
Abstract
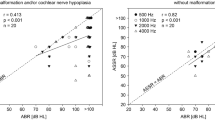
The inclusion of the auditory steady-state response (ASSR) into test-batteries for objective audiometry has allowed for clinical comparisons with the most widely used procedure, the auditory brainstem response (ABR). The current study describes ASSR and ABR thresholds for a group of infants and young children with various types and degrees of hearing loss. A sample of 48 subjects (23 female) with a mean age of 2.8 ± 1.9 years SD were assessed with a comprehensive test-battery and classified according to type and degree of hearing loss. Thresholds were determined with a broadband click-evoked ABR and single frequency ASSR evoked with continuous tones (0.25–4 kHz) amplitude modulated (67–95 Hz). Mean difference scores (±SD) between the ABR and high frequency ASSR thresholds were 9.8 (±11), 3.6 (±12) and 10.5 (±12) dB at 1, 2 and 4 kHz, respectively. An ASSR mean threshold for 2–4 and 1–4 kHz compared to the ABR threshold revealed an average difference of 7 (±9) and 7.9 (±8) dB, respectively. The overall correlation between the ABR and ASSR thresholds was highest for the mean ASSR thresholds of 2–4 and 1–4 kHz (r = 0.92 for both conditions). Correlations between the ABR and individual ASSR frequencies were slightly less (0.82–0.86). The average of the 2–4 kHz ASSR thresholds correlated best with the click-evoked ABR for all categories of hearing loss except for the sensorineural hearing loss category for which the 1–4 kHz ASSR average was better correlated to ABR thresholds. Findings demonstrate the reliability of verifying high frequency ASSR thresholds with a click-evoked ABR as an important cross-check in infants for whom behavioural audiometry may not be possible.

Similar content being viewed by others


References
Canale A, Lacilla M, Cavalot AL, Albera R (2006) Auditory steady-state responses and clinical applications. Eur Arch Otorhinolaryngol 263:499–503
Firszt JB, Gaggl W, Runge-Samuelson CL, Burg LS, Wackym A (2004) Auditory sensitivity in children using the auditory steady-state response. Arch Otolaryngol Head Neck Surg 130:536–540
Gorga MP, Neely ST, Hoover BM, Dierking DM, Beauchaine KL, Manning C (2004) Determining the upper limits of stimulation for auditory steady-state response measurements. Ear Hear 25:302–307
Johnson TA, Brown CJ (2005) Threshold prediction using the auditory steady-state response and the tone burst auditory brainstem response: a within-subject comparison. Ear Hear 26:559–576
Lins OG, Picton TW, Boucher BL, Durieux-Smith A, Champagne SC, Moran LM, Perez-Abalo MC, Martin V, Savio G (1996) Frequency-specific audiometry using steady-state responses. Ear Hear 17:81–96
Oates P, Stapells DR (1998) Auditory brainstem response estimates of the pure-tone audiogram: current status. Semin Hear 19:61–85
Picton TW, John MS (2004) Avoiding electromagnetic artifacts when recording auditory steady-state responses. J Am Acad Audiol 15:541–554
Picton TW, John MS, Dimitrijevic A, Purcell D (2003) Human auditory steady-state responses. Int J Audiol 42:177–219
Picton TW, Dimitrijevic A, Perez-Abalo M, Van Roon P (2005) Estimating audiometric thresholds using auditory steady-state responses. J Am Acad Audiol 16:140–156
Rance G, Briggs RJS (2002) Assessment of hearing in infants with moderate to profound impairment: the Melbourne experience with auditory steady-state evoked potential testing. Ann Otol Rhinol Laryngol 111(Suppl 189):22–28
Rance G, Rickards FW, Cohen LT, De Vidi S, Clark GM (1995) The automated prediction of hearing thresholds in sleeping subjects using auditory steady-state evoked potentials. Ear Hear 16:499–507
Roberson JB, O’Rourke C, Stidham KR (2003) Auditory steady-state response testing in children: evaluation of a new technology. Otolaryngol Head Neck Surg 129:107–113
Scherf F, Brokx J, Wuyts FL, Van de Heyning PH (2006) The ASSR: clinical application in normal hearing and hearing-impaired infants and adults, comparison with the click-evoked ABR and pure-tone audiometry. Int J Audiol 45:281–286
Schmulian D, Swanepoel D, Hugo R (2005) Predicting pure-tone thresholds with dichotic multiple frequency auditory steady state responses. J Am Acad Audiol 16:5–17
Small SA, Stapells DR (2004) Artifactual responses when recording auditory steady-state responses. Ear Hear 25:611–623
Stapells D (1989) Auditory brainstem response assessment of infants and children. Semin Hear 10:229–251
Stapells DR (2000) Frequency-specific evoked potential audiometry in infants. In: Seewald RC (ed) A sound foundation through early amplification: proceedings of an international conference. Phonak AG, Chicago, pp 13–31
Stueve MP, O’Rourke C (2003) Estimation of hearing loss in children comparison of auditory steady-state response, auditory brainstem response, and behavioral test methods. Am J Audiol 12:125–136
Swanepoel D, Erasmus H (2007) Auditory steady-state responses for estimating moderate hearing loss. Eur Arch Otorhinolaryngol 264:755–759
Swanepoel D, Schmulian D, Hugo R (2004) Establishing normal hearing with the dichotic multiple-frequency auditory steady-state response compared to an auditory brainstem response protocol. Acta Otolaryngol 124:62–68
Swanepoel D, Steyn K (2005) Short report: establishing normal hearing for infants with the auditory steady-state response. S Afr J Commun Disord 52:36–39
Vander Werff KR, Brown CJ, Gienapp BA, Schmidt Clay KM (2002) Comparison of auditory steady-state response and auditory brainstem response thresholds in children. J Am Acad Audiol 13:227–235
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Swanepoel, D., Ebrahim, S. Auditory steady-state response and auditory brainstem response thresholds in children. Eur Arch Otorhinolaryngol 266, 213–219 (2009). https://doi.org/10.1007/s00405-008-0738-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-008-0738-1