
Abstract
ELP are uncommon diseases. The most frequent etiology is the chronic use of medicines containing mineral oily substances, mostly paraffin or vaseline, for constipation or rhinopharyngeal diseases.
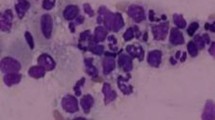
ELP are often asymptomatic. Diagnosis must be considered in case of patient history, with use of oily medicines, and imaging features, particularly hypodense consolidations, suggest it. This diagnosis must be confirmed by various examinations allowing to show presence of intrapulmonary oil, such as bronchoalveolar lavage or histological specimens of which fat stains will be used.
Endogenous lipid pneumonia must be eliminated.
Early recognition and discontinuation of exposure are essential to prevent the lesions from evolving towards fibrosis and respiratory failure.
Access this chapter
Tax calculation will be finalised at checkout
Purchases are for personal use only
Similar content being viewed by others


References
Laughlen GF. Studies on pneumonia following nasopharyngeal injections of oil. Am J Pathol. 1925;1:407–14.
Pinkerton H. The reaction to oils and fats in the lung. Arch Pathol. 1928;5:380–401.
Ikeda K. Lipoid pneumonia of the adult type. Arch Pathol. 1938;23:470–92.
Kaplan L. Combined cod liver oil and liquid petrolatum pneumonia in a child. Am J Dis Child. 1941;62:1217–23.
Sweeney WJ. Intranasal medication with oils. Eye Ear Nose Throat Mon. 1943;22:335–8.
Sodeman WA, Stuart HM. Lipoid pneumonia in adults. Ann Intern Med. 1946;24:241–53.
Volk BW, Nathanson L, Losner S. Incidence of lipoid pneumonia in a survey of 389 chronically ill patients. Am J Med. 1951;10:316–24.
Greenridge HW, Tuttle MJ. Lipoid pneumonia in a veteran’s hospital. Ann Intern Med. 1955;43:1259.
Rouffy J, Almosni M, Chelloul N. Aspects actuels des lipoidoses pulmonaires exogènes de l’adulte. Ann Med Interne (Paris). 1976;127(8–9):637–43.
Proudfit JP, Vanordstrand HT, Miller CW. Pneumonie graisseuse chronique à la suite d’exposition professionnelle. Arch Ind Hyg Occupat Med. 1950;1(1):105.
Wood EH. Unusual case of carcinoma of both lungs associated with lipoid pneumonia. Radiology. 1943;40:193–5.
Guest JL, Arean VM, Brenner HA. Group IV atypical mycobacterium infection occurring in association with mineral oil granuloma of lungs. Am Rev Respir Dis. 1967;95:656–62.
Polednak AP. Postmortem bacteriology and pneumonia in a mentally retarded population. Am Rev Respir Dis. 1977;67(2):190–5.
Ikeda K. Oil aspiration pneumonia: clinical-pathologic and experimental considerations. Am J Dis Child. 1935;49:985–1006.
Council on Pharmacy and Chemistry. Nasal inhalant preparations containing petrolatum omitted from N.N.R. JAMA. 1942;118:378.
Balakrishnan S. Lipoid pneumonia in infants and children in South India. Br Med J. 1973;4(5888):329–31.
Marchiori E, Zanetti G, Mauro Mano C, Hochheger B. Exogenous lipoid pneumonia. Clinical and radiological manifestations. Respir Med. 2011;105:659–66.
Gondouin A. Pneumonies lipidiques exogènes. Résultats d’une enquête rétrospective nationale (44 observations), Thèse de doctorat en médecine. Besançon: Université de Franche-Comté, Faculté de médecine et de Pharmacie; 1993.
Greenberger PA, Katzenstein A. Lipid pneumonia with atypical mycobacterial colonization. Association with allergic bronchopulmonary aspergillosis. Arch Intern Med. 1983;143(10):2003–5.
Oldenburger D, Maurer WJ, Beltaos E. Inhalation lipoid pneumonia from burning fats. A newly recognized industrial hazard. JAMA. 1972;222(10):1288–9.
Venuta F, Rendina EA, Pesacarmona EO. Lipoid pneumonia after laryngectomy mimicking pulmonary malignancy. Ann Thorac Surg. 1990;49(6):1026–7.
Cullen MR, Balmes JR, Robins JM. Lipoid pneumonia caused by oil mist exposure from a steel rolling tandem mill. Am J Ind Med. 1981;2(1):51–8.
Szabo-Gay O, Benoit N, Doutrellot-Philippon C, Le Meunier F, Sevestre H, Jounieaux V. Occupational lipid pneumonia induced by cutting fluids exposition. Presse Med. 2011;40(6):656–9.
Pujol JL, Barneon G, Bousquet J. Interstitial pulmonary disease induced by occupational exposure to paraffin. Chest. 1990;97(1):234–6.
Ameille J, Brochard P. Les pneumopathies lipidiques professionnelles. Rev Prat Med Gen. 1991;5(146):1767–70.
Meyer A. Huilome pulmonaire chez les chanteurs. Arch Mal Prof. 1976;37(9):629–31.
Gondouin A, Manzoni P, Ranfaing E, Brun J, Cadranel J, Sadoun D, Cordier JF, Depierre A, Dalphin JC. Exogenous lipid pneumonia: a retrospective multicentre study of 44 cases in France. Eur Respir J. 1996;9(7):1463–9.
Gentina T, Tilllie-leblond I, Birolleau S. Fire-eater’s lung: seventeen cases and a review of the literature. Medicine (Baltimore). 2001;80:291–7.
Marchiori E, Zanetti G, Mano CM, Irion KL, Daltro PA, Hochhegger B. Lipoid pneumonia in 53 patients after aspiration of mineral oil: comparison of high-resolution computed tomography findings in adults and children. J Comput Assist Tomogr. 2010;34(1):9–12.
Carette MF, Grivaux M, Monod B, Capeau F, Lebreton C, Bigot JM. MR findings in lipoid pneumonia. Am J Roentgenol. 1989;153(5):1097–8.
Franquet T, Giménez A, Bordes R, Rodríguez-Arias JM, Castella J. The crazy-paving pattern in exogenous lipoid pneumonia: CT-pathologic correlation. Am J Roentgenol. 1998;170(2):315–7.
Choi HK, Park CM, Goo JM, Lee HJ. Pulmonary alveolar proteinosis versus exogenous lipoid pneumonia showing crazy-paving pattern: comparison of their clinical features and high-resolution CT findings. Acta Radiol. 2010;51(4):407–12.
Fox BD, Shechtman I, Shitrit D, Bendayan D, Kramer MR. A “fat chance” it’s malignant: lipoid pneumonia simulating lung cancer on PET scan. Thorax. 2007;62(5):464.
Ridaura-Sanz C, Lopez-Corella E, Salazar-Flores M. Exogenous lipoid pneumonia superinfected with acid-fast bacilli in infants: a report of nine cases. Fetal Pediatr Pathol. 2006;25(2):107–17.
Haro M, Murcia I, Nunez A, Julia E, Valer J. Massive haemoptysis complicating exogenous lipid pneumonia. Eur Respir J. 1998;11(2):507–8.
Breton JL, Jeffredo Y, Ranfaing E, Clement F, Faure E, Garnier G. Associated lipid pneumonia and bronchiolo-alveolar carcinoma. Rev Mal Respir. 1994;11(6):596–8.
Sante LR. The fate of oil particles in the lung and their possible relationship to the development of bronchogenic carcinoma. Am J Roentgenol Radium Ther. 1949;62:788–97.
Rolla AR, Granfone A, Balogh K. Granuloma-related hypercalcemia in lipoid pneumonia. Am J Med. 1986;292(5):313–6.
Dossing M, Khan JH. Nasal or oral oil application on infants: a possible risk factor for adult bronchiectasis. Eur J Epidemiol. 1995;11(2):141–4.
Hugosson C, Bahabri S, Rifai A, al-Dalaan A. Hypertrophic osteoarthropathy caused by lipoid pneumonia. Pediatr Radiol. 1995;25(6):482–3.
Heckers H, Melcher FW, Dittmark K. Long-term course of mineral oil pneumonia. Lung. 1978;155:101–9.
Wong CA, Wilsher ML. Treatment of exogenous lipoid pneumonia by whole lung lavage. Aust N Z J Med. 1994;24(6):734–5.
Chang HY, Chen CW, Chen CY, Hsuie TR, Chen CR, Lei WW, Wu MH, Jin YT. Successful treatment of diffuse lipoid pneumonitis with whole lung lavage. Thorax. 1993;48(9):947–8.
Al-Malki TA. Lung resections in bronchiectasis due to lipoid pneumonia: a custom-design approach. East Afr Med J. 2000;77(4):203–5.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer-Verlag London
About this chapter
Cite this chapter
Gondouin, A., Dalphin, JC. (2015). Exogenous Lipoid Pneumonia. In: Cottin, V., Cordier, JF., Richeldi, L. (eds) Orphan Lung Diseases. Springer, London. https://doi.org/10.1007/978-1-4471-2401-6_19
Download citation
DOI: https://doi.org/10.1007/978-1-4471-2401-6_19
Published:
Publisher Name: Springer, London
Print ISBN: 978-1-4471-2400-9
Online ISBN: 978-1-4471-2401-6
eBook Packages: MedicineMedicine (R0)