
Abstract
Introduction
The high mortality rate associated with sepsis necessitates a timely identification of the causative organism in order to optimize antimicrobial therapy. PCR assays are increasingly being used for this purpose. The aim of this study was to compare three commercially available PCR systems for the diagnosis of systemic infections.
Patients and methods
In a prospective observational study, a broad-range (SepsiTest®; Molzym, Bremen, Germany) and two multiplex PCR assays (VYOO®; SIRS-Lab, Jena, Germany and LightCycler® SeptiFast; Roche, Mannheim, Germany) were compared to blood cultures with respect to the clinical course of 50 critically ill patients with sepsis, severe sepsis or septic shock.
Results
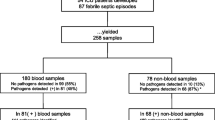
Pathogens were detected by PCR in 12 % (SepsiTest®), 10 % (VYOO®) and 14 % (LightCycler® SeptiFast) of samples and in 26 % by blood culture. Negative results were obtained using all four methods in 32 samples (64 %) and 3 (6 %) samples were positive in all tests. Upon consideration of additional diagnostic findings and the clinical course, eight (16 %) of the positive blood culture results were deemed clinically relevant. All three PCR assays could also identify the causative organism (or a specific gene thereof) in three of these eight positive blood cultures, whereas for five of the eight, all three PCR assays were negative. In one patient with a negative blood culture, the SepsiTest®, VYOO® and LightCycler® SeptiFast assays were positive for Streptococcus species. The PCR assays appeared to be less susceptible than blood cultures to false-positive results arising from contamination with coagulase-negative staphylococcal organisms.
Conclusion
There was some variability between the three PCR assays tested and the corresponding blood cultures with regards to the type of pathogen detected. The three PCR assays appeared to be less susceptible to false-positive results than blood cultures.
Zusammenfassung
Einleitung
Die hohe Letalität der Sepsis impliziert die möglichst rasche Identifizierung des auslösenden Erregers zur antibiotischen Therapieoptimierung. Hierzu werden zunehmend Verfahren verwendet, die auf der Polymerase-Kettenreaktion (PCR) basieren. Ziel dieser Studie war der Vergleich von 3 PCR-basierten Verfahren zur Erregerdetektion bei systemischen Infektionen.
Methoden
In einer prospektiven Observationsstudie wurden an 50 kritisch kranken Patienten mit Sepsis, schwerer Sepsis oder septischem Schock ein Breitspektrum-PCR-Verfahren (SepsiTest®, Molzym, Bremen) sowie 2 Multiplex-PCR-Verfahren (VYOO®, SIRS-Lab, Jena, und LightCycler® SeptiFast, Roche, Mannheim) mit der Blutkultur hinsichtlich des klinischen Kontexts verglichen.
Ergebnisse
Erreger wurden in 12 % (SepsiTest®), 10 % (VYOO®), 14 % (Light Cycler® SeptiFast) sowie 26 % der Fälle in der Blutkultur identifiziert. Insgesamt 32 Proben (64 %) waren in allen 4 Verfahren negativ, 3 (6 %) in allen Verfahren positiv. Acht (16 %) positive Blutkulturen wurden im klinischen Zusammenhang mittels zusätzlicher Befunde als klinisch relevant eingestuft. In 3 dieser 8 Fälle konnte der Erreger – oder ein spezifisches Gen – mittels aller 3 PCR-Verfahren nachgewiesen werden. Bei 5 der 8 relevanten positiven Blutkulturen waren alle 3 PCR-Verfahren negativ. In einer negativen Blutkultur waren SepsiTest®, VYOO® und Light Cycler® SeptiFast positiv für Streptokokken. Die PCR-Verfahren scheinen im Vergleich zur Blutkultur weniger anfällig für falsch-positive Befunde durch Kontamination mit Koagulase-negativen Staphylokokken zu sein.
Schlussfolgerung
Hinsichtlich der identifizierten Erreger gibt es einige Unterschiede zwischen den 3 untersuchten PCR-Verfahren und der entsprechenden Blutkultur. Die 3 PCR-Verfahren erscheinen weniger anfällig für falsch-positive Befunde.
Similar content being viewed by others

Introduction
Sepsis is associated with a high mortality rate and remains a serious condition in intensive care medicine [1]. Estimates for the prevalence of sepsis (or severe sepsis) and septic shock in German intensive care units (ICU) are 12 and 11 %, respectively. Transposing these figures to the German population would equate to 154,000 new cases of sepsis per year. Sepsis accounts for approximately 60,000 fatalities annually and is the third most common cause of death in Germany [2]. Timely commencement of an appropriate antibiotic treatment is directly related to survival rate [3, 4, 5, 6]. Rapid and reliable detection of the causative agent is therefore crucial to optimizing treatment and improving survival rates. Blood cultures still represent the gold standard in microbiological diagnostics, alongside other cultures from localized specimens like tracheal aspirates, urine and wound swabs. Unfortunately, the currently available diagnostic tests are unable to detect the causative organism or source of infection in a considerable number of cases, despite a high clinical probability of infection [7]. Furthermore, bacteremia can only be detected in approximately 30 % of patients with severe sepsis or septic shock [8]. A promising new approach to identify relevant microorganisms and their resistance genes within 6–8 h of blood sampling are assays based on the polymerase chain reaction (PCR). Following extraction and purification, nucleic acid (NA) can be rapidly amplified by PCR, and specific NAs subsequently identified. These assays should enable an earlier commencement of specific antibiotic treatment compared to using blood cultures. In addition, this approach may overcome the insufficiencies of initial empiric antibiotic therapies regarding multi-resistant bacteria, which are a rapidly increasing problem in ICUs. A number of different PCR-based assays are now being used increasingly to identify the causative organism in sepsis. One approach for rapid identification of the causative microorganism out of a range of potential pathogens is the so-called multiplex PCR assay (VYOO®; SIRS-Lab, Jena, Germany and LightCycler® SeptiFast; Roche, Mannheim, Germany). These assays allow for parallel detection of species- or genus-specific targets in different microorganisms. Another approach is the broad-range identification of pathogens by amplifying parts of the rRNA and other bacterial or fungal genes, followed by sequence analysis of the species (SepsiTest®; Molzym, Bremen, Germany).
The vast majority of studies have investigated the LightCycler® SeptiFast assay. Furthermore, no study to date has directly compared the three different PCR assays. Therefore, the aim of this pilot study was to compare the three commercially available PCR tests with each other and with blood cultures.
Patients and methods
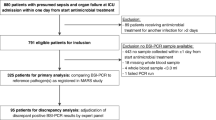
This prospective observational study was conducted between April and July 2009 in the Department of Intensive Care Medicine at the University Medical Center, Hamburg-Eppendorf, Germany. Inclusion criteria for the 50 patients recruited were a minimum age of 18 years, as well as clinical symptoms and signs consistent with the diagnosis of sepsis according to the sepsis criteria of the German Sepsis Competence Network [8]. Approval from the local ethics board was obtained, as was informed consent from each of the patients or their legal representative.
Following diagnosis of sepsis, severe sepsis or septic shock, blood culture samples were taken as part of the routine diagnostic workup and one additional 5 ml vial of blood was drawn for the PCR-based analysis. The following three PCR assays were performed:
-
1.
SepsiTest®
-
2.
VYOO®
-
3.
LightCycler® SeptiFast
The two multiplex PCR assays—VYOO® and LightCycler® SeptiFast—are built to detect targets in a predefined panel representing the most important sepsis pathogens by either species- or genus-specific fluorescent probes or electrophoretic separation of target-specific NA. The third assay, SepsiTest®, uses eubacterial and panfungal real-time PCR (rtPCR) to detect bacterial and fungal pathogens by virtue of their 16S and 18S ribosomal RNA (rRNA). Following gene-based universal PCR, the amplification product is sequenced for species identification [9].
Sample processing and PCR analysis was conducted by the Department of Clinical Microbiology, Virology and Hygiene at the University Medical Center. Modification of initial empiric antimicrobial therapy was based exclusively on the results of the blood cultures. Results of the multiplex PCR assays were not available to the attending intensivist.
Following recruitment, Simplified Acute Physiology Score II (SAPS II) [10], as well as C-reactive protein (CRP) and procalcitonin (PCT) values and leukocyte count were recorded. The following general and clinical data were also obtained: age, gender, diagnosis, treatment history, date of sampling, as well as the results of all microbiological tests, imaging and clinical follow-up examinations.
Processing of blood cultures
Collection and processing of the blood cultures and the ethylenediaminetetraacetic acid (EDTA) treated blood samples was conducted according to the German Society of Hygiene and Microbiology (DGHM) standards for microbiological/infectiological quality (MIQ) in diagnostics [11]. Immediately after sampling, the containers for blood cultures (Aerobe: BD BACTEC PLUS Aerobic/F, anaerobe: BD BACTEC PLUS Anaerobic/F; BD Diagnostics, Germany) were transported to the Institute of Medical Microbiology for cultivation at 37 °C. Further processing was carried out according to the institute’s quality standards and operating procedures. All aerobic and anaerobic blood culture samples were incubated for a total of 7 days in the Bactec® 9240 and 9120 analysis devices (BD Diagnostics, Germany), respectively. In the event of bacterial growth, subsamples were taken to inoculate blood- and McConkey agar plates, as well as to produce a gram stain and determine antibiotic sensitivities. In the event of anaerobic growth, an additional sample was taken to inoculate a Schaedler agar plate. In each instance of bacterial growth, all subspecies were differentiated and antibiotic sensitivities determined. Following completion of analysis, positive cultures were deep frozen at −80 °C.
In the event of a positive finding in the blood cultures, the microbiologist immediately informed the responsible intensivist and a written report was generated and sent to the ICU. For the comparison with the results of the PCR-based assays, processing and interpretation of the blood cultures was done in a blinded fashion.
Processing of PCR assays
The EDTA blood samples were stored at 4–10 °C and the NA was extracted within 24 h, according to the manufacturers’ specifications. Processing, NA extraction and PCR were performed by the laboratory technicians at the Institute of Medical Microbiology. All analytical steps of each of the assays were performed according to the manufacturers’ specifications. The results were interpreted by the attending microbiologist.
Integration and interpretation of results
The integration of clinical and laboratory data, as well as microbiological and PCR-based assay results was performed by the study investigators. The results of each of the three PCR assays were compared to the results of the blood cultures. Interpretation of the clinical relevance of each result was performed by an intensivist and a microbiologist from outside the study team. The final clinical diagnosis—which served as the reference standard—was made on the basis of all available clinical information. This included the clinical course, physical examinations and intraoperative findings, as well as all the results of laboratory, microbiological and pathological tests and imaging. The blood culture and PCR results were then compared to the final clinical diagnosis and categorized as true- or false-positive and true- or false-negative.
Results
The study included 50 critically ill patients. Results from the three PCR assays and blood cultures were available for all patients. At the point of inclusion in the study, all patients fulfilled the criteria for sepsis and 27 patients (54 %) were in septic shock, requiring significant vasopressor support. The demographics and mortality rates of the study population are illustrated in Tab. 1. At the point of recruitment into the study, 36 of the 50 patients (72 %) had received antibiotic treatment.
Blood cultures were positive in 13 patients (26 %). Staphylococcus epidermidis was identified in 6 patients, Streptococcus pneumoniae, Candida albicans, Staphylococcus aureus, Enterococcus faecium, Enterobacter aerogenes, Citrobacter coseri and Peptostreptococcus species were each identified in one patient. Considering all clinical information, eight of the positive blood culture results were deemed relevant. All positive microbiological and/or PCR results and their clinical interpretations are presented in Tab. 2.
Two of the eight (25 %) clinically relevant pathogens found in blood cultures could also be identified by all three multiplex PCR assays (Streptococcus pneumoniae and Staphylococcus aureus). In one additional case, while Staphylococcus epidermidis was identified in both the blood culture and the SepsiTest®, coagulase-negative Staphylococcus was found by the LightCycler® SeptiFast and the specific mecA resistance gene was identified in the VYOO® assay.
In five of the eight (62.5 %) relevant positive blood cultures, no pathogen could be identified by any of the three PCR assays. The pathogens identified in these five blood cultures were Candida albicans, Staphylococcus epidermidis, Enterobacter aerogenes, Citrobacter koseri and Enterococcus faecium.
In one blood culture-negative patient, two assays—SepsiTest® and VYOO®—identified Streptococcus agalactiae, whereas the third assay, the LightCycler® SeptiFast, found Streptococcus species.
In 32 patients (64 %), all methods—blood cultures and PCR assays— showed concordant negative results. There was a trend towards a higher rate of positive results in the PCR-based assays with increasing severity of sepsis (Tab. 3) and a lower detection rate for patients with low PCT levels. The detection rate for all three PCR assays was lower than that of the blood cultures with respect to the total number of pathogens detected and those considered clinically relevant.
Results of the individual PCR assays
SepsiTest®
The SepsiTest® assay identified pathogens in six instances (12 %). The following organisms were each detected once (Tab. 4): Staphylococcus epidermidis, Staphylococcus aureus, Streptococcus pneumoniae, Streptococcus agalactiae, Streptococcus constellatus, and Klebsiella pneumoniae. In three cases (Streptococcus pneumoniae, Staphylococcus aureus, and Staphylococcus epidermidis), the PCR results were consistent with the findings of the blood cultures. In 2 patients, the pathogens identified by the PCR based assay (Streptococcus agalactiae and Streptococcus constellatus) corresponded to negative blood cultures. Both findings were deemed clinically relevant, because the same pathogens had been isolated in other culture specimens and were likely to be the causative agent of sepsis. In one case there was a discrepancy between the findings of the PCR assay and the blood culture: Staphylococcus epidermidis was identified in the blood culture and Klebsiella pneumoniae by the SepsiTest®. As the patient’s clinical condition improved markedly following initiation of a Klebsiella pneumonae targeted antibiotic treatment, the Klebsiella finding was considered relevant. However, Staphylococcus epidermidis was interpreted as contamination. In five of the eight clinically relevant positive blood cultures, the SepsiTest® assay was negative. In 35 patients (70 %), both blood cultures and the SepsiTest® assay were negative.
VYOO®
The VYOO® assay identified pathogens in five cases (10 %). The following organisms and resistance gene were each detected once (Tab. 5): Escherichia coli, Staphylococcus aureus, Streptococcus pneumoniae, Streptococcus agalactiae and the mecA resistance gene. In two cases, the PCR results were consistent with the findings of the blood cultures (Streptococcus pneumoniae and Staphylococcus aureus). In one additional patient, the staphylococcal resistance gene mecA was detected, consistent with the growth of Staphylococcus epidermidis in blood culture. MecA can be found in all oxacillin (methicillin) resistant Staphylococcus aureus (MRSA) and coagulase-negative Staphylococcus species [12]. In two cases, the pathogens identified by the VYOO® PCR assay (Streptococcus agalactiae and Escherichia coli) corresponded to negative blood cultures. However, both of these PCR findings were considered relevant because these pathogens were also found in other specimens. In five of the eight clinically relevant positive blood cultures, the VYOO® assay was negative. In 36 patients (72 %) both blood cultures and the VYOO® assay were negative.
LightCycler® SeptiFast
The LightCycler® SeptiFast assay identified eight pathogens in seven samples. The following organisms were detected (Tab. 6): Enterococcus faecium, Aspergillus fumigatus, coagulase-negative Staphylococci, Staphylococcus aureus, Streptococcus pneumoniae, streptococcal species, Klebsiella pneumoniae/oxytoca, and Enterobacter cloacae/aerogenes. In one sample, two pathogens were detected by means of PCR (Enterococcus faecium and Aspergillus fumigatus), but only Enterococcus faecium was considered clinically relevant, because it was also cultivated from an earlier wound swab. The Aspergillus fumigatus was not deemed relevant because there were no clinical or microbiological indications of an invasive aspergillosis either at this time or during the subsequent clinical course. In three cases the PCR results were consistent with the findings of the blood cultures: Streptococcus pneumoniae, Staphylococcus aureus, and Staphylococcus epidermidis (blood culture)/coagulase-negative Staphylococcus (LightCycler® SeptiFast). In four cases, the pathogens identified by the LightCycler® SeptiFast assay corresponded to negative blood cultures. However, two of these four findings were deemed clinically relevant. The PCR-based finding of Streptococcal species was considered relevant because in this patient, ß-hemolytic streptococci had been cultivated from other specimens.
The positive result for Enterobacter aerogenes/cloacae was not considered relevant, since no clinical improvement was observed after treatment with an Enterobacter-targeted antibiotic therapy. The positive PCR result for Klebsiella pneumoniae/oxytoca was not considered relevant either, because the result was obtained after 14 days of treatment with meropenem.
In five of the eight relevant positive blood cultures, the LightCycler® SeptiFast assay was negative. In 33 patients (66 %), both blood cultures and the LightCycler® SeptiFast assay were negative.
In contrast to the other two PCR-based assays (SepsiTest® and VYOO®), the LightCycler® SeptiFast assay does not differentiate between either Enterobacter aerogenes and cloacae, or Klebsiella pneumoniae and oxytoca species. Furthermore, it does not distinguish between subtypes of coagulase negative Staphylococci and also classifies Streptococcus pyogenes, agalactiae, and mitis as Streptococcus species.
Discussion
The results of the three PCR assays performed using samples from critically ill sepsis patients showed some variation in comparison to each other and in relation to the corresponding blood cultures. Although the detection rate of all PCR-based assays was lower than that of the blood cultures, almost every third (30.8 %) positive blood culture represented a false-positive finding. Up until now, no published study had compared three different PCR assays with each other and to the results blood cultures for critically ill patients.
Due to the high sepsis-related mortality rates, the necessity of infectious source control and a timely and adequate anti-infective therapy, rapid identification of the causative pathogen and its susceptibility has a high priority. Cultivating organisms from blood cultures—still considered the gold standard for the detection of pathogens—is very time consuming. In a clinical study by Wellinghausen et al. [13], the mean time taken to reach a positive result was 19.2 h (range 6.7–58.4). In other cases, up to 120 h have been required [14]. Moreover, blood cultures have a low detection rate, particularly when samples are taken from patients who already receiving empiric anti-infective treatment [15].
Most studies investigating PCR assays have examined the LightCycler® SeptiFast assay. In the majority of these publications, the PCR-based assay identified more pathogens than the corresponding blood cultures [16, 17, 18, 19]. Lodes et al. [20] recently published a study that also showed a higher detection rate of the LightCycler® SeptiFast assay in 104 ICU surgery patients (39.9 % LightCycler® SeptiFast vs. 20.3 % blood culture). These results stand in contrast to the results of our study, where the blood cultures showed a higher pathogen detection rate. Other recent research is in line with our results: studies investigating patients with suspected sepsis in the emergency department [21], patients with malignancies and sepsis [22], critically ill neutropenia patients [23] and etiological diagnosis of community-onset bloodstream infections [24].
The other two PCR assays (SepsiTest® and VYOO®) are less well studied in respect to sepsis. In their multicenter study, Wellinghausen et al. [13] investigated the SepsiTest® assay using 342 samples from 187 patients with systemic inflammatory response syndrome (SIRS), sepsis or neutropenic fever. They documented a higher rate of positive results as compared to blood cultures. Bloos et al. studied the VYOO® assay in 24 patients with severe sepsis and 22 patients with SIRS. In sepsis patients, the VYOO® assay gave more positive results than the blood cultures, whereas in SIRS patients, the blood cultures were positive in five cases but no pathogens were identified by the PCR assay [25]. However, in contrast to the VYOO® version used by Bloos et al., the newer version of the assay that we employed has been further developed as a commercially available test using automated protocol steps.
Among our patient group, the rate of positive blood cultures was 26 %. This is comparable to the results of some earlier studies [26, 27]. In studies performed in emergency departments, the rates of positivity were generally higher. In a recent study, Hettwer et al. [28] documented positive cultures in 43.5 % of patients admitted to a multidisciplinary emergency department with suspected severe infection. The main reason for lower positivity rates of blood cultures in ICU patients is the fact that these patients are more often already on antibiotic treatment at the time of sampling. In accordance with this, 72 % of the patients in our study group were receiving antibiotic treatment at the time of sampling.
In most studies comparing PCR-based assays with blood cultures, more pathogens were detected by the PCR techniques. However, a positive PCR result—particularly in the absence of blood culture confirmation—should always be assessed critically within the individual clinical and microbiological context. Positivity in a PCR-based assay may well reflect a real infection, but could also result of external contamination, the presence of the NA of non-viable microorganisms, or even be obtained from freely circulating phagocytised microbial DNA from microorganisms already destroyed [29]. The last three scenarios would result in an unnecessary use of antibiotics.
Beyond the diagnostic properties, there is some preliminary evidence that the presence of microbial DNA in the blood of sepsis patients (in the absence of a positive blood culture) may also have a prognostic value. In their prospective study, Bloos et al. [17] evaluated 142 patients with severe sepsis. Patients with a positive PCR assay result had higher organ dysfunction scores and a trend toward higher mortality compared to patients with a negative result (39.1 % vs. 25.3 %, p = 0.115). Further studies are necessary to evaluate the potential prognostic value of detecting microbial NA using PCR-based assays in sepsis patients.
Diagnostic studies addressing the validity and reliability of PCR-based assays for identification of the causative microorganism in sepsis patients are generally faced with the problem of choosing an appropriate reference standard. Blood cultures are often considered the gold standard, but these have limited validity themselves [29]. In our study, we sought to overcome these problems by distinguishing between false- and true-positive PCR assay results by using all available clinical information, including the results of additional microbiological tests and imaging, as well as the clinical course of the patient (Tab. 7). Using this approach, the results of the PCR-based assays were deemed to be true-positive in five cases without a corresponding positive blood culture. One of these cases showed the same microbiological species (Streptococcus agalactiae/species) in all three assays. There was no instance of conflicting results between the three PCR-based assays.
Not all pathogens cultivated in blood cultures were also detected by PCR despite being included in the panel of the PCR assays (except in the case of Citrobacter species, which are not included in the panels of VYOO® and LightCycler® SeptiFast). In 8 % of all the patients in our study, coagulase-negative Staphylococcus species were identified in blood cultures but considered to be contamination. In contrast, none of the three PCR assays identified coagulase-negative staphylococci as a result of contamination. This higher contamination rate of blood cultures compared to the PCR assays is in line with other studies [28, 30]. The phenomenon of higher rates of false positives in blood cultures is explained by the higher levels of bacterial DNA or frequent contaminants such as coagulase-negative staphylococci that are required for detection in PCR assays [9, 31].
Similar to the findings with bacterial causes of septic shock, it has been shown that delayed antimycotic treatment significantly increases mortality rates in patients with fungal infections [32, 33, 34]. The advantage of the short turnaround times involved in PCR assays thus becomes even more relevant in fungal infections, since the time taken to reach positivity in candidemia blood cultures is usually much longer than with bacteremia [35]. However, for one patient in our study with culture proven candidemia, all three PCR assays were negative. In another case, the LightCycler® SeptiFast assay was positive for Aspergillus fumigatus, but none of the other microbiological diagnostic tests or the clinical course suggested an invasive Aspergillus infection.
Other studies on the LightCycler® SeptiFast assay have documented more samples testing positive for Candida DNA than Candida positive blood cultures. In their prospective multicenter study, Westh et al. [36] observed more positive PCR-based results for Candida albicans in sepsis patients than in the corresponding blood cultures. Bloos et al. [17] published similar findings in their group of critically ill postoperative patients with severe sepsis or septic shock.
In our study focused on critically ill sepsis patients, there was some variability between the three PCR assays and the corresponding blood cultures with regards to the type of pathogen detected. Interpretation of the diagnostic validity and of the differences between the assays is limited by the small sample size.
The major logistic advantage of PCR-based techniques over blood cultures is the much faster turnaround time of these assays—6–8 h as compared to 1–3 days. However, these assays require specifically trained personnel, ideally available 24 hours a day. So even where a multiplex PCR assay is available, most hospitals only perform the assay during the day. Only very few studies have addressed the question of whether obtaining a faster result by means of multiplex PCR translates into relevant changes in clinical management and outcome. In one study, antibiotic therapy was modified according to the results of the LightCycler® SeptiFast assay, but this did not alter mortality rates [20]. Lehmann et al. [37] applied a mathematical model to the original data of a study on the LightCycler® SeptiFast assay and calculated a 2.6 % absolute reduction in mortality rate for a scenario of antibiotic treatment modification based on the PCR-based pathogen findings.
Nevertheless, it is expected that despite the current high demands on financial and personnel resources, PCR-based assays will be increasingly applied in the routine diagnostic workup of sepsis patients. However, it has to be noted that complete identification of the antibiotic resistance spectrum can currently only be achieved by blood culture. This becomes increasingly important in the context of the emerging multi-resistant bacteria. Moreover, despite PCR assays covering a broad range of sepsis-relevant pathogens, they currently do not cover them all. In our analysis, the rate of positive results observed in PCR systems increased with higher severity scores (Tab. 3) and elevated PCT levels.
In accordance with the existing literature, our results confirm that PCR assays may positively supplement blood culture results as part of the diagnostic workup of septic patients, but they should not replace blood culture at present. Combining blood culture and PCR assays could raise the detection rate of microorganisms, as shown by our research and in other recent studies [13, 16, 20]. Future studies involving a larger number of patients are required to compare different PCR systems and to further evaluate their diagnostic and prognostic validity, as well as the effect the use of these assays has on clinical management and outcome. Two large multicenter studies are currently being carried out to further investigate the validity of different multiplex PCR assays [38, 39].
References
Angus DC, Linde-Zwirble WT, Lidicker J et al (2001) Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med 29:1303–1310
Engel C, Brunkhorst FM, Bone HG et al (2007) Epidemiology of sepsis in Germany: results from a national prospective multicenter study. Intensive Care Med 33:606–618
Nobre V, Sarasin FP, Pugin J (2007) Prompt antibiotic administration and goal-directed hemodynamic support in patients with severe sepsis and septic shock. Curr Opin Crit Care 13:586–591
Garnacho-Montero J, Garcia-Garmendia JL, Barrero-Almodovar A et al (2003) Impact of adequate empirical antibiotic therapy on the outcome of patients admitted to the intensive care unit with sepsis. Crit Care Med 31(12):2742–2751
Hanon FX, Monnet DL, Sorensen TL et al (2002) Survival of patients with bacteraemia in relation to initial empirical antimicrobial treatment. Scand J Infect Dis 34(7):520–528
Kumar A, Roberts D, Wood KE et al (2006) Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med 34:1589–1596
Kluge S, Braune S, Nierhaus A et al (2012) Diagnostic value of positron emission tomography combined with computed tomography for evaluating patients with septic shock of unknown origin. J Crit Care 27(3):316.e1–316.e7
Reinhart K, Brunkhorst FM, Bone HG et al (2010) Prävention, Diagnose, Therapie und Nachsorge der Sepsis Erste Revision der S2k-Leitlinien der Deutschen Sepsis-Gesellschaft e.V. (DSG) und der Deutschen Interdisziplinären Vereinigung für Intensiv- und Notfallmedizin (DIVI). Anaesthesist 59:347–370
Pletz MW, Wellinghausen N, Welte T (2011) Will polymerase chain reaction (PCR)-based diagnostics improve outcome in septic patients? A clinical view. Intensiv Care Med 37:1069–1076
Fleig V, Brenck F, Wolff M, Weigand MA (2011) Scoring-Systeme in der Intensiv-medizin Grundlagen, Modelle, Anwendung und Grenzen. Anaesthesist 60:963–974
Mauch H, Podbielski A, Herrmann M, Kniehl E (Hrsg) (2007) MiQ—Blutkulturdiagnostik—Sepsis, Endokarditis, Katheterinfektionen, Teil I + II. ELSEVIER—Urban & Fischer, München
Witte W, Cuny C, Klare I et al (2008) Emergence and spread of antibiotic-resistant Gram-positive bacterial pathogens. Int J Med Microbiol 298(5–6):365–377. (Epub Mar 5)
Wellinghausen N, Kochem AJ, Disqué C et al (2009) Diagnosis of bacteremia in whole-blood samples by use of a commercial universal 16S rRNA gene-based PCR and Sequence Analysis. J Clin Microbiol 47:2759–2765
Cockerill FR, Wilson JW, Vetter EA et al (2004) Optimal testing parameters for blood cultures. Clin Infect Dis 38(12):1724–1730
Klouche M, Schröder U (2008) Rapid methods for diagnosis of bloodstream infections. Clin Chem Lab Med 46(7):888–908
Obara H, Aikawa N, Hasegawa N et al (2011) The role of a real-time PCR technology for rapid detection and identification of bacterial and fungal pathogens in whole-blood samples. J Infect Chemother 17(3):327–333
Bloos F, Hinder F, Becker K et al (2010) A multicenter trial to compare blood culture with polymerase chain reaction in severe human sepsis. Intensive Care Med 36:241–247
Yanagihara K, Kitagawa Y, Tomonaga M et al (2010) Evaluation of pathogen detection from clinical samples by real-time polymerase chain reaction using a sepsis pathogen DNA detection kit. Crit Care 14:R159
Lehmann LE, Hunfeld KP, Steinbrucker M et al (2010) Improved detection of blood stream pathogens by real-time PCR in severe sepsis. Intensive Care Med 36:49–56
Lodes U, Bohmeier B, Lippert H et al (2012) PCR-based rapid sepsis diagnosis effectively guides clinical treatment in patients with new onset of SIRS. Langenbecks Arch Surg 397:447–455. (Epub 2011 Nov)
Tsalik EL, Jones D, Nicholson B et al (2010) Multiplex PCR to diagnose bloodstream infections in patients admitted from the emergency department with sepsis. J Clin Microbiol 48(1):26–33
Maubon D, Hamidfar-Roy R, Courby S et al (2010) Therapeutic impact and diagnostic performance of multiplex PCR in patients with malignancies and suspected sepsis. J Infect 61(4):335–342. (Epub 2010 Jul 15)
Bravo D, Blanquer J, Tormo M et al (2011) Diagnostic accuracy and potential clinical value of the LightCycler SeptiFast assay in the management of bloodstream infections occurring in neutropenic and critically ill patients. Int J Infect Dis 15(5):e326–e331. (Epub 2011 Feb 24)
Josefson P, Strålin K, Ohlin A et al (2011) Evaluation of a commercial multiplex PCR test (SeptiFast) in the etiological diagnosis of community-onset bloodstream infections. Eur J Clin Microbiol Infect Dis 30(9):1127–1134. (Epub 2011 Mar 4)
Bloos F, Sachse S, Schmidt KH et al (2008) Nucleic acid amplification-based pathogen detection in the blood of severe sepsis patients. Crit Care 12(Suppl 5):P43
Lamoth F, Jaton K, Prodhom G et al (2010) Multiplex blood PCR in combination with blood cultures for improvement of microbiological documentation of infection in febrile neutropenia. J Clin Microbiol 48:3510–3516
Dierkes C, Ehrenstein B, Siebig S et al (2009) Clinical impact of a commercially available multiplex PCR system for rapid detection of pathogens in patients with presumed sepsis. BMC Infect Dis 9:126
Hettwer S, Wilhelm J, Schürmann M et al (2012) Microbial diagnostics in patients with presumed severe infection in the emergency department. Med Klin Intensivmed Notfmed 107:53–62
Afshari A, Schrenzel J, Leven M, Harbarth S (2012) Bench-to-bedside review: rapid molecular diagnostics for bloodstream infection—a new frontier? Crit Care 16:222
Lehmann LE, Alvarez J, Hunfeld KP et al (2009) Potential clinical utility of polymerase chain reaction in microbiological testing for sepsis. Crit Care Med 37(12):3085–3090
Casalta JP, Gouriet F, Roux V et al (2009) Evaluation of the LightCycler® SeptiFast test in the rapid etiologic diagnostic of infectious endocarditis. Eur J Clin Micrbiol Infect Dis 28:569–573
Garey KW, Rege M, Pai MP et al (2006) Time to initiation of fluconazole therapy impacts mortality in patients with candidemia: a multi-institutional study. Clin Infect Dis 43:25–31
Parkins MD, Sabuda DM, Elsayed S, Laupland KB (2007) Adequacy of empirical antifungal therapy and effect on outcome among patients with invasive Candida species infections. J Antimicrob Chemother 60:613–618
Bassetti M, Trecarichi EM, Righi E et al (2007) Incidence, riskfactors and predictors of outcome of candidemia. Survey in 2 Italian university hospitals. Diagn Microbiol Infect Dis 58:325–331
Taur Y, Cohen N, Dubnow S et al (2010) Effect of antifungal therapy timing on mortality in cancer patients with candidemia. Antimicrob Agents Chemother 54(1):184–190
Westh H, Lisby G, Breysse F et al (2009) Multiplex real-time PCR and blood culture for identification of bloodstream pathogens in patients with suspected sepsis. Clin Microbiol Infect 15:544–551
Lehmann LE, Herpichboehm B, Kost GJ et al (2010) Cost and mortality prediction using polymerase chain reaction pathogen detection in sepsis: evidence from three observational trials. Crit Care 14(5):R186
Welte T (2010) An assessment of the potential clinical utility of a new multiplex-PCR assay (VYOO®) in the management of ICU patients with sepsis. German Clinical Trials Register DRKS00000612. Intensivmed 47:463
Dark P, Dunn G, Chadwick P et al (2011) The clinical diagnostic accuracy of rapid detection of healthcare-associated bloodstream infection in intensive care using multipathogen real-time PCR technology. BMJ Open 1(1):e000181. (Epub 2011 Jun 30)
Acknowledgements
We thank G. Franke, Th. Meyer and M. Aepfelbacher from the Department of Clinical Microbiology, Virology and Hygiene who performed the microbiological studies.
Conflict of interest
On behalf of all authors, the corresponding author states the following: This study was supported by Molzym GmbH & Co. KG, Sirs-Lab GmbH and Roche Diagnostics GmbH. These companies provided test kits and instruments for PCR diagnostics, as well as full technical support.
Author information
Authors and Affiliations
Corresponding author
Additional information
J. Schreiber and A. Nierhaus contributed equally to this work.
J. Schreiber und A. Nierhaus haben zu gleichen Teilen zu dieser Arbeit beigetragen.
Rights and permissions
About this article
Cite this article
Schreiber, J., Nierhaus, A., Braune, S. et al. Comparison of three different commercial PCR assays for the detection of pathogens in critically ill sepsis patients. Med Klin Intensivmed Notfmed 108, 311–318 (2013). https://doi.org/10.1007/s00063-013-0227-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00063-013-0227-1