that group, infectious etiology could be established only with regard to 11 episodes. Identified viral pathogens included rhinoviruses and adenoviruses, whereas M. pneumoniae, S. aureus, and S. pneumoniae were confirmed as bacteria causing URTI symptoms. A study by Cox et al. [12] identified viral or bacterial pathogen in 30% of athletes with upper respiratory symptoms, while 57% of all cases were accompanied either by presence of a detectable pathogen or by other laboratory pathological features of infection. Bacterial cause was found in 3% of cases only, while most frequently detected viral pathogens included rhinovirus (10%); influenza virus (10%); parainfluenza viruses 1, 2, and 3 (6%); and coronaviruses (3%). Hitherto published data indicate that pathogen identification is possible in approx. 45% of URTI symptoms in athletes [13]. A similar proportion has been also described regarding URTI symptoms in the general population [14].
2 Immunological Changes Related to Exercise
2.1 Immunoglobulins and Exercise
Decreased effectiveness of local humoral immune response at the level of the respiratory mucosae is one of the characteristic features associated with intense physical exercise. This is predominantly reflected in decreased salivary IgA (sIgA) concentrations, but the importance of other proteins contained in saliva has been recently pointed at in the context of susceptibility to upper respiratory tract infections [15]. Increased URTI susceptibility following participation in long-distance runs was observed in multiple studies [1,2,3,4,5]. Already in 1983 Peters and Bateman [3] ascertained the presence of URTI symptoms in one-third of ultramarathon participants as compared with 15% of non-running controls. Moreover, the prevalence of URTI symptoms was more prevalent in those who performed better in terms of time required to complete the run. Another study performed in runners showed, however, that those who were more committed to intensive training during preparations to long-distance run were less likely to develop infection symptoms [4]. Robson-Ansley and colleagues [5] reported a 47% prevalence of URTI symptoms over the 2-week period following participation to the London Marathon. In their study, however, a significant correlation of URTI symptoms occurred with positive IgE-mediated allergen sensitizations and atopic status, as assessed by the AQUA questionnaire designed for allergy screening in athletes [16]. The question related to the proportion of upper respiratory infection-like symptoms due to exposure to inhalant allergens and not to infection per se therefore arises. Several studies were performed in nonprofessional exercisers or sedentary subjects [6, 7] revealing that decrease in susceptibility to URTI is predominantly visible in regular exercisers who do not advance into professional, high-endurance type of training.
Shifts in salivary IgA are observed in subjects loaded with strenuous exercise associated with sports training [17,18,19,20,21,22], as well as being part of military training curriculum [23,24,25]. Decreased salivary IgA is usually correlated with increased URTI susceptibility, although this mutual association is not always evident [15]. A pioneer study by Tomasi et al. [18] comparing salivary IgA levels in cross-country skiers versus age-matched controls showed significant decreases both at baseline and after participation in a competitive run. Studies in swimmers [19, 20] also showed decreased IgA levels in saliva after training. Additionally, salivary IgA levels were inversely correlated with duration and intensity of training, as well as with number of reported infections [19]. Similarly, decreased salivary IgA was described as a risk factor for developing upper respiratory symptoms in male yacht race participants [21].
There exist, however, studies that failed to show modification of salivary IgA in response to a repeated training exercise [26, 27] pertinent to different sports disciplines. Moreover, some studies do not confirm direct association between decreased salivary IgA and frequency or severity of respiratory infections [28,29,30].This leads to assumption that influence of factors other than excessive exercise load should be taken into consideration while interpreting the data regarding salivary IgA levels. These factors include, among others, pattern of exercise, its intensity and duration, as well as the general stamina of each individual. In the case of extremely intensive training programs, provisions should be made for additional factors modifying immune response, such as increased energy consumption, sleep deprivation, altitude above sea level, and stress-associated psychological factors [15, 31,32,33].
Moderate physical activity as part of lifestyle modification plans in previously sedentary subjects leads to increase in salivary IgA levels. This fact speaks in favor of beneficial anti-inflammatory and immunomodulatory properties attributed to moderate but regular exercise [34, 35]. In young soccer players, it has been observed that salivary IgA increase considerably during a 2-week detraining period scheduled at the end of a 21-week competitive season. Increase in salivary IgA was accompanied by a significant decrease in URTI symptom score [36].
Data regarding serum immunoglobulins are contradictory. According to many authors, IgG levels in endurance athletes increase both directly after exercise and over longer observation periods [37,38,39,40]. In other studies, however, considerable falls in serum IgG were observed in association with prolonged strenuous exercise (75-kilometer run, 3-week rugby training camp participation, 2 weeks of regular running training) [41,42,43,44].
Similarly ambiguous results have been observed regarding serum IgM where both reductions [37, 41,42,43] and increases [38, 45] were seen under intensive exercise conditions.
3 Cytokines, Inflammation, and URTI Susceptibility in Exercisers and Athletes
Physical exercise is a stimulus inducing multiple cytokine synthesis and release. At the same time, as mentioned above, it may have anti-inflammatory and immunomodulatory properties. In spite of an anti-inflammatory action, however, an acute bout of exercise results in increased release of acute phase proteins and inflammation cytokines (IL-6, IL-1β, MIP-1α, IL-8). Secondary to this, increased serum levels of anti-inflammatory cytokines have been observed (e.g., IL-10, IL-1ra) [15, 46,47,48,49,50,51]. Serum levels of anti-inflammatory IL-1ra protein observed in young speed skaters were negatively correlated with ambient air temperature during winter season in the outdoor training area, suggesting that serum IL-1ra is partly reflecting cold air exposure in winter athletes. In addition, serum IL-1ra was significantly elevated in winter season only in athletes not reporting frequent respiratory tract infections [52] which adds further insight into the significance of anti-inflammatory cytokine properties in conditioning susceptibility to respiratory infections.
Intensive exercise is accompanied by hyperventilation resulting in sequential warming and cooling of the airways. This may lead to epithelial cells dehydration and, subsequently, hyperosmolar stress causing increased release of chemokines, such as RANTES and IL-8 which, in turn, induce leukocyte influx to the airways.
As a result of decrease in Th1 cell numbers with Th2 numbers remaining at constant level, the Th1/Th2 balance is skewed toward Th2 predominance due to strenuous exercise. Such Th1/Th2 unbalance plays an important role in increasing URTI susceptibility. Cortisol and adrenaline released during exercise decrease the intensity of Th1-dependent response. Muscle fiber-derived IL-6 directly stimulates Th2-mediated response which—together with decreased Th1 response—is likely to contribute to lower efficacy of antiviral response mechanisms [53, 54].
It is hypothesized that persistent low-grade inflammation that is currently considered important in pathogenesis of, among others, cardiovascular and metabolic diseases may be present in the airways of subjects performing regular intensive exercise. Indeed, there is an increased flood of inflammatory cells (neutrophils, eosinophils, lymphocytes) in the athletes’ airways resulting from a hyperventilation-induced increase in airway osmolarity stimulating bronchial epithelial cells to release chemotactic factors. It has been, however, also observed that exercise bout leads to considerable lowering of the expression of adhesive particles on the surface of inflammatory cells explaining why airway inflammation may appear blunted in athletes in spite of the presence of multiple exercise-associated pro-inflammatory stimuli. The appearance of infection-like episodes without evidence for the role of infectious pathogens may result from a transient loss of control of such local inflammation due to external physicochemical factors present in the environment where exercise is performed (e.g., swimming pool disinfectants, cold and dry air hyperpnea) [13].
Intensity of inflammation is also associated with anti-inflammatory and immunomodulatory function of the Clara cell proteins (CC16) which has immunomodulatory and anti-inflammatory properties. Assessment of serum CC16 levels can also be a marker of airway epithelium damage. In Olympic athletes (as compared with a general population sample) significantly lower serum CC16 levels were ascertained, irrespective of the discipline performed or the training regime followed [55]. In addition, athletes reporting frequent respiratory infections had significantly lower serum CC16 as compared to illness-resistant athletes, and a serum CC16 level below 5 ng/mL was associated with more than twofold increase of frequent URTI risk.
4 Conclusions
Regular exercise of moderate intensity remains the best lifestyle intervention if long-term prophylaxis of respiratory infections and lowering of inflammation are aimed at. However, repeated and strenuous exercise may predispose to the development of respiratory tract infections. Careful screening of athletes, also including the use of questionnaires specifically designed, appears highly useful in managing those in whom respiratory symptoms impair sports performance.
Various aspects of changes in lifestyle and everyday routine, such as diet, sleep deprivation, traveling, jet lag, stress, community living, and general health status, should be considered as modifiers of URTI susceptibility even in apparently illness-prone subjects. Moreover, concomitant asthma, allergic diseases, and atopy may modify the susceptibility to respiratory infections.
In the case of respiratory symptoms in athletes, differential diagnoses should be also always considered (i.e., exercise-induced bronchoconstriction, vocal-cord dysfunction).
Several dietary supplements have been reported to restore a normal immune function and reduce the increased risk of URTI in athletes, including Vitamin C, glucose, lipids, zinc, Echinacea, and other minerals. However, data available are scarce and sometimes conflicting; systematic reviews and meta-analysis failed to show any effect for most of the remedies suggested [56,57,58,59,60,61].
Lastly, the high prevalence of URTI in athletes has induced some authors to recommend yearly vaccinations against influenza (and hepatitis A and B immunization) [62].
Key Points
-
Regular moderate physical activity is believed to contribute to a more effective immune response against respiratory infection agents.
-
Repeated and strenuous exercise predisposes to the development of symptoms suggestive of respiratory tract infections.
-
Intensive exercise training leads to decrease in salivary IgA which is frequently associated with an increased prevalence of respiratory symptoms.
-
Pathogens responsible for athletes’ upper respiratory tract infections (URTI) can be identified in less than half of the episodes.
References
Nieman D. Exercise, upper respiratory tract infection, and the immune system. Med Sci Sports Exerc. 1994;26(2):128–39.
Nieman D, Johanssen L, Lee J, Arabatzis K. Infectious episodes in runners before and after the Los Angeles Marathon. J Sports Med Phys Fitness. 1990;30(3):316–28.
Peters E, Bateman E. Ultramarathon running and upper respiratory tract infections. An epidemiological survey. S Afr Med J. 1983;64(15):582–4.
Nieman D, Johanssen L, Lee J. Infectious episodes in runners before and after a roadrace. J Sports Med Phys Fitness. 1989;29(3):289–96.
Robson-Ansley P, Howatson G, Tallent J, Mitcheson K, Walshe I, Toms C, et al. Prevalence of allergy and upper respiratory tract symptoms in runners of London Marathon. Med Sci Sports Exerc. 2012;44(6):999–1004.
Kostka T, Drygas W, Jegier A, Praczko K. Physical activity and upper respiratory tract infections. Int J Sports Med. 2008;29(2):158–62.
Nieman DC, Henson DA, Austin MD, Sha W. Upper respiratory tract infection is reduced in physically fit and active adults. Br J Sports Med. 2011;45(12):987–92.
Fondell E, Lagerros YT, Sundberg CJ, Lekander M, Bälter O, Rothman KJ, et al. Physical activity, stress, and self-reported upper respiratory tract infection. Med Sci Sports Exerc. 2011;43(2):272–9.
Malm C. Susceptibility to infections in elite athletes: the S-curve. Scand J Med Sci Sports. 2006;16(1):4–6.
Walsh N, Oliver S. Exercise, immune function and respiratory infection: an update on the influence of training and environmental stress. Immunol Cell Biol. 2016;94(2):132–9.
Spence L, Brown W, Pyne D, Nissen M, Sloots T, McCormack J, et al. Incidence, etiology, and symptomatology of upper respiratory illness in elite athletes. Med Sci Sports Exerc. 2007;39(4):577–86.
Cox AJ, Gleeson M, Pyne DB, Callister R, Hopkins WG, Fricker PA. Clinical and laboratory evaluation of upper respiratory symptoms in elite athletes. Clin J Sport Med. 2008;18(5):438–45.
Bermon S. Airway inflammation and upper respiratory tract infection in athletes: is there a link? Exerc Immunol Rev. 2007;13:6–14.
Mäkelä MJ, Puhakka T, Ruuskanen O, Leinonen M, Saikku P, Kimpimäki M, et al. Viruses and Bacteria in the etiology of the common cold. J Clin Microbiol. 1998;36(2):539–42.
Walsh N, Gleeson M, Shephard R, Gleeson M, Woods J, Bishop N, et al. Position statement. Part one: immune function and exercise. Exerc Immunol Rev. 2011;17:6–63.
Bonini M, Braido F, Baiardini I, Del Giacco S, Gramiccioni C, Manara M, et al. AQUA: allergy questionnaire for athletes. Development and validation. Med Sci Sports Exerc. 2009;41(5):1034–41.
Fahlman M, Engels H. Mucosal IgA and URTI in American college football players: a year longitudinal study. Med Sci Sports Exerc. 2005;37:374–80.
Tomasi T, Trudeau F, Czerwinski D, Erredge S. Immune parameters in athletes before and after strenuous exercise. J Clin Immunol. 1982;2:173–8.
Gleeson M, McDonald W, Pyne D, Cripps A, Francis J, Fricker P, et al. Salivary IgA levels and infection risk in elite swimmers. Med Sci Sports Exerc. 1999;31(1):67–73.
Gleeson M, McDonald WA, Cripps AW, Pyne DB, Clancy RL, Fricker PA. The effect on immunity of long-term intensive training in elite swimmers. Clin Exp Immunol. 1995;102(1):210–6.
Neville V, Gleeson M, Folland JP. Salivary IgA as a risk factor for upper respiratory infections in elite professional athletes. Med Sci Sports Exerc. 2008;40(7):1228–36.
Mortatti AL, Moreira A, Aoki MS, Crewther BT, Castagna C, de Arruda AFS, et al. Effect of competition on salivary cortisol, immunoglobulin A, and upper respiratory tract infections in elite young soccer players. J Strength Cond Res. 2012;26(5):1396–401.
Carins J, Booth C. Salivary immunoglobulin-A as a marker of stress during strenuous physical training. Aviat Space Environ Med. 2002;73:1203–7.
Tiollier E, Gomez-Merino D, Burnat P, Jouanin J, Bourrilhon C, Filaire E, et al. Intense training: mucosal immunity and incidence of respiratory infections. Eur J Appl Physiol. 2005;93:421–8.
Whitham M, Laing S, Dorrington M, Walters R, Dunklin S, Bland D, et al. The influence of an arduous military training program on immune function and upper respiratory tract infection incidence. Mil Med. 2006;171:703–9.
Vardiman JP, Riggs CE, Galloway DL, Waxman MB, Touchberry CD, Gallagher PM. Salivary IgA is not a reliable Indicator of upper respiratory infection in collegiate female soccer athletes. J Strength Cond Res. 2011;25(7):1937–42.
Moreira A, Bacurau RFP, Napimoga MH, Arruda AFS, Freitas CG, Drago G, et al. Salivary IL-21 and IGA responses to a competitive match in elite basketball players. Biol Sport. 2013;30(4):243–7.
Alexandre M, Franco A, Ramos CP, Clóvis F, Carlos SA, Roberto DOP, et al. The impact of a 17-day training period for an international championship on mucosal immune parameters in top-level basketball players and staff members. Eur J Oral Sci. 2008;116(5):431–7.
Milanez VF, Ramos SP, Okuno NM, Boullosa DA, Nakamura FY. Evidence of a non-linear dose-response relationship between training load and stress markers in elite female futsal players. J Sports Sci Med. 2014;13(1):22–9.
Moraes H, Aoki MS, Freitas CG, Arruda AFS, Drago G, Moreira A. SIgA response and incidence of upper respiratory tract infections during intensified training in youth basketball players. Biol Sport. 2017;34(1):49–55.
Oliver S, Laing S, Wilson S, Bilzon J, Walters R, Walsh N. Salivary immunoglobulinA response at rest and after exercise following a 48 h period of fluid and/or energy restriction. Br J Nutr. 2007;97:1109–16.
Walsh N, Gleeson M, Pyne D, Nieman D, Dhabhar F, Shephard R, et al. Position statement. Part two: maintaining immune health. Exerc Immunol Rev. 2011;17:64–103.
Bishop N, Gleeson M. Acute and chronic effects of exercise on markers of mucosal immunity. Front Biosci. 2009;14:4444–56.
Akimoto T, Kumai Y, Akama T, Hayashi E, Murakami H, Soma R, et al. Effects of 12 months of exercise training on salivary secretory IgA levels in elderly subjects. Br J Sports Med. 2003;37:76–9.
Klentrou P, Cieslak T, MacNeil M, Vintinner A, Plyley M. Effect of moderate exercise on salivary immunoglobulin A and infection risk in humans. Eur J Appl Physiol. 2002;87:153–8.
Moreira A, Mortatti AL, Arruda AFS, Freitas CG, de Arruda M, Aoki MS. Salivary IgA response and upper respiratory tract infection symptoms during a 21-week competitive season in young soccer players. J Strength Cond Res. 2014;28(2):467–73.
McKune A, Smith L, Semple S, Wadee A. Influence of ultra-endurance exercise on immunoglobulin isotypes and subclasses. Br J Sports Med. 2005;39:665–70.
Petibois C, Cazorla G, Deleris G. The biological and metabolic adaptations to 12 months training in elite rowers. Int J Sports Med. 2003;24:36–42.
Poortmans J. Serum protein determination during short exhaustive physical activity. J Appl Physiol. 1971;30:190–2.
Poortmans J, Haralambie G. Biochemical changes in a 100 km run: proteins in serum and urine. Eur J Phys. 1979;40:245–54.
Hejazi K, Hosseini S. Influence of selected exercise on serum immunoglobulin, testosterone and cortisol in semi-endurance elite runners. Asian J Sports Med. 2012;3:185–92.
Israel S, Buhl B, Neumann G. Die Konzentration der Immunglobuline A, G und M im Serum bei trainierten und untrainierten sowie nach verschiedenen sportlichen Ausdauerleistungen. Med Sport (Berlin). 1982;22:225–31.
Mashiko T, Umeda T, Nakaji S, Sugawara K. Effects of exercise on the physical condition of college rugby players during summer training camp. Br J Sports Med. 2004;38:186–90.
Nehlsen-Cannarella S, Nieman D, Jessen J, Chang L, Gusewitch G, Blix G, et al. The effects of acute moderate exercise on lymphocyte function and serum immunoglobulin levels. Int J Sports Med. 1991;12:391–8.
Nieman D, Nehlsen-Cannarella S. The effects of acute and chronic exercise on immunoglobulins. Sports Med. 1991;11:183–201.
Nielsen A, Pedersen B. The biological roles of exercise-induced cytokines: IL-6, IL-8, and IL-15. Appl Physiol Nutr Metab. 2007;32:833–9.
Nieman D, Dumke C, Henson D, McAnulty S, McAnulty L, Lind R, et al. Immune and oxidative changes during and following the Western states endurance run. Int J Sports Med. 2003;24:541–7.
Nieman D, Henson D, Smith L, Utter A, Vinci D, Davis J, et al. Cytokine changes after a marathon race. J Appl Physiol. 2001;91:109–14.
Pedersen B, Fischer C. Beneficial health effects of exercise--the role of IL-6 as a myokine. Trends Pharmacol Sci. 2007;28:152–6.
Cox A, Pyne D, Saunders P, Callister R, Gleeson M. Cytokine responses to treadmill running in healthy and illness-prone athletes. Med Sci Sports Exerc. 2007;39:1918–26.
Suzuki K, Nakaji S, Yamada M, Totsuka M, Sato K, Sugawara K. Systemic inflammatory response to exhaustive exercise. Cytokine kinetics. Exerc Immunol Rev. 2002;8:6–48.
Kurowski M, Jurczyk J, Moskwa S, Jarzębska M, Krysztofiak H, Kowalski ML. Winter ambient training conditions are associated with increased bronchial hyperreactivity and with shifts in serum innate immunity proteins in young competitive speed skaters. Arch Med Sci. 2018;14(1):60–8.
Gleeson M. Immune system adaptation in elite athletes. Curr Opin Clin Nutr Metab Care. 2006;9:659–65.
Lancaster G, Halson S, Khan Q, Drysdale P, Wallace F, Jeukendrup A, et al. Effects of acute exhaustive exercise and chronic exercise training on type 1 and type 2 T lymphocytes. Exerc Immunol Rev. 2004;10:91–106.
Kurowski M, Jurczyk J, Jarzębska M, Moskwa S, Makowska J, Krysztofiak H, et al. Association of serum Clara cell protein CC16 with respiratory infections and immune response to respiratory pathogens in elite athletes. Respir Res. 2014;15:45.
Peters EM, Goetzsche JM, Grobbelaar B, Noakes TD. Vitamin C supplementation reduces the incidence of postrace symptoms of upper-respiratory-tract infection in ultramarathon runners. Am J Clin Nutr. 1993;57:170–4.
Nieman DC. Exercise immunology: nutritional countermeasures. Can J Appl Physiol. 2001;26:S45–55.
Peck MD. Interactions of lipids with immune functions. Biochemical effects of dietary fatty lipids on plasma membranes. J Nutr Biochem. 1994;5:466–78.
Fraker PJ, Gershwin ME, Good RA, Prasad A. Interrelationships between zinc and immune function. Fed Proc. 1986;45:1474–9.
Barrett B, Vohmann M, Calabrese C. Echinacea for upper respiratory infection. J Fam Pract. 1999;48:628–35.
Moreira A, Kikkomen RA, Delgado L, Fonseca JA, Korpela R, Haahtela H. Nutritional modulation of exercise induced immunosuppression in athletes: a systematic review and metanalysis. Eur J Clin Nutr. 2007;61(4):443–60.
Constantini N, Ken-Dror A, Eliakim A, Galatzkia L, Morag A, Mann G, Volach B, Asharov J, Shoval D. Vaccinations in sports and recommendations for immunization against flu, hepatitis a and hepatitis B. Harefuah. 2001;1191-5(1228):140.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Kurowski, M. (2019). Respiratory Infections. In: Cogo, A., Bonini, M., Onorati, P. (eds) Exercise and Sports Pulmonology. Springer, Cham. https://doi.org/10.1007/978-3-030-05258-4_9
Download citation
DOI: https://doi.org/10.1007/978-3-030-05258-4_9
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-05257-7
Online ISBN: 978-3-030-05258-4
eBook Packages: MedicineMedicine (R0)