
Abstract
Background
Previous studies have noted a high (41%) prevalence and poor discharge summary communication of pending laboratory (lab) tests at the time of hospital discharge for general medical patients. However, the prevalence and communication of pending labs within a high-risk population, specifically those patients discharged to sub-acute care (i.e., skilled nursing, rehabilitation, long-term care), remains unknown.
Objective
To determine the prevalence and nature of lab tests pending at hospital discharge and their inclusion within hospital discharge summaries, for common sub-acute care populations.
Design
Retrospective cohort study.
Participants
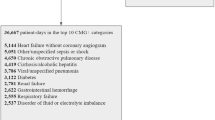
Stroke, hip fracture, and cancer patients discharged from a single large academic medical center to sub-acute care, 2003–2005 (N = 564)
Main Measures
Pending lab tests were abstracted from the laboratory information system (LIS) and from each patient’s discharge summary, then grouped into 14 categories and compared. Microbiology tests were sub-divided by culture type and number of days pending prior to discharge.
Key Results
Of sub-acute care patients, 32% (181/564) were discharged with pending lab tests per the LIS; however, only 11% (20/181) of discharge summaries documented these. Patients most often left the hospital with pending microbiology tests (83% [150/181]), particularly blood and urine cultures, and reference lab tests (17% [30/181]). However, 82% (61/74) of patients’ pending urine cultures did not have 24-hour preliminary results, and 19% (13/70) of patients’ pending blood cultures did not have 48-hour preliminary results available at the time of hospital discharge.
Conclusions
Approximately one-third of the sub-acute care patients in this study had labs pending at discharge, but few were documented within hospital discharge summaries. Even after considering the availability of preliminary microbiology results, these omissions remain common. Future studies should focus on improving the communication of pending lab tests at discharge and evaluating the impact that this improved communication has on patient outcomes.
Similar content being viewed by others

References
Forsman RW. Why is the laboratory an afterthought for managed care organizations? Clin Chem. 1996;42:813–6.
Roy CL, Poon EG, Karson AS, et al. Patient safety concerns arising from test results that return after hospital discharge. Ann Intern Med. 2005;143:121–8.
Were MC, Li X, Kesterson J, et al. Adequacy of hospital discharge summaries in documenting tests with pending results and outpatient follow-up providers. J Gen Intern Med. 2009;24:1002–6.
The Joint Commission. Standard RC.02.04.01. Available at: http://www.jointcommission.org/. Accessed October 20, 2010.
Kripalani S, LeFevre F, Phillips CO, Williams MV, Basaviah P, Baker DW. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297:831–41.
Coleman EA. Falling through the cracks: challenges and opportunities for improving transitional care for persons with continuous complex care needs. J Am Geriatr Soc. 2003;51:549–55.
Kind AJ, Smith MA, Frytak JR, Finch MD. Bouncing back: Patterns and predictors of complicated transitions 30 days after hospitalization for acute ischemic stroke. J Am Geriatr Soc. 2007;55:365–73.
Deutsch A, Fiedler RC, Granger CV, Russell CF. The Uniform Data System for Medical Rehabilitation report of patients discharged from comprehensive medical rehabilitation programs in 1999. Am J Phys Med Rehabil. 2002;81:133–42.
Deutsch A, Fiedler RC, Iwanenko W, Granger CV, Russell CF. The Uniform Data System for Medical Rehabilitation report: patients discharged from subacute rehabilitation programs in 1999. Am J Phys Med Rehabil. 2003;82:703–11.
Sahyoun NR, Pratt LA, Lentzner H, Dey A, Robinson KN. The changing profile of nursing home residents: 1985-1997. Aging Trends. 2001;4:1–8.
Jardine L, Davies MW, Faoagali J. Incubation time required for neonatal blood cultures to become positive. J Paediatr Child Health. 2006;42:797–802.
Kaplan RL, Harper MB, Baskin MN, Macone AB, Mandl KD. Time to detection of positive cultures in 28- to 90-day-old febrile infants. Pediatrics. 2000;106:E74.
Martinez JA, Pozo L, Almela M, et al. Microbial and clinical determinants of time-to-positivity in patients with bacteraemia. Clin Microbiol Infect. 2007;13:709–16.
Shah SS, Downes KJ, Elliott MR, Bell LM, McGowan KL, Metlay JP. How long does it take to "rule out" bacteremia in children with central venous catheters? Pediatrics. 2008;121:135–41.
Harrison JP, McDowell GM. The role of laboratory information systems in healthcare quality improvement. Int J Health Care Qual Assur. 2008;21:679–91.
McPherson RA, Pincus MR, Henry JB. Henry's Clinical Diagnosis and Management by Laboratory Methods. 21st ed. Philadelphia: Saunders Elsevier; 2007.
Cary NC, ed. SAS Statistical Software. 8.2. SAS Institute; 2002.
Stata Corporation. Stata Statistical Software. 8.0 ed. College Station, TX: Stata Corporation; 1999.
Hickey A, Clinch D, Groarke EP. Prevalence of cognitive impairment in the hospitalized elderly. Int J Geriatr Psychiatry. 1997;12:27–33.
Weaver FM, Guihan M, Hynes DM, Byck G, Conrad KJ, Demakis JG. Prevalence of subacute patients in acute care: results of a study of VA hospitals. J Med Syst. 1998;22:161–72.
Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418–28.
Berild D, Mohseni A, Diep LM, Jensenius M, Ringertz SH. Adjustment of antibiotic treatment according to the results of blood cultures leads to decreased antibiotic use and costs. J Antimicrob Chemother. 2006;57:326–30.
McIsaac WJ, Moineddin R, Ross S. Validation of a decision aid to assist physicians in reducing unnecessary antibiotic drug use for acute cystitis. Arch Intern Med. 2007;167:2201–6.
Swanson JM, Wood GC, Croce MA, Mueller EW, Boucher BA, Fabian TC. Utility of preliminary bronchoalveolar lavage results in suspected ventilator-associated pneumonia. J Trauma. 2008;65:1271–7.
Poon EG, Gandhi TK, Sequist TD, Murff HJ, Karson AS, Bates DW. "I wish I had seen this test result earlier!": dissatisfaction with test result management systems in primary care. Arch Intern Med. 2004;164:2223–8.
Isaac DR, Gijsbers AJ, Wyman KT, Martyres RF, Garrow BA. The GP-hospital interface: attitudes of general practitioners to tertiary teaching hospitals. Med J Aust. 1997;166:9–12.
Meara JR, Wood JL, Wilson MA, Hart MC. Home from hospital: a survey of hospital discharge arrangements in Northamptonshire. J Public Health Med. 1992;14:145–50.
Pantilat SZ, Lindenauer PK, Katz PP, Wachter RM. Primary care physician attitudes regarding communication with hospitalists. Am J Med. 2001;111:15–20.
Wahls T, Haugen T, Cram P. The continuing problem of missed test results in an integrated health system with an advanced electronic medical record. Jt Comm J Qual Patient Saf. 2007;33:485–92.
Acknowledgments
The authors would like to acknowledge the contributions of key people who helped make this project a success: Patty Horstmeier, Donald Wiebe, Wen-Jan Tuan, Patrick Ferguson and Peggy Munson.
Funding for this project was provided by the University of Wisconsin (UW) Hartford Center of Excellence in Geriatrics and the UW Health Innovation Program. Dr. Kind is supported by a K-L2 through the NIH grant 1KL2RR025012-01 [Institutional Clinical and Translational Science Award (UW-Madison) 1UL1RR025011 (KL2) program of the National Center for Research Resources, National Institute of Health]. Additional support was provided by the Health Innovation Program and the Community-Academic Partnerships core of the University of Wisconsin Institute for Clinical and Translational Research (UW ICTR), grant 1UL1RR025011 from the Clinical and Translational Science Award (CTSA) program of the National Center for Research Resources, National Institutes of Health. The project described was supported by Award Number K23AG034551 from the National Institute on Aging. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Aging or the National Institutes of Health.
We presented an earlier version of the manuscript as a poster at the American Geriatrics Society Annual Meeting in Orlando, Florida, in May 2010.
Conflicts of Interest
None disclosed.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Walz, S.E., Smith, M., Cox, E. et al. Pending Laboratory Tests and the Hospital Discharge Summary in Patients Discharged To Sub-Acute Care. J GEN INTERN MED 26, 393–398 (2011). https://doi.org/10.1007/s11606-010-1583-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-010-1583-7