
Abstract
Purpose
To determine the incidence, the reasons, and the predictive factors for unanticipated admission after ambulatory surgery.
Methods
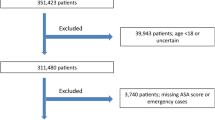
Preoperative, intraoperative, and postoperative data were collected prospectively on 15,172 consecutive ambulatory surgical patients during a 32-month period. The data were built into a statistical model, and predictive factors were identified and classified.
Results
The overall incidence of unanticipated admission was 1.42%. Admitted patients were more likely to be older, male, and ASA status II or III. Duration of anaesthesia was longer, and surgery was more likely to be completed after 3 pm. Length of stay in the Postanaesthesia Care Unit and the Ambulatory Surgery Unit was longer. Surgical reasons were cited in 38.1% of admitted patients; anaesthesia-related reasons were cited in 25%; social reasons accounted for 19.5%, and medical reasons for 17.2%. Ear, nose and throat (ENT) patients had the highest unanticipated admission rate (18.2%), followed by urology (4.8%) and chronic pain block (3.9%). Gynaecological patients had the lowest rate (0.4%). Among the predictive factors found were male, ASA status II and III, long duration of surgery, surgery finishing after 3 pm, postoperative bleeding, excessive pain, nausea and vomiting, and excessive drowsiness or dizziness.
Conclusion
Earlier operating time for certain surgical procedures, screening for proper support at home, and implementation of clinical pathways to deal aggressively with problems such as pain, nausea and vomiting should decrease the incidence of unanticipated admission.
Résumé
Objectif
Déterminer l’incidence, les raisons et les facteurs prédictifs d’une admission non prévue à la suite d’une chirurgie ambulatoire.
Méthode
Les données préopératoires, intraopératoires et postopératoires ont été recueillies pendant 32 mois de façon prospective auprès de 15 172 patients consécutifs, à la suite d’une chirurgie ambulatoire. Ces données ont été intégrées à un modèle statistique et les facteurs prédictifs ont été identifiés et classifies.
Résultats
L’incidence totale d’admission imprévue était de 1,42%. Les patients admis étaient plus susceptibles d’être âgés, de sexe mâle et d’état ASA II ou III. La durée de l’anesthésie était longue et plus susceptible de se prolonger après 15 h. Les séjours à l’unité des soins postanesthésiques et à l’unité de chirurgie ambulatoire étaient prolongés. Les raisons chirurgicales ont été invoquées pour 38,1% des patients admis; les raisons reliées à l’anesthésie pour 25%; les raisons sociales pour 19,5% et les raisons médicales pour 17,2%. Les patients d’oto-rhino-laryngologie (ORL) ont présenté le plus haut taux d’admission non planifiée (18,2%) suivis des patients d’urologie (4,8%) et de ceux qui avaient reçu un bloc thérapeutique pour douleurs chroniques (3,9%). Les patientes de gynécologie avaient le taux le plus bas (0,4%). Parmi les facteurs prédictifs identifiés, on a trouvé le sexe mâle, l’état ASA II et III, une chirurgie de durée prolongée, une chirurgie qui se termine après 15 h, les saignements postopératoires, la douleur excessive, les nausées et les vomissements, une grande somnolence et des étourdissements importants.
Conclusion
Le fait de procéder plus tôt dans la journée à certaines interventions chirurgicales, le dépistage préalable d’un soutien approprié pour le patient à domicile et la mise en application des moyens cliniques permettant de s’occuper énergiquement des effets secondaires comme la douleur et, les nausées et vomissements devraient diminuer l’incidence de l’admission non prévue.
Article PDF
Similar content being viewed by others

References
Fancourt-Smith PF, Harnstein J, Jenkins LC. Hospital admissions from the Surgical Day Care Centre of Vancouver General Hospital 1977–1987. Can J Anaesth 1990; 37: 699–704.
Levin P, Stanziola A, Hand R. Postoperative hospital retention following ambulatory surgery in a hospitalbased program. American College of Utilization Review Physicians 1990; 5: 90–4.
Gold BS, Kitz DS, Lecky JH, Neuhaus JM. Unanticipated admission to the hospital following ambulatory surgery. JAMA 1989; 262: 3008–10.
Johnson CD, Jarrett PEM. Admission to hospital after day case surgery. Ann R Coll Surg Engl 1990; 72: 225–8.
Rudkin GE, Osborne GA, Doyle CE. Assessment and selection of patients for day surgery in a public hospital. Med J Aust 1993; 158: 308–12.
Twersky RS, Abiona M, Thorne AC, et al. Admissions following ambulatory surgery: outcome in seven urban hospitals. Ambulatory Surgery 1995; 3: 141–6.
Chung FF, Chan VWS, Ong D. A postanaesthetic discharge scoring system for home readiness after ambulatory surgery. Ambulatory Surgery 1993; 1: 189–93.
Osborne GA, Rudkin GE. Outcome after day-care surgery in a major teaching hospital. Anaesth Intensive Care 1993; 21: 822–7.
Biswas TK, Leary C. Postoperative hospital admission from a day surgery unit: a seven-year retrospective survey. Anaesth Intensive Care 1992; 20: 147–50.
Meeks GR, Waller GA, Meydrech EF, Flautt FH Jr. Unscheduled hospital admission following ambulatory gynecologic surgery. Obstet Gynecol 1992; 80: 446–50.
Freeman LN, Schachat AP, Manolio TA, Enger C. Multivariate analysis of factors associated with unplanned admission in ‘outpatient’ ophthalmic surgery. Ophthalmic Surgery 1988; 19: 719–23.
Isenberg V, Apt L, Yamada S. Overnight admission of outpatient strabismus patients. Ophthalmic Surgery 1990; 21: 540–3.
Meeks GR, Meydrech EF, Bradford TH, Hollis RS. Comparison of unscheduled hospital admission following ambulatory operative laparoscopy at a teaching hospital and a community hospital. J Laparoendosc Surg 1995; 5: 7–13.
Kinnard P, Lirette R. Outpatient orthopedic surgery: a retrospective study of 1996 patients. Can J Surg 1991; 34: 363–6.
Michaloliakou C, Chung F, Sharma S. Preoperative, multimodal analgesia facilitates recovery after ambulatory laparoscopic cholecystectomy. Anesth Analg 1996; 82: 44–51.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Fortier, J., Chung, F. & Su, J. Unanticipated admission after ambulatory surgery — a prospective study. Can J Anaesth 45, 612–619 (1998). https://doi.org/10.1007/BF03012088
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03012088