
Abstract
KP is a 32-year-old moderately myopic man who presented with the history of several days of flashing lights and “cobwebs with lots of tiny little dots” in his right eye. His vision was somewhat impaired by the floaters. Examination showed best-corrected vision in his right eye of 20/50 by moving his eye back and forth to see through the floaters. The visual acuity in the left eye was 20/20. Fundus examination found a mild vitreous hemorrhage in the right eye with a Weiss ring in the anterior vitreous. There was some clumping of blood inferiorly with the obscuration of the view of the retina in the inferotemporal quadrant.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
KP is a 32-year-old moderately myopic man who presented with the history of several days of flashing lights and “cobwebs with lots of tiny little dots” in his right eye. His vision was somewhat impaired by the floaters. Examination showed best-corrected vision in his right eye of 20/50 by moving his eye back and forth to see through the floaters. The visual acuity in the left eye was 20/20. Fundus examination found a mild vitreous hemorrhage in the right eye with a Weiss ring in the anterior vitreous. There was some clumping of blood inferiorly with the obscuration of the view of the retina in the inferotemporal quadrant.
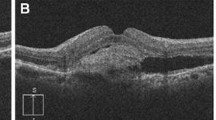
Echography revealed a partial posterior vitreous detachment with moderate intravitreal opacities consistent with hemorrhage. A focal area of vitreoretinal traction was noted at the 7:00 equator consistent with an elevated flap tear with focal subretinal fluid (Fig. 1). This was discussed with the patient, and he was advised to reduce physical activity, stop nonsteroidal anti-inflammatory drugs, and return every few days for repeat echography until the vitreous hemorrhage cleared enough to allow treatment of the retinal tear with careful monitoring of the degree of subretinal fluid.

B-scan of posterior vitreous detachment with vitreous traction and subretinal fluid (arrow)
Other causes of vitreous opacification include asteroid hyalosis. This condition is usually idiopathic and often unilateral. It can be dense enough to preclude visualization of the fundus, but the patient generally has surprisingly good vision. The reason for this optical paradox is not understood. A patient presenting for the first time to the examiner is best served by an ultrasound evaluation of the eye to rule out fundus pathology.
Author information
Authors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Harrie, R.P., Kendall, C.J. (2014). Case Study 87 Retinal Tear with Subretinal Fluid. In: Clinical Ophthalmic Echography. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-7082-3_87
Download citation
DOI: https://doi.org/10.1007/978-1-4614-7082-3_87
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-7081-6
Online ISBN: 978-1-4614-7082-3
eBook Packages: MedicineMedicine (R0)