
Abstract
Purpose
Mucormycosis encompasses a group of opportunistic fungal infections caused by Zygomycetes, order Mucorales. Mucormycosis can manifest as rhino-orbito-cerebral, pulmonary, gastrointestinal, cutaneous, and disseminated infections. Pulmonary mucormycosis is the second most common presentation. This manuscript characterizes the demographics, clinical presentation, diagnostic procedures, radiologic findings, therapeutic interventions, and outcome in pulmonary mucormycosis.
Methods
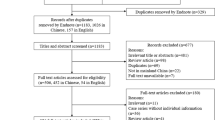
We retrospectively reviewed clinical data of 35 patients with pulmonary mucormycosis from 2000 to 2015. Microbiologic diagnosis was based on positive culture from a sterile site or findings on histopathology consistent with mucormycosis. Independent predictors of 28-day mortality were assessed using logistic regression. Survival curves were estimated using Kaplan–Meier method.
Results
There was male predominance with a mean age of 55 ± 15 years. Analysis of predisposing conditions revealed the prevailing presence of malignancy. Sixty-six percent of patients were receiving immunosuppressive agents. Common presenting clinical findings were fever, neutropenia, dyspnea, and cough. Radiologic findings included pleural effusion and nodules. All patients received medical therapy and 43% underwent additional surgical intervention. Twenty eight day mortality was 29% with concurrent bacteremia found as the sole independent predictor. Similar survival from pulmonary mucormycosis was noted over time.
Conclusions
Pulmonary mucormycosis is an opportunistic angioinvasive fungal infection. Physicians must have a high level of suspicion in immunocompromised patients with fever and respiratory symptoms refractory to antibiotics. A low threshold should be had for performing an invasive procedure to gain reliable diagnosis, as early, aggressive medical and surgical interventions are needed for successful treatment.

Similar content being viewed by others

References
Danion F, Aguilar C, Catherinot E, Alanio A, DeWolf S, Lortholary O, et al. Mucormycosis: new developments into a persistently devastating infection. Semin Respir Crit Care Med. 2015;36:692–705. doi:10.1055/s-0035-1562896.
Tedder M, Spratt JA, Anstadt MP, Hegde SS, Tedder SD, Lowe JE. Pulmonary mucormycosis: results of medical and surgical therapy. Ann Thorac Surg. 1994;57:1044–50.
Bitar D, Van Cauteren D, Lanternier F, Dannaoui E, Che D, Dromer F, et al. Increasing incidence of zygomycosis (mucormycosis), France, 1997–2006. Emerg Infect Dis. 2009;15:1395–401. doi:10.3201/eid1509.090334.
Saegeman V, Maertens J, Meersseman W, Spriet I, Verbeken E, Lagrou K. Increasing incidence of mucormycosis in University Hospital Belgium. Emerg Infect Dis. 2010;16:1456–8. doi:10.3201/eid1609.100276.
Cornely OA, Arikan-Akdagli S, Dannaoui E, Groll AH, Lagrou K, Chakrabarti A, et al. ESCMID and ECMM joint clinical guidelines for the diagnosis and management of mucormycosis 2013. Clin Microbiol Infect. 2014;20:5–26. doi:10.1111/1469-0691.12371.
Chakrabarti A, Das A, Mandal J, Shivaprakash MR, George VK, Tarai B, et al. The rising trend of invasive zygomycosis in patients with uncontrolled diabetes mellitus. Med Mycol. 2006;44:335–42. doi:10.1080/13693780500464930.
Chamilos G, Marom EM, Lewis RE, Lionakis MS, Kontoyiannis DP. Predictors of pulmonary zygomycosis versus invasive pulmonary aspergillosis in patients with cancer. Clin Infect Dis. 2005;41:60–6. doi:10.1086/430710.
Chakrabarti A, Das A, Sharma A, Panda N, Das S, Gupta KL, et al. Ten yearsʼ experience in zygomycosis at a tertiary care centre in India. J Infect. 2001;42:261–6. doi:10.1053/jinf.2001.0831.
Pagano L, Ricci P, Tonso A, Nosari A, Cudillo L, Montillo M, et al. Mucormycosis in patients with haematological malignancies: a retrospective clinical study of 37 cases. GIMEMA Infection Program (Gruppo Italiano Malattie Ematologiche Maligne dellʼAdulto). Br J Haematol. 1997;99:331–6.
McAdams HP, Rosado de Christenson M, Strollo DC, Patz EF Jr. Pulmonary mucormycosis: radiologic findings in 32 cases. AJR Am J Roentgenol. 1997;168:1541–8. doi:10.2214/ajr.168.6.9168721.
Saegeman V, Maertens J, Ectors N, Meersseman W, Lagrou K. Epidemiology of mucormycosis: review of 18 cases in a tertiary care hospital. Med Mycol. 2010;48:245–54. doi:10.1080/13693780903059477.
Hammond SP, Bialek R, Milner DA, Petschnigg EM, Baden LR, Marty FM. Molecular methods to improve diagnosis and identification of mucormycosis. J Clin Microbiol. 2011;49:2151–3. doi:10.1128/jcm.00256-11.
Alvarez E, Sutton DA, Cano J, Fothergill AW, Stchigel A, Rinaldi MG, et al. Spectrum of zygomycete species identified in clinically significant specimens in the United States. J Clin Microbiol. 2009;47:1650–6. doi:10.1128/jcm.00036-09.
Marchiori E, Zanetti G, Escuissato DL, Souza AS Jr, Meirelles GS, Fagundes J, et al. Reversed halo sign: high-resolution CT scan findings in 79 patients. Chest. 2012;141:1260–6. doi:10.1378/chest.11-1050.
Greenberg RN, Mullane K, van Burik JA, Raad I, Abzug MJ, Anstead G, et al. Posaconazole as salvage therapy for zygomycosis. Antimicrob Agents Chemother. 2006;50:126–33. doi:10.1128/aac.50.1.126-133.2006.
Marty FM, Ostrosky-Zeichner L, Cornely OA, Mullane KM, Perfect JR, Thompson GR 3rd, et al. Isavuconazole treatment for mucormycosis: a single-arm open-label trial and case-control analysis. Lancet Infect Dis. 2016;16:828–37. doi:10.1016/s1473-3099(16)00071-2.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article. This research received no grant from any funding agency in the public, commercial or non-profit sectors.
Rights and permissions
About this article

Cite this article
Lin, E., Moua, T. & Limper, A.H. Pulmonary mucormycosis: clinical features and outcomes. Infection 45, 443–448 (2017). https://doi.org/10.1007/s15010-017-0991-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-017-0991-6